
Seborrheic Keratosis of the Eyelid
Key Points at a Glance
Section titled “Key Points at a Glance”1. What is seborrheic keratosis of the eyelid?
Section titled “1. What is seborrheic keratosis of the eyelid?”Seborrheic keratosis is the most common benign eyelid tumor in middle-aged and elderly people, also called verruca senilis. It causes raised lesions due to age-related thickening or horizontal proliferation of the epidermis, and tends to enlarge over several years. An important feature is that it does not become malignant.
Epidemiology
Section titled “Epidemiology”- Among benign eyelid tumors, it accounts for 14% (9/64 eyes) by pathological diagnosis, making it the second most common tumor.
- It is considered an age-related change commonly seen in middle-aged and elderly people (mainly after the 50s).
- It is also one of the most common benign tumors on the skin of the whole body, and about 80% of people over 50 have some form of seborrheic keratosis 1).
- Ultraviolet exposure is known as an exacerbating factor 1).
- On the eyelid, it commonly occurs on the skin side from the eyelashes.
- Familial occurrence has also been reported1).
Seborrheic keratosis is a benign tumor that does not become malignant, and it will not turn into cancer even if left untreated. However, because it can clinically resemble basal cell carcinoma or malignant melanoma, histopathological examination is recommended for a definitive diagnosis. Particularly in cases of rapid growth or when the surface is hard with central ulceration, malignancy must be ruled out.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”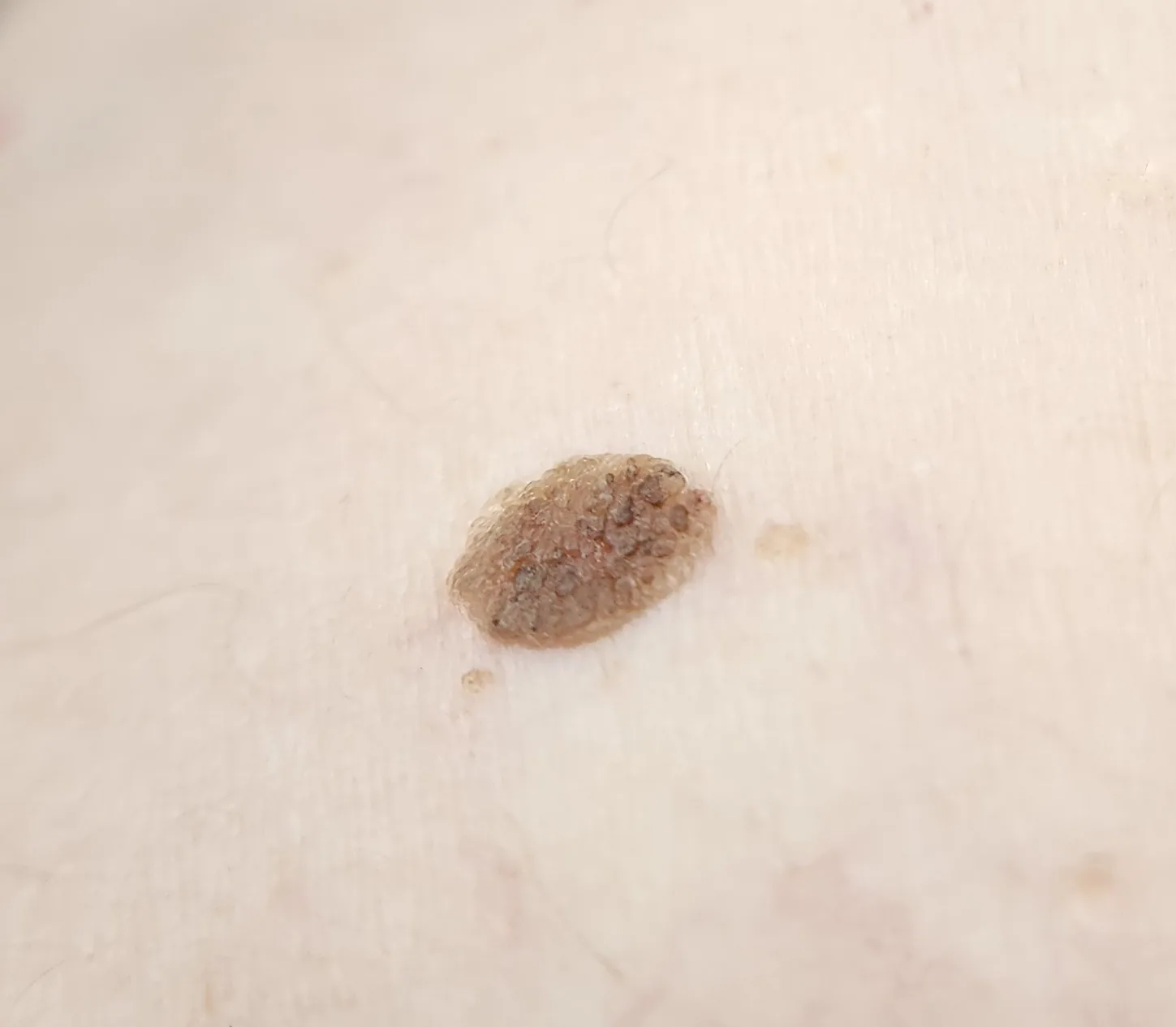
Subjective Symptoms
Section titled “Subjective Symptoms”It is often asymptomatic. The main subjective symptoms are listed below.
- Cosmetic concerns: Brown or black elevated lesions on the eyelid are often noticed as an aesthetic issue.
- Foreign body sensation: Rarely, when the tumor becomes large, mild foreign body sensation may be reported.
- Tearing and irritation: When occurring at the eyelash margin, irritative symptoms may appear.
Clinical Findings
Section titled “Clinical Findings”- Predilection site: Commonly occurs on the skin side of the eyelashes. It can also occur on the skin surface away from the eyelid margin.
- Color: Varies from light brown to black, and color changes may be present within the same lesion.
- Shape and surface characteristics: Well-demarcated. The surface may be rough and irregular due to keratinization, or glossy like a mulberry. Hyperkeratosis may cause papillary elevation.
- Hardness: The surface of the tumor is soft and fragile. This is an important distinguishing feature from basal cell carcinoma (which is hard).
- Size: Varies from a few mm to over 1 cm. It enlarges over a period of years.
Dermoscopic Findings
Section titled “Dermoscopic Findings”Observation with a dermoscope is useful as a diagnostic aid, and the following findings are characteristic 2).
- Cerebriform pattern: The surface exhibits brain-like grooves and ridges.
- Milia-like cysts: Observed as white to yellowish-white round dots.
- Comedo-like openings: Observed as brown to black round openings.
If multiple of these findings are present, seborrheic keratosis is highly likely.
For clinical differentiation, seborrheic keratosis is characterized by “well-defined borders, soft and fragile surface, and absence of central ulceration or depression.” In contrast, basal cell carcinoma shows findings such as “central ulceration, depression, pearly luster, vascular proliferation (telangiectasia), and hardness.” Cerebriform patterns and milia-like cysts on dermoscopy are characteristic of seborrheic keratosis, but differentiation may be difficult in pigmented lesions. Pathological examination is essential for a definitive diagnosis.
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”Multiple factors are involved in the development of seborrheic keratosis.
- Aging: The most significant risk factor. It is based on thickening and increased proliferation of epidermal cells with aging.
- Ultraviolet exposure: Sun exposure is involved in the onset and exacerbation 1). The eyelids are areas easily affected by sunlight.
- Genetic factors: Familial occurrence has been reported, suggesting the involvement of genetic predisposition 1).
- FGFR3 gene mutation: FGFR3 (fibroblast growth factor receptor 3) gene mutations have been reported in some seborrheic keratoses, and it has been confirmed that mutations are present even at the stage of flat lesions3).
- PIK3CA mutation: Similar to FGFR3, it is involved in the activation of proliferative signaling pathways3).
Leser-Trélat Sign
Section titled “Leser-Trélat Sign”When seborrheic keratoses appear rapidly and in large numbers over a short period, it is called the Leser-Trélat sign, which may indicate a paraneoplastic syndrome associated with internal malignancy4). Associated malignancies include gastrointestinal cancers (gastric cancer, colorectal cancer), lung cancer, breast cancer, and lymphoma. However, since seborrheic keratoses also increase with age in healthy individuals, caution is needed only in cases of rapid and multiple appearance.
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”Clinical Diagnosis
Section titled “Clinical Diagnosis”In elderly patients, it is often clinically diagnosable as a well-demarcated brown to black verrucous raised lesion. However, because there are malignant tumors with similar appearance, pathological examination is always necessary for a definitive diagnosis.
Dermoscopic findings (cerebriform pattern, pseudocysts, pseudocomedones) are useful as diagnostic aids and contribute to improved accuracy in differentiating benign from malignant lesions2).
A dermoscope (dermatoscope) is a non-invasive diagnostic aid that uses a specialized lens to magnify pigmented skin lesions. By using polarized light or immersion fluids (such as alcohol or gel), it eliminates surface light reflection and allows detailed observation of pigment structures from the epidermis to the superficial dermis. It is useful for identifying characteristic findings of seborrheic keratosis (gyriform pattern, pseudocysts, pseudocomedones) and improves differentiation from malignant melanoma and basal cell carcinoma.
Histopathological Examination
Section titled “Histopathological Examination”The definitive diagnosis of seborrheic keratosis is made by histopathological examination. The following findings are characteristic:
- Acanthosis and proliferation of spinous cells1)
- Pseudohorn cysts: Cystic structures containing keratin material are a pathological hallmark1)
- Proliferation of a mixture of basaloid cells and squamous epithelial cells
- Absence of nuclear atypia or infiltrative growth pattern distinguishes it from malignant diseases
All excised specimens must be submitted for pathological examination to confirm the exclusion of malignancy.
Differential Diagnosis
Section titled “Differential Diagnosis”| Differential Disease | Key Differentiating Features |
|---|---|
| Basal cell carcinoma | Central ulceration/depression, vascular proliferation, firm surface, pearly luster |
| Malignant melanoma | Pigment heterogeneity, rapid enlargement, irregular shape, ABCDE rule |
| Eyelid nevus (mole) | Present since childhood, flat and soft |
| Actinic keratosis | Precancerous lesion, red and rough surface, prone to crusting |
| Pigmented basal cell carcinoma | Pigmentation, pearly luster, vascular proliferation |
| Verruca vulgaris | Common in young people, HPV infection, cauliflower-like surface |
5. Standard Treatment
Section titled “5. Standard Treatment”If there are no cosmetic or functional issues, observation is possible. Treatment is performed when there is a tendency to enlarge, when differentiation from malignancy is necessary, or when the patient desires treatment.
Surgical Excision
Section titled “Surgical Excision”This is the first-line treatment. The tumor is excised along with the epidermis, serving both for definitive diagnosis and treatment.
- Ensuring safety margins: Excision at the very edge of the tumor border may lead to recurrence. Excise with sufficient safety margins.
- Management in elderly patients: Elderly patients often have excess skin, so simple closure is possible in many cases.
- Lesions involving eyelashes: If the eyelashes are involved in the tumor, manage the eyelid margin with open treatment.
- Resected specimen: Must be sent for pathological examination to confirm the presence of malignant components.
Cryotherapy
Section titled “Cryotherapy”Indicated for small to medium-sized lesions. Cryotherapy using liquid nitrogen can be performed on an outpatient basis and is minimally invasive, but the recurrence rate is slightly higher than that of excision. A disadvantage is that a definitive pathological diagnosis cannot be obtained.
Laser therapy
Section titled “Laser therapy”- CO2 laser vaporization: An excellent option for cosmetic outcomes, with minimal thermal damage to surrounding tissue 5). However, vaporized tissue is difficult to evaluate pathologically, so it is contraindicated when malignancy cannot be ruled out.
- Erbium YAG laser: Allows precise vaporization with good cosmetic results 5).
Electrocoagulation
Section titled “Electrocoagulation”An option that can be performed on an outpatient basis for small lesions 1). The tumor is cauterized by electrocoagulation under local anesthesia.
Treatment options overview
Section titled “Treatment options overview”| Treatment | Indication | Advantages | Disadvantages |
|---|---|---|---|
| Excision with epidermis | All cases (definitive diagnosis and treatment) | Pathological confirmation and margin control possible | Surgical invasiveness (under local anesthesia) |
| Cryocoagulation | Small to medium lesions | Minimally invasive, outpatient procedure | Risk of recurrence, no pathological evaluation possible |
| CO2 laser vaporization | Cases prioritizing cosmetic outcome | Precise, minimally invasive | Pathological evaluation difficult |
| Erbium YAG laser | Cases prioritizing cosmetic outcome | Precise vaporization, good cosmetic results | Pathological evaluation difficult |
| Electrocoagulation | Small lesions | Outpatient procedure | Pathological evaluation difficult due to thermal damage |
Seborrheic keratosis does not become malignant, so observation is an option if there are no cosmetic or functional problems. However, if clinical differentiation from basal cell carcinoma or malignant melanoma is difficult, or if rapid growth, color change, or ulceration is observed, biopsy or resection is recommended to rule out malignancy. Even if left untreated for a long time, regular observation is important, and if any changes occur, consultation with an ophthalmologist should not be neglected.
6. Pathophysiology and detailed pathogenesis
Section titled “6. Pathophysiology and detailed pathogenesis”Seborrheic keratosis is a raised lesion caused by thickening and horizontal proliferation of the epidermis, and is considered a type of age-related change.
Histological features
Section titled “Histological features”- Hyperkeratosis and acanthosis: Thickening of the entire epidermis and hyperkeratosis occur 1).
- Pseudohorn cysts: Cyst-like structures containing keratinous material. This is a characteristic pathological finding, corresponding to “pseudocysts” on dermoscopy 1).
- Mixture of basaloid cells and squamous cells: The tumor contains both in varying proportions, and there are several histological types such as acanthotic, adenoid, and inflamed types.
- The absence of nuclear atypia and invasive patterns is important for differentiation from malignant tumors.
Molecular mechanisms
Section titled “Molecular mechanisms”- FGFR3 (fibroblast growth factor receptor 3) gene mutations: Mutations are already present at the flat lesion stage and are associated with age and site 3). FGFR3 mutations activate cell proliferation signals and contribute to excessive proliferation of epidermal cells.
- PIK3CA mutation: Involved in activation of the PI3K/Akt/mTOR pathway and may coexist with FGFR3 mutation3).
- These somatic mutations are understood as mutations that accumulate with age and cause increased proliferation through a pathway different from malignant transformation.
Mechanism of Leser-Trélat sign
Section titled “Mechanism of Leser-Trélat sign”The association with internal malignancy in cases of rapid multiple onset is thought to be due to overproduction of tumor-derived transforming growth factor alpha (TGF-α) and insulin-like growth factor (IGF), which promote epidermal cell proliferation4). It is understood as a type of paraneoplastic syndrome.
7. Latest research and future prospects
Section titled “7. Latest research and future prospects”Topical hydrogen peroxide therapy
Section titled “Topical hydrogen peroxide therapy”Topical hydrogen peroxide 40% (Eskata®) has been approved by the FDA for seborrheic keratosis on the trunk and extremities6). In phase 3 trials, the treatment group had a significantly higher endpoint achievement rate. Application to the eyelids is currently limited due to effects on the cornea and conjunctiva, and dedicated trials are expected in the future.
AI-assisted dermoscopic diagnosis
Section titled “AI-assisted dermoscopic diagnosis”AI-assisted diagnostic systems for dermoscopic images have been developed, and improved accuracy in differentiating benign from malignant lesions has been reported7). Especially for flat pigmented lesions on the face, studies are accumulating showing discrimination accuracy comparable to that of experts. Application to the eyelids is also a future challenge.
Significance of Leser-Trélat sign as a biomarker
Section titled “Significance of Leser-Trélat sign as a biomarker”Early identification of Leser-Trélat sign in cases of rapid multiple onset of seborrheic keratosis may lead to early detection of internal malignancy4). Since the timing and pattern of the sign vary depending on the type of malignancy, development of systematic screening protocols is underway.
8. References
Section titled “8. References”- Christian Hafner, Thomas Vogt. Seborrheic keratosis. J Deutsche Derma Gesell. 2008;6(8):664-677. doi:10.1111/j.1610-0387.2008.06788.x.
- Braun RP, Rabinovitz HS, Oliviero M, Kopf AW, Saurat JH.. Dermoscopy of pigmented skin lesions. J Am Acad Dermatol. 2005;52(1):109-121. doi:10.1016/j.jaad.2001.11.001. PMID:15627088.
- Hafner C, Hartmann A, van Oers JM, Stoehr R, Zwarthoff EC, Hofstaedter F, Landthaler M, Vogt T.. FGFR3 mutations in seborrheic keratoses are already present in flat lesions and associated with age and localization. Mod Pathol. 2007;20(8):895-903. doi:10.1038/modpathol.3800837. PMID:17585316.
- Schwartz RA. Sign of Leser-Trélat. Journal of the American Academy of Dermatology. 1996;35(1):88-95. doi:10.1016/S0190-9622(96)90502-2. PMID:8682971.
- Wollina U. Erbium-YAG laser therapy — analysis of more than 1,200 treatments. Glob Dermatol. 2016;3(2):223-227. doi:10.15761/god.1000171.
- Baumann LS, Blauvelt A, Draelos ZD, et al. Safety and efficacy of hydrogen peroxide topical solution, 40% (w/w), in patients with seborrheic keratoses. Dermatol Surg. 2018;44(11):1439-1446.
- Tschandl P, Rosendahl C, Kittler H.. Dermatoscopy of flat pigmented facial lesions. J Eur Acad Dermatol Venereol. 2015;29(1):120-127. doi:10.1111/jdv.12483. PMID:24661420.