
Conjunctival Papilloma
1. What is conjunctival papilloma?
Section titled “1. What is conjunctival papilloma?”Conjunctival papilloma is a benign epithelial tumor of the conjunctiva caused by human papillomavirus (HPV) infection. Tumor cells proliferate like leaves on a branch of tumor vessels, forming a pink, cauliflower-shaped mass.
Classification
Section titled “Classification”Morphologically, it is broadly divided into the following two types.
- Exophytic type: A typical form that grows outward from the conjunctival surface via a thin vascular stalk.
- Sessile type: Develops with a broad base and may be difficult to distinguish from conjunctival squamous cell carcinoma.
Epidemiology
Section titled “Epidemiology”It is a relatively common disease among benign conjunctival tumors. It often occurs from young to middle-aged adults. HPV infection is involved in the development of many cases, and it can be multiple. In immunocompromised states, it tends to be multiple and recurrent.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”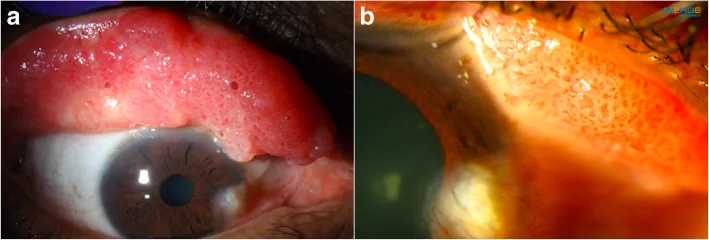
Subjective Symptoms
Section titled “Subjective Symptoms”- Foreign body sensation/discomfort: Caused by mechanical irritation from the mass.
- Redness: Conjunctival hyperemia derived from tumor vessels.
- Contact lens intolerance: Large sessile lesions may make wearing contact lenses difficult.
- Asymptomatic: Small lesions may be asymptomatic.
Clinical Findings (Findings Confirmed by Physician Examination)
Section titled “Clinical Findings (Findings Confirmed by Physician Examination)”Typical pedunculated lesions appear as pinkish (reddish) cauliflower-like masses attached to the conjunctival surface by a thin vascular stalk. The surface is irregular and highly vascularized, and multiple lesions may occur.
Sessile types show broad-based growth. In the upper tarsal conjunctiva, they present as multiple giant papillary hypertrophic lesions, sometimes with a cauliflower-like appearance with central necrosis 1). This form can be clinically difficult to distinguish from giant papillary conjunctivitis, and cases have been reported in contact lens wearers 1).
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”HPV Type Involvement
Section titled “HPV Type Involvement”- HPV types 6 and 11 (low-risk types): Major causative viruses of benign papilloma. Low risk of malignant transformation.
- HPV types 16 and 18 (high-risk types): Rarely involved and carry a risk of malignant transformation.
Risk Factors
Section titled “Risk Factors”- HPV infection: Possible routes include sexual contact, hand-to-eye contact, and iatrogenic transmission.
- Immunosuppression: Systemic immune deficiency increases the likelihood of multiple or recurrent lesions.
- Children and young adults: Predilection for the inferior fornix and bulbar conjunctiva has been reported.
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”Diagnostic Points
Section titled “Diagnostic Points”Slit-lamp microscopy is used to observe the morphology, presence of a vascular stalk, and borders of the mass. In pedunculated lesions, identification of a thin vascular stalk aids diagnosis.
Histopathological examination is essential for definitive diagnosis. Clinical differentiation between conjunctival papilloma and conjunctival squamous cell carcinoma can be difficult, making histological diagnosis indispensable.
Pathological Findings
Section titled “Pathological Findings”Histologically, acanthotic proliferative epithelium with little keratinization proliferates along papillary projections with blood vessels. Cellular atypia is usually absent.
Differential Diagnosis
Section titled “Differential Diagnosis”- Conjunctival squamous cell carcinoma: Characterized by broad-based growth and corkscrew tumor vessels, lacking a pedunculated vascular stalk.
- Conjunctival nevus: Often associated with pigmentation (melanin).
- Pyogenic granuloma: History of inflammation such as chalazion or post-surgery, with rapid growth.
- Giant papillary conjunctivitis: Common in contact lens wearers. Biopsy may be needed to differentiate from sessile papilloma 1).
The most important clinical distinguishing feature is the attachment pattern of the tumor. Papilloma shows a pedunculated growth with a thin vascular stalk from the conjunctival surface, whereas squamous cell carcinoma grows with a broad base and lacks a vascular stalk. However, sessile papilloma may present with broad-based growth, making clinical differentiation difficult. In such cases, histopathological examination is essential for definitive diagnosis.
5. Standard Treatment
Section titled “5. Standard Treatment”Surgical Treatment (First Choice)
Section titled “Surgical Treatment (First Choice)”Complete excision including the tumor base is the first choice. Since simple excision alone has a high recurrence rate, two cycles of cryotherapy (freeze and thaw) are added to the resection margins.
Treatment flow:
- Excision including the tumor base (including the vascular stalk from the base)
- Apply two cycles of cryotherapy (freeze and thaw) to the resection margins
- Submit the excised specimen for histopathological examination (to rule out squamous cell carcinoma)
Treatment of Recurrent Cases
Section titled “Treatment of Recurrent Cases”For recurrence after simple excision, consider the following:
- Re-excision + cryocoagulation: Repeat surgical excision of recurrent lesions
- Mitomycin C (MMC) eye drops: Reported as off-label use
- Interferon alpha eye drops: May be used as topical immunotherapy
- Oral cimetidine (H2 receptor antagonist): Immunomodulatory effects on HPV-related papillomas have been reported. A case of a 48-year-old woman with sessile papilloma who received oral cimetidine after surgery and showed no recurrence during 3 months of follow-up has been reported1)
Recurrence is relatively common. It is thought to be due to residual HPV virus around the resection margin, which is why simple excision alone tends to recur. To prevent recurrence, excision including the tumor base and two cycles of cryocoagulation (freeze and thaw) are important. Recurrence is particularly common in immunocompromised states.
6. Pathophysiology and Detailed Pathogenesis
Section titled “6. Pathophysiology and Detailed Pathogenesis”Mechanism of Epithelial Proliferation by HPV
Section titled “Mechanism of Epithelial Proliferation by HPV”HPV (mainly types 6 and 11) infects squamous epithelial cells, and viral DNA proliferates in the nucleus. The E6 and E7 proteins encoded by the virus interfere with host cell growth regulators (such as p53 and Rb), causing abnormal proliferation of epithelial cells.
As a result, tumor cells proliferate in a leaf-like pattern along tumor blood vessels, forming papillary projections. This growth pattern leads to the clinical cauliflower-like appearance.
Differences Between Pedunculated and Sessile Types
Section titled “Differences Between Pedunculated and Sessile Types”In the pedunculated type, papillary growth occurs through a thin vascular stalk. In contrast, the sessile type shows a broad-based horizontal growth pattern, morphologically similar to the broad-based growth of squamous cell carcinoma. Even in the sessile type, the basement membrane is preserved, which is an essential difference from malignant tumors.
High-risk HPV types and malignant transformation
Section titled “High-risk HPV types and malignant transformation”Common types 6 and 11 are low-risk types and follow a benign course. Rarely, high-risk HPV types (16 and 18) may be involved, theoretically posing a risk of malignant transformation. In such cases, definitive diagnosis is made by histopathological examination.
7. References
Section titled “7. References”- Chang KL, Yeh SI. Sessile Papilloma Mimicking Giant Papillary Conjunctivitis. Ophthalmology. 2025;132(4):e78. doi:10.1016/j.ophtha.2024.07.010. PMID:39066768.
- Liu Z, Lin Y. Conjunctival Papilloma. N Engl J Med. 2024;391(3):259. PMID: 39018535.
- Hsu CJ, Chang C, Huang YH. Successfully Treated Giant Conjunctival Papilloma. Ophthalmology. 2023;130(12):1341. PMID: 36681593.