Eyelid sebaceous carcinoma (SGC) is a highly malignant tumor arising from the sebaceous glands of the eyelid—the meibomian glands, Zeis glands, and glands of the caruncle. It is considered one of the most important malignant tumors of the eyelid. The distribution of origin is 92% from meibomian glands, 6% from Zeis glands, and 2% from the caruncle2). Since the upper eyelid contains about 50 meibomian glands and the lower eyelid about 25, it occurs more frequently in the upper eyelid. It primarily occurs after the fifth decade of life, is slightly more common in women, and metastasis or recurrence occurs in several to 20% of cases. It is a poor-prognosis disease that can sometimes be fatal.
The disease is positioned very differently in Western countries and East Asia. Among all malignant eyelid tumors, basal cell carcinoma accounts for 80–95% in Western countries, while sebaceous carcinoma accounts for only 1–3%1). In contrast, the proportion of sebaceous carcinoma is significantly higher in Asian populations.
Region/Population
Proportion of sebaceous carcinoma
Western countries
1–3%1)
India (536 cases)
53%1)
China (1,086 cases)
32%1)
Japan (38 cases)
29%1)
In Asians with eyelid malignant tumors, the probability that it is sebaceous carcinoma reaches 6.21 times (range 3.8–10.1) that of non-Asians 1). However, the “incidence” of sebaceous carcinoma itself is higher in Caucasians (2.03 per million) than in Asian/Pacific populations (1.07 per million). Because basal cell carcinoma is relatively less common in Asians, the proportion of sebaceous carcinoma among all malignant tumors appears higher.
The average age of onset is reported as 58 years in Indian populations and 57–72 years overall 1). In addition to the eyelid, 25% of cases may occur in the head and neck, other skin sites, or the genitalia.
This is an autosomal dominant genetic disorder that combines sebaceous tumors with visceral malignancies (gastrointestinal, endometrial, urological). It is caused by mutations in DNA mismatch repair genes (MLH1, MSH2, MSH6), and 24% of patients with Muir–Torre syndrome develop sebaceous carcinoma. When diagnosing sebaceous carcinoma, it is advisable to also inquire about family history and gastrointestinal symptoms.
QWhen an eyelid mass is diagnosed as sebaceous carcinoma, is it necessary to suspect the presence of other cancers?
A
The possibility of Muir-Torre syndrome should be considered. Muir-Torre syndrome is a genetic disorder characterized by sebaceous tumors and internal malignancies such as colorectal cancer. If loss of expression is observed on immunohistochemical staining for MLH1, MSH2, and MSH6, referral to a gastroenterologist or other specialist is recommended. When sebaceous carcinoma or sebaceous adenoma is found, family history and gastrointestinal symptoms should always be elicited.
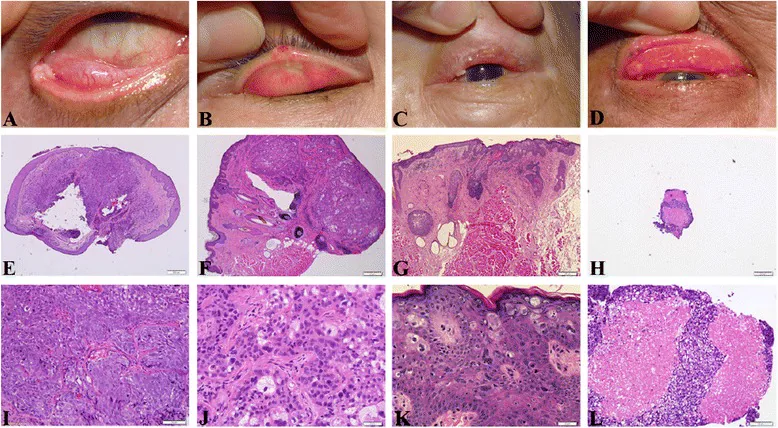
Tsai YJ, Wu SY, Huang HY, et al. Expression of retinoic acid-binding proteins and retinoic acid receptors in sebaceous cell carcinoma of the eyelids. BMC Ophthalmol. 2015;15:142. Figure 1. PMID: 26503156; PMCID: PMC4623897; DOI: 10.1186/s12886-015-0145-5. License: CC BY.
Preoperative clinical images (a–d) and hematoxylin and eosin staining (e–l) of eyelid sebaceous carcinoma (SeCC). (a) Granuloma-like mass arising from the lower eyelid tarsus; (b) small ulcerative nodule on the right upper eyelid; (c) diffuse lesion with indistinct margins resembling blepharitis; (d) advanced tumor infiltrating the entire tarsus. These correspond to eyelid nodules and masquerade syndrome discussed in the section “2. Main symptoms and clinical findings.”
Yellowish nodular mass: Characterized by a yellow appearance due to lipids within tumor cells. Commonly occurs at the upper eyelid margin, with an irregular surface and fragile tumor vessels prone to bleeding.
Observation by eyelid eversion: It is important to evert the eyelid and also examine the conjunctival side.
Diffuse type (7%)
Intraepithelial infiltration without mass formation: A type that spreads thinly from the meibomian gland opening to the eyelid margin skin or palpebral conjunctiva. This type is most often diagnosed late.
Eyelash loss (madarosis): One of the characteristic findings of the diffuse type. Always check as a sign of malignancy or severe inflammation.
The tumor occurs in the upper eyelid in 59% of cases, lower eyelid 29%, medial canthus 3%, and lateral canthus 2% 1).
Importance of madarosis: When malignant tumors such as sebaceous carcinoma or severe inflammation are present at the eyelid margin, eyelashes may fall out. If madarosis is observed, carefully examine the surrounding area for causative lesions, and consider biopsy or consultation with a tumor specialist for lesions suspicious for malignancy.
Pagetoid spread: A characteristic pattern where tumor cells proliferate and spread in a sheet-like manner within the bulbar and palpebral conjunctival epithelium away from the main lesion. It presents with fireworks-like tumor vessels and tumor cell proliferation covering the entire palpebral conjunctiva, and may form skip lesions.
QWhy is sebaceous carcinoma called the great masquerader?
A
This is because clinical diagnosis is extremely difficult due to its similarity to multiple diseases such as chalazion, blepharitis, and basal cell carcinoma. Nodular lesions are easily mistaken for chalazion, and the diffuse type resembles pagetoid spread in blepharitis. For recurrent chalazion that requires repeated incisions, sebaceous carcinoma should always be considered, and curettage specimens must be submitted for pathological examination.
Advanced age: Median age at onset is 57–72 years. Aging is a major risk factor.
Sex difference: Sebaceous carcinoma of the eyelid is slightly more common in women (male-to-female ratio 1:1.5)1).
Upper eyelid predominance: Due to the higher number of meibomian glands (approximately 50 in the upper eyelid vs. 25 in the lower eyelid).
History of periorbital radiation therapy: This is a risk factor even in young individuals.
Immunosuppression: Immunosuppressed states such as after solid organ transplantation or lymphoma may also be associated.
Muir-Torre syndrome: Mutations in DNA mismatch repair genes (MLH1, MSH2, MSH6).
Tumor size: Tumors larger than 15 mm increase the risk of regional lymph node metastasis. Preoperative CT/MRI evaluation for metastasis is essential.
QIs it true that sebaceous carcinoma is more common in Asians?
A
In Asians with eyelid malignancies, the probability of sebaceous carcinoma is 6.21 times higher than in non-Asians 1). However, this refers to relative proportions; the incidence rate (per population) of sebaceous carcinoma itself is higher in Caucasians (2.03 per million) than in Asians/Pacific Islanders (1.07 per million). Because basal cell carcinoma is less common in Asians, the proportion of sebaceous carcinoma appears relatively higher.
Having a high index of suspicion is most important. Actively suspect sebaceous carcinoma in the following cases.
Atypical or recurrent chalazion (repeated recurrence after incision)
Chronic blepharitis or persistent blepharoconjunctivitis unresponsive to treatment
Yellowish thickening or yellow mass of the eyelid
Eyelid lesion with loss of eyelashes
Even if it appears to be a chalazion, always submit the curettage material for pathological examination. In some cases, the presence or absence of improvement with antibiotic eye ointment can help differentiate pagetoid spread from blepharitis.
Excisional biopsy of the primary lesion: Perform a wide excisional biopsy, mark the margins, and submit to pathology.
Conjunctival mapping biopsy: To determine the extent of the lesion, perform multiple biopsies from the palpebral and bulbar conjunctiva in all four quadrants of both eyelids. This is essential for determining the extent of pagetoid spread.
If sebaceous carcinoma is suspected, the following imaging tests are performed to evaluate metastasis and invasion.
Head and neck CT/MRI: Essential when tumor size exceeds 15 mm due to increased risk of regional lymph node metastasis. Used to confirm regional lymph node metastasis and distant metastasis.
Orbital CT/MRI: Evaluates intraorbital extension when deep invasion is suspected.
Tumors are classified as T1 to T4 based on tumor size and eyelid/orbital invasion2).
T category
Definition
T1
Tumor longest diameter ≤10 mm
T2
Tumor longest diameter >10 to 20 mm
T3
Tumor longest diameter >20 mm
T4
Invasion into orbit, paranasal sinuses, etc.
In the 8th edition, compared to the 7th edition, the definition of T1 has been expanded (from ≤5 mm to ≤10 mm), and it has been shown that downstaging occurs2).
Histologically, basophilic tumor cells proliferate in nests, with marked atypia and pleomorphism, and characteristic intracytoplasmic lipid droplets (appearing as clear vacuoles on H&E staining). In poorly differentiated cases, lipid droplets may be inconspicuous, and the tumor may be misdiagnosed as squamous cell carcinoma. When arising from the tarsal plate, the presence of even a few intracytoplasmic lipid droplets is a key finding for diagnosing sebaceous carcinoma.
Standard immunohistochemical markers are listed below.
Marker
Characteristic
Adipophilin
Intracellular lipid droplet-associated protein. Highly sensitive and practical for sebaceous differentiation 3)
Androgen receptor
Generally positive in sebaceous carcinoma of the eyelid
Epithelial membrane antigen (EMA)
Positive
Muir-Torre syndrome screening: Check for loss of expression of MLH1, MSH2, and MSH6 by immunohistochemical staining.
When sebaceous gland tumors (sebaceous carcinoma, sebaceous adenoma, etc.) are combined with internal malignancies (especially colorectal cancer), Muir-Torre syndrome should be suspected. If loss of expression of MLH1, MSH2, or MSH6 is confirmed by immunohistochemical staining of pathological tissue specimens, referral to gastroenterology or gynecology for further evaluation is recommended. When sebaceous carcinoma is observed, a family history should also be obtained, keeping in mind that it is an autosomal dominant genetic disorder.
For localized eyelid lesions, excision with a safety margin of 3 mm or more is performed. Intraoperative margin assessment using frozen sections is desirable.
Reconstruction strategy based on the extent of tarsal defect:
Defect ≤1/3: Reconstruction possible with simple closure or local flap.
Defect >1/3: Reconstruct the anterior lamella (skin and orbicularis muscle) and posterior lamella (tarsus and conjunctiva) separately.
Posterior lamella reconstruction tissue: Use autologous tissue such as hard palate with mucosa, nasal septal cartilage, ear cartilage + labial mucosa.
When extensive full-thickness eyelid resection is required: Transplant from the opposing or contralateral healthy eyelid using the Switch flap method or Cutler-Beard method.
In Western countries, Mohs micrographic surgery or complete peripheral and deep margin assessment (CCPDMA) is a method of excising tissue while evaluating all margins, which is expected to reduce the rate of positive margins.
Topical antineoplastic eye drops (management of pagetoid spread)
When pagetoid spread is confined to the epithelium, topical antineoplastic eye drops may allow preservation of the eyeball. If the lesion invades beyond the basement membrane, eye drop treatment is ineffective.
Mitomycin C (MMC) eye drops:
0.04% ophthalmic solution, 4 times daily
Administer 2–3 cycles of 1 week on, 1 week off
5-Fluorouracil (5-FU) eye drops:
1% ophthalmic solution, 4 times daily
Administer eye drops for 2–4 days followed by 1 month off, repeating for 2–6 cycles
This is performed in cases of orbital invasion, large deeply invasive lesions, or extensive bulbar conjunctival involvement. The reported rates of exenteration by AJCC stage are T1 3%, T2 3%, T3 8%, and T4 63%2).
Sebaceous carcinoma is radiosensitive and is used for cases where radical resection is difficult or as postoperative adjuvant therapy.
External beam radiation therapy (55–66 Gy): Considered effective for local control, but the optimal dose has not been established.
Hata (2012) reported a 5-year local progression-free rate of 100% in 13 cases4).
If regional lymph node metastasis occurs, neck dissection + postoperative chemotherapy + radiation therapy is performed2).
QWhat safety margin is required for surgery of sebaceous carcinoma?
A
Resection with a safety margin of at least 3 mm is common. Intraoperative margin assessment using frozen sections is performed, and additional resection is done if margins are positive. If the tarsal plate defect is one-third or less, reconstruction with simple closure or local flap is possible; otherwise, the anterior and posterior lamellae are reconstructed separately. For T4 tumors or cases with orbital invasion, orbital exenteration is considered.
Sebaceous carcinoma is a malignant tumor arising from the glandular epithelium of sebaceous glands. The reported distribution of origin sites is 92% from Meibomian glands, 6% from Zeis glands, and 2% from the caruncle 2).
Histologically, sebaceous cells (lipid-rich cells with vacuolated cytoplasm) and undifferentiated basaloid cells are mixed, with differentiation ranging from well-differentiated to poorly differentiated. The lipids within tumor cells give a yellowish macroscopic appearance. When poorly differentiated, histological differentiation from squamous cell carcinoma can be difficult, but the presence of intracytoplasmic lipid droplets, even in small numbers, within a tarsal-based tumor supports a diagnosis of sebaceous carcinoma.
Mechanism of pagetoid spread: A pattern in which malignant cells individually migrate and proliferate in the epithelium—palpebral conjunctiva, bulbar conjunctiva, and skin—at sites distant from the main tumor. Skip lesions may form, and tumor cells can be present in areas that appear grossly normal. Therefore, mapping biopsy of the conjunctiva to assess the extent of spread is essential for treatment.
Molecular mechanism of Muir–Torre syndrome: An autosomal dominant genetic disorder caused by mutations in DNA mismatch repair genes (MLH1, MSH2, MSH6, PMS2). These mutations lead to loss of repair function for DNA replication errors, resulting in accumulation of mutations in tumor suppressor genes and development of sebaceous neoplasms.
Prognostic factors: Tumor size >15 mm increases the risk of regional lymph node metastasis. Cases with pagetoid spread or orbital invasion tend to have a poor prognosis, and metastasis-related death can occur.
7. Latest research and future perspectives (reports at the research stage)
Morawala (2023) examined the AJCC 8th edition T classification in 119 cases of sebaceous carcinoma and showed that the T classification is useful for prognosis prediction 2). The hazard ratio for lymph node metastasis of T4 tumors was 2.38, for distant metastasis was 4.30, and for metastasis-related death was 6.62. In the 8th edition, the definition of T1 was changed from ≤5 mm in the 7th edition to ≤10 mm, and downstaging was confirmed.
Li & Finger (2021) treated T2bN0M0 orbital sebaceous carcinoma with resection + cryotherapy + ultra-thick amniotic membrane transplantation followed by high-dose-rate brachytherapy (2,000 cGy/5 fractions) + electron beam external beam radiotherapy (36 Gy/20 fractions), totaling 56 Gy 5). At 1 year, visual acuity was 20/20, with no radiation retinopathy or optic neuropathy. However, cervical lymph node metastasis occurred.
Radiation therapy combined with hydrogen peroxide-impregnated gauze
Adachi (2022) treated a 97-year-old patient with inoperable preauricular sebaceous carcinoma using 60 Gy/30 fr electron beam therapy combined with hydrogen peroxide-impregnated gauze 4). At 8 months, macroscopic complete remission was achieved. The only adverse event was Grade 2 radiation dermatitis. A radiosensitizing effect of hydrogen peroxide is suggested, but this is a report of a small number of cases, and further validation is needed.
Kaliki S, Bothra N, Bejjanki KM, Nayak A, Ramappa G, Mohamed A, et al. Malignant Eyelid Tumors in India: A Study of 536 Asian Indian Patients. Ocular oncology and pathology. 2019;5(3):210-219. doi:10.1159/000491549. PMID:31049330; PMCID:PMC6489076.
Morawala A, Mohamed A, Krishnamurthy A, Jajapuram SD, Kaliki S. Sebaceous gland carcinoma: analysis based on the 8(th) edition of American Joint Cancer Committee classification. Eye (Lond). 2023;37(4):714-719. doi:10.1038/s41433-022-02025-2. PMID:35347292; PMCID:PMC9998849.
Ramachandran V, Tumyan G, Loya A, Treat K, Vrcek I. Sebaceous Carcinoma Masquerading As Orbital Cellulitis. Cureus. 2022;14(2):e22288. doi:10.7759/cureus.22288. PMID:35350510; PMCID:PMC8933264.
Adachi A, Oike T, Tamura M, Ota N, Ohno T. Radiotherapy With Hydrogen Peroxide-Soaked Gauze for Preauricular Sebaceous Carcinoma. Cureus. 2022;14(7):e27464. doi:10.7759/cureus.27464. PMID:35923494; PMCID:PMC9339371.
Li F, Stewart RD, Finger PT. Interstitial Brachytherapy for Orbital Sebaceous Carcinoma. Ophthalmic plastic and reconstructive surgery. 2021;37(6):e215-e217. doi:10.1097/IOP.0000000000002031. PMID:34314398; PMCID:PMC8565506.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.