Basal cell carcinoma is a malignant tumor arising from neoplastic proliferation of basal cells of the epidermis toward the dermis. It is thought to originate from primordia of epidermal appendages. It is the most common malignant eyelid tumor, with lower proliferative capacity than other malignancies, and is a low-grade tumor that rarely metastasizes distantly. It commonly occurs on the lower eyelid, near the eyelid margin and eyelashes, and can also appear at the inner and outer canthi.
Basal cell carcinoma accounts for approximately 80% of non-melanoma skin cancers 1) and 70–80% of all cutaneous malignancies. 2) In Western countries, it comprises 82–91% of malignant eyelid tumors, 8) but in Asia, the proportion varies from 11–65% by region. 8) In a study of 536 cases in India, basal cell carcinoma accounted for 24% of malignant eyelid tumors, with a mean age of onset of 60 years. 8)
The incidence has increased by 5% over the past 10 years in Europe. 2) The mortality rate is low, less than 1%. 6) The distribution of eyelid involvement is: lower eyelid 59%, inner canthus 13–30%, upper eyelid 15–16%, and outer canthus 3–5%. 8)
QDoes basal cell carcinoma metastasize?
A
Distant metastasis is extremely rare. The metastasis rate is reported as 0.0028–0.55% 1), and the mortality rate is less than 1% 6), classifying it as a low-grade tumor. However, it is highly locally invasive and can progress to deep tissues if left untreated. Particularly, the ulcerative type and inner canthus type may infiltrate deeply into the orbit.
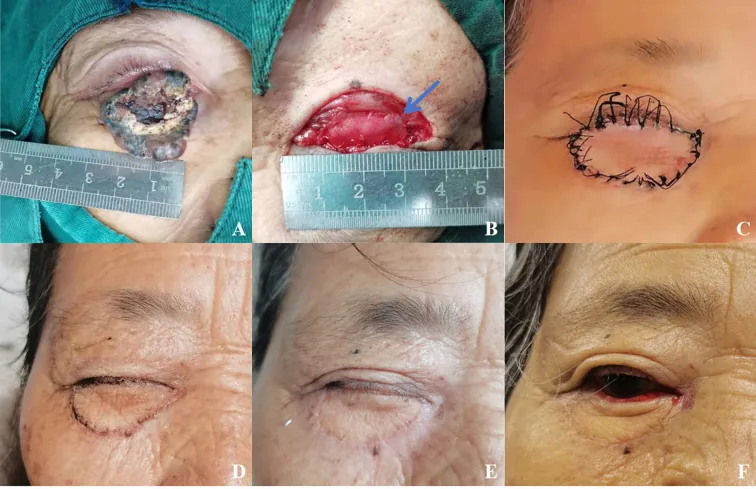
Xie L, et al. Clinical outcomes of xenogeneic acellular dermal matrix combined with full-thickness skin graft in the eyelid reconstruction following the excision of eyelid malignant tumors. Front Oncol. 2025. Figure 1. PMCID: PMC12283606. License: CC BY.
(A) Right eye basal cell carcinoma in a 68-year-old female, (B) eyelid defect and reconstruction with XADM, (C)–(F) course from 2 weeks to 6 months postoperatively. Corresponds to basal cell carcinoma discussed in section “2. Main Symptoms and Clinical Findings.”
Nodular and ulcerative types are the most common clinically. In a multicenter study in India, the nodular-ulcerative type accounted for 51% and the nodular type for 42%. 8) The median tumor diameter was reported as 12 mm and thickness as 4 mm. 8)
It is characterized by central ulceration or central depression. It often appears black or brown due to proliferation of pigment cells, but some cases are partially black or show no black color. Since it originates from the epidermis, no lesions are seen on the conjunctival surface of the eyelid.
Nodular Type
Appearance: Pearly papule/nodule. Telangiectasia on the surface.
Center: As the lesion enlarges, the center may become depressed and form an ulcer (nodular-ulcerative type).
Histological features: Characteristic tumor cell islands with peripheral palisading and clefts.
Sclerosing (Infiltrative) Type
Appearance: Scar-like flat induration. Ill-defined borders with white to yellow color.
Infiltration: Strong tendency for deep infiltration, high risk of orbital extension.
Prognosis: High recurrence rate, classified as a high-risk subtype. Morpheaform, micronodular, and basosquamous types are also high-risk.
Lesions in the medial canthus have a tendency to infiltrate deep into the orbit, so evaluation of orbital extension is particularly important. Pigmented basal cell carcinoma is found in 55% of Indians, while it is 1% in Paris and 45% in the Mediterranean, showing racial differences. 8)
Histopathologically, tumor cells are positive for CK5/6, CK14, and BerEP4, and negative for CK20. 3)
QWhich part of the eyelid is most commonly affected?
A
The lower eyelid is most common (50–66%), followed by the inner canthus (13–30%). 8) The upper eyelid accounts for 15–16%, and the outer canthus for 3–5%. The inner canthus requires attention because it tends to infiltrate deep into the orbit.
Factors that increase the risk of metastasis are listed below.
Risk factor
Notes
Tumor size (metastasis rate 25% if >5 cm, 50% if >10 cm)
The most important factor 1)
Male
Sex difference exists1)
Recurrent basal cell carcinoma
Increased risk of metastasis in recurrent cases1)
Perineural invasion
Histological finding1)
Primary tumor on scalp or ear
Increased tendency for metastasis7)
History of radiotherapy or immunosuppression
Treatment-related factors1)
QIs there a way to prevent basal cell carcinoma?
A
UV protection with sunscreen, hats, and sunglasses is effective as primary prevention. Since ultraviolet radiation (especially UVB) is the major environmental factor, daily UV protection is recommended.
Histological examination by incisional biopsy is essential for definitive diagnosis. The clinical-pathological concordance rate for basal cell carcinoma is reported to be 86%. 8)
Histologically, basophilic tumor cells proliferate forming nests of various sizes. Peripheral palisading of nuclei at the edge of the nests is characteristic. Clefts form between tumor islands and surrounding stroma. High-risk subtypes (morpheaform, infiltrative, micronodular) showing sheet-like or infiltrative growth patterns have a high risk of recurrence.
During surgery, frozen section examination is performed to confirm the absence of tumor cells at the resection margins before reconstructing the defect. However, frozen section diagnosis is not final. It is essential to confirm with permanent sections that tumor cells have been completely removed.
The AJCC 8th edition TNM classification is used for staging eyelid BCC. 9)
T1: Maximum tumor diameter ≤ 20 mm (eyelid involvement only)
T2: Maximum tumor diameter > 20 mm, or invasion of the globe or orbit
T3: Deep invasion into the orbit, facial bones, or nerves
T4: Invasion of bone or skull base
Most cases are early-stage with N0 (no regional lymph node metastasis) and M0 (no distant metastasis), and radical resection of pT1N0M0 has a good prognosis.
Basal cell carcinoma is the third most common orbital invasive malignant neoplasm (approximately 10%)3), and orbital invasion should be considered especially for lesions in the medial canthus.
Surgical excision is the basis of standard treatment. Most nodular types have relatively clear borders, and total removal is often possible with a safety margin of 1–2 mm.
The excision strategy depends on the tumor location and growth pattern.
When the lesion involves the eyelid margin: Tumor excision including the tarsal plate is necessary.
For skin lesions away from the eyelid margin without tarsal plate adhesion: Only anterior lamellar resection including the orbicularis oculi muscle is sufficient.
Ulcerative type (especially medial canthus): Borders are unclear and it grows invasively into deeper tissues. Because there is no tarsal plate barrier, it tends to invade deeply into the orbit. The deep margin must be taken generously, regardless of the apparent size on the skin surface.
Intraoperative evaluation: Confirm resection margins with frozen sections and permanent specimens.
In a multicenter study in India, wide excision was performed in 94% of cases, with a recurrence rate of 3% and an eye preservation rate of 94%. 8) Orbital exenteration was required in 5% of cases. 8)
International standards (NCCN guidelines) recommend a 4 mm clinical margin for low-risk basal cell carcinoma. 2) The 5-year recurrence rate for recurrent basal cell carcinoma is high at 11–17%, and reoperation or adjuvant therapy may be necessary. 2)
Mohs micrographic surgery (MMS) is a technique in which tissue is removed in thin layers and the entire margin of the excised tissue is evaluated intraoperatively with horizontal sections. 14) It is particularly useful for recurrent cases, high-risk subtypes, and medial canthal lesions, with a very low 5-year recurrence rate of around 1% for primary cases. 14) In Western countries, it is widely used as the standard procedure for periocular BCC. 15)
A 7-year database analysis of Mohs surgery for periocular BCC in Australia, involving over 1,000 cases, showed a recurrence rate of 1.0%, and only histologically positive margins were an independent risk factor for recurrence. 14)
Reconstruction techniques are selected according to the size of the eyelid defect after excision. 11)
Defect size
Surgical technique
≤1/4 (small defect)
Direct closure
1/4 to 1/2 (moderate defect)
Tenzel rotational flap
>1/2, large upper eyelid defect
Cutler-Beard procedure (bridge flap from lower eyelid)
>1/2, large lower eyelid defect
Hughes procedure (tarsoconjunctival flap from upper eyelid) + skin graft/flap
If orbital invasion is confirmed, orbital exenteration (including the eye) or orbital content removal may be necessary. 10) A multidisciplinary approach is important in the management of orbital invasive BCC. 13)
Radiation therapy is considered when patients are in poor general condition or elderly and cannot tolerate radical resection. Recurrence rates have been reported as 7.4% for primary basal cell carcinoma and 9.5% for recurrent basal cell carcinoma. 2) Local control rates decrease with increasing tumor size and depth of invasion, falling to 80–85%, and to 50–75% when bone or cartilage is involved. 1)
Imiquimod 5% cream: A topical immune response modifier for superficial basal cell carcinoma. Used for superficial lesions where surgical excision is difficult.
Systemic Drug Therapy
Vismodegib: Hedgehog pathway inhibitor (SMO inhibitor). Response rate 30% in metastatic basal cell carcinoma and 43% in locally advanced basal cell carcinoma (Erivance trial). 1)
Cemiplimab: PD-1 inhibitor. Approved for patients resistant or intolerant to hedgehog pathway inhibitors. Response rate 32% (phase 2 trial). 1)
QAre there treatments other than surgery?
A
For locally advanced or metastatic cases, hedgehog pathway inhibitors (Vismodegib, Sonidegib) and immune checkpoint inhibitors (Cemiplimab) are used. 1) Radiation therapy is indicated for cases where curative resection is difficult. Imiquimod 5% cream is an option for superficial basal cell carcinoma. However, surgical excision is the first choice.
QWhat is the surgical margin for eyelid basal cell carcinoma in Japan?
A
For nodular type, a safety margin of 1–2 mm is recommended; for lid margin lesions, excision including the tarsal plate; for ulcerative type, a deep margin is recommended. Intraoperative frozen section and permanent section margin assessment are important. In patients with poor general condition or elderly patients where curative resection is difficult, radiation therapy may be considered.
QWhat is Mohs surgery?
A
Mohs surgery (Mohs micrographic surgery, MMS) is a technique in which all margins of the excised tissue are evaluated pathologically during surgery using horizontal sections. 14) Compared to conventional surgical excision, it has a higher tissue preservation rate, and the 5-year recurrence rate for primary cases is very low, around 1%. It is particularly useful for recurrent cases, high-risk subtypes, and lesions at the inner canthus where margin evaluation is critical.
Abnormal activation of the hedgehog signaling pathway plays a central role in the development of basal cell carcinoma. Under normal conditions, PTCH1 (Patched 1) protein suppresses SMO (Smoothened), and GLI transcription factors remain inactive in the absence of hedgehog ligands.
In basal cell carcinoma, inactivating mutations of the PTCH gene (9q22.3) or activating mutations of SMO lead to constitutive activation of SMO. As a result, GLI transcription factors translocate to the nucleus, enhancing transcription of target genes involved in cell proliferation, survival, and angiogenesis. Abnormal activation of this pathway is confirmed in up to 90% of basal cell carcinomas. 1)4)
Tumors are thought to originate from primordia of epidermal appendages. Tumor cells form cord-like or island-like structures, and a histopathological feature is peripheral palisading. Subtypes showing sheet-like or infiltrative growth patterns (morpheaform, infiltrative, micronodular) have a high risk of recurrence and are classified as high-risk histological types. 1)6)
Ulcerative and medial canthal types have particularly strong local invasiveness. In the medial canthus, which lacks the anatomical barrier of the tarsal plate, tumors can infiltrate deep into the orbit, sometimes necessitating orbital exenteration. 10)
7. Latest Research and Future Perspectives (Investigational Reports)
Casey MC et al. (2021) reported a phase 2 trial of cemiplimab for advanced basal cell carcinoma. 1) In patients with locally advanced or metastatic basal cell carcinoma who were resistant or intolerant to hedgehog pathway inhibitors, the response rate was 32%, with a response duration exceeding one year.
Combination therapy with nivolumab (PD-1 inhibitor) and ipilimumab (CTLA-4 inhibitor) is under investigation, and future results are awaited. 1) As recent trends in eyelid tumors, the application of photodynamic therapy and topical drug therapy to eyelid BCC is also being studied. 12)
The prognosis of metastatic basal cell carcinoma by route of metastasis is shown below. The median survival for lymphatic metastasis is reported as 87 months 1)4), for hematogenous metastasis 24 months 1)4), and for bone metastasis 12 months 7). The most common metastatic site is lymph nodes (60%), followed by lung (42%), bone (10%), and skin (10%). 7) In a review of 7 cases of metastatic basal cell carcinoma originating in the head and neck, the median time to metastasis was 3 years. 4)
Ryan SE et al. (2024) reported a multidisciplinary approach including surgery, Vismodegib, and radiotherapy (25 Gy/5 fractions) for basal cell carcinoma with thoracic spine metastasis. 5) A good response to Vismodegib was confirmed, and this case highlights the efficacy of hedgehog pathway inhibitors for metastatic basal cell carcinoma.
Chemotherapy (e.g., platinum agents) is a second- or third-line option when hedgehog pathway inhibitors and immunotherapy are ineffective, and its role is limited. 1)7)
Máire‐Caitlín Casey, Roisín Pollock, Rachel H Enright, James Paul O’Neill, Neville Shine, Paul Sullivan, Fiachra T Martin, Barry O’Sullivan. Metastatic and locally aggressive BCC: Current treatment options. Clinical Case Reports. 2021;9(10). doi:10.1002/ccr3.4965.
Rokicki JP, Shaye DA, Rosenfeld E, et al. Recurrent deeply invasive basal cell carcinoma with internal carotid artery involvement. J Craniofac Surg. 2023;34(8):e731-e732.
Roque-Choque EC, Villalobos-Espinoza JR, Silva-Ocas I, Alvarado-Villacorta R, Muro-Mansilla P. Primary basal cell carcinoma of the caruncle: case report and review of the literature. Arquivos brasileiros de oftalmologia. 2024;87(3):e20220357. doi:10.5935/0004-2749.2022-0357. PMID:38537041; PMCID:PMC11627277.
Rodrigues MG, de Lucena AV, Domingues GA, de Aquino CM, Otto DY, Bandiera de Oliveira Santos A, et al. Metastatic basal cell carcinoma: Case series and literature review. Brazilian journal of otorhinolaryngology. 2025;91 Suppl 1(Suppl 1):101619. doi:10.1016/j.bjorl.2025.101619. PMID:40441022; PMCID:PMC12159677.
Ryan SE, Hall JRL, Humble R, Olinger CR. Basal Cell Carcinoma With Metastasis to the Thoracic Spine: An Uncommon Case Report and Review of the Literature. Journal of the American Academy of Orthopaedic Surgeons. Global research & reviews. 2024;8(2). doi:10.5435/JAAOSGlobal-D-23-00214. PMID:38380962; PMCID:PMC10881082.
Lise Mayrin Økland Thunestvedt, Lars Helgeland, Ingeborg Margrethe Bachmann, Åsa Karlsdottir, Torjan Magne Haslerud, Håkon Reikvam. Basosquamous Basal Cell Carcinoma with Bone Marrow Metastasis. Current Oncology. 2022;29(4):2193-2198. doi:10.3390/curroncol29040178.
Gokul Krishnan, Karthik Udupa, Ruchee Khanna. A Case of Basal Cell Carcinoma With Metastasis to the Pelvic Bone. Cureus. 2022. doi:10.7759/cureus.30305.
Swathi Kaliki, Nandini Bothra, Kavya Madhuri Bejjanki, Arpita Nayak, George Ramappa, Ashik Mohamed, Tarjani Vivek Dave, Mohammad Javed Ali, et al. Malignant Eyelid Tumors in India: A Study of 536 Asian Indian Patients. Ocul Oncol Pathol. 2018;5(3):210-219. doi:10.1159/000491549.
Xu S, Sagiv O, Rubin ML, et al. Validation study of the AJCC Cancer Staging Manual, Eighth Edition, staging system for eyelid and periocular squamous cell carcinoma. JAMA Ophthalmol. 2019 May 1;137(5):537-542. doi:10.1001/jamaophthalmol.2019.0238. PMID:30869769; PMCID:PMC6512305.
Leibovitch I, McNab A, Sullivan T, Davis G, Selva D.. Orbital invasion by periocular basal cell carcinoma. Ophthalmology. 2005;112(4):717-723. doi:10.1016/j.ophtha.2004.11.036. PMID:15808267.
Subramanian N.. Reconstructions of eyelid defects. Indian J Plast Surg. 2011;44(1):5-13. doi:10.4103/0970-0358.81437. PMID:21713158; PMCID:PMC3111123.
Silverman N, Shinder R. What’s new in eyelid tumors. Asia Pac J Ophthalmol (Phila). 2017;6(2):143-148. doi:10.22608/apo.201701.
Sun MT, Wu A, Figueira E, Huilgol S, Selva D.. Management of periorbital basal cell carcinoma with orbital invasion. Future Oncol. 2015;11(22):3003-3010. doi:10.2217/fon.15.190. PMID:26437207.
Malhotra R, Huilgol SC, Huynh NT, Selva D.. The Australian Mohs database, part I: periocular basal cell carcinoma experience over 7 years. Ophthalmology. 2004;111(4):624-630. doi:10.1016/j.ophtha.2003.12.003. PMID:15051192.
Ho SF, Brown L, Bamford M, Sampath R, Burns J.. 5 years review of periocular basal cell carcinoma and proposed follow-up protocol. Eye (Lond). 2013;27(1):78-83. doi:10.1038/eye.2012.230. PMID:23154501; PMCID:PMC3545370.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.