
Metastatic Choroidal Tumor
Key Points at a Glance
Section titled “Key Points at a Glance”1. What is Metastatic Choroidal Tumor?
Section titled “1. What is Metastatic Choroidal Tumor?”Malignant tumors arising in various organs throughout the body can metastasize to the eye. The most common site of intraocular metastasis is the uveal tissue, particularly the choroid. Metastasis to the iris or ciliary body is rare.
The choroid is the tissue with the highest blood flow within the eye, providing an anatomical background that makes it easy for tumor cells carried via the bloodstream to be trapped. Metastatic lesions commonly occur in the posterior pole and may be single or multiple. Bilateral metastasis is seen in about one-quarter of cases.
The primary site distribution differs by sex. In men, the most common primary site is lung cancer, while in women, it is breast cancer. Metastases from kidney cancer, gastrointestinal cancer, and prostate cancer have also been reported. In breast cancer, uveal metastasis may occur after a long interval following treatment of the primary tumor.
Frequency by primary site (sex differences)
Section titled “Frequency by primary site (sex differences)”| Sex | Most common primary site | Other primary sites |
|---|---|---|
| Male | Lung cancer | Kidney cancer, gastrointestinal cancer, prostate cancer |
| Female | Breast cancer | Lung cancer, kidney cancer, gastrointestinal cancer |
Differential diagnosis from the three major choroidal tumors
Section titled “Differential diagnosis from the three major choroidal tumors”Metastatic choroidal tumor has a distinctive appearance among the three major tumors that occur in the choroid (malignant melanoma, hemangioma, and metastatic tumor).
| Malignant melanoma | Hemangioma | Metastatic tumor | |
|---|---|---|---|
| Color | Black, gray, brown | Orange-red | Yellow-white |
| Shape | Dome-shaped | Fusiform | Plate-like |
| Retinal detachment | None to moderate | None to mild | Marked |
| Growth | Relatively slow | None | Rapid |
In men, lung cancer is the most common source of metastasis, while in women, breast cancer is the most common. Metastases from kidney cancer, gastrointestinal cancer, and prostate cancer have also been reported. Bilateral eye metastases occur in about one-quarter of cases. In breast cancer, intraocular metastasis may be discovered long after treatment of the primary tumor.
2. Main symptoms and clinical findings
Section titled “2. Main symptoms and clinical findings”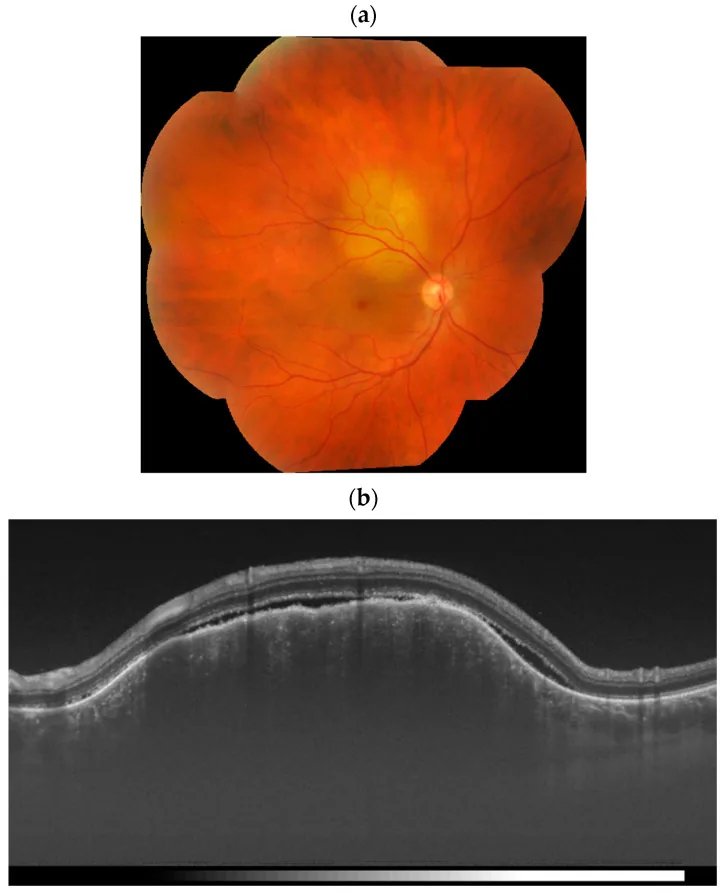
Subjective symptoms
Section titled “Subjective symptoms”In choroidal metastasis, the following symptoms occur due to serous retinal detachment associated with the tumor:
- Visual field defect: Visual field loss corresponding to the area of retinal detachment.
- Visual acuity loss: Marked decrease when the macula is involved.
- Metamorphopsia: Objects appear distorted, due to retinal displacement.
Iris metastasis presents with different symptoms.
- Blurred vision and visual acuity loss: Caused by bleeding from the tumor.
- Anterior chamber flare: Inflammatory cells from the iris tumor spill into the anterior chamber.
Clinical findings (choroidal metastasis)
Section titled “Clinical findings (choroidal metastasis)”On fundus examination, it is found as a relatively flat, well-demarcated yellowish-white lesion. As it progresses, it becomes elevated and may be difficult to distinguish from other choroidal tumors. Prominent serous retinal detachment is present directly over or around the lesion.
The reason it takes a plate-like form is that tumor cells are trapped in the choriocapillaris and grow laterally along the vessels. This also damages the retinal pigment epithelium (RPE) cells, leading to exudative (serous) retinal detachment.
Fluorescein Angiography (FA) Findings
Section titled “Fluorescein Angiography (FA) Findings”- Early to mid phase: Granular hyperfluorescence within the tumor.
- Late phase: Transition to diffuse irregular hyperfluorescence.
- Peritumoral area: A band-like hypofluorescent rim may be observed.
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”Mechanism of Metastasis
Section titled “Mechanism of Metastasis”Tumor cells from the primary site disseminate hematogenously throughout the body and reach the eye. Within the eye, the choroid has the richest blood flow, making it a common site for tumor cell entrapment and metastasis.
After being trapped in the capillary network of the choriocapillaris, tumor cells proliferate locally. This process damages the RPE and causes exudative retinal detachment.
Main Risk Factors
Section titled “Main Risk Factors”- History of malignancy: Particularly lung cancer, breast cancer, renal cancer, gastrointestinal cancer, and prostate cancer require attention.
- Advanced systemic malignancy: Intraocular metastasis occurs as part of distant metastasis.
- Long-term course after breast cancer treatment: Ocular metastasis may appear several to more than ten years after treatment.
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”Key Points for Diagnosis
Section titled “Key Points for Diagnosis”A history of malignancy and treatment is key to diagnosis. The combination of characteristic fundus findings (yellow-white flat lesions with marked serous retinal detachment) and a history of malignancy makes the diagnosis of metastatic choroidal tumor almost certain.
In lung cancer, ocular metastases may be discovered before the primary tumor. Some patients first visit an ophthalmologist due to vision loss, and subsequent workup reveals a systemic malignancy.
Required Examinations
Section titled “Required Examinations”Fundus examination: Confirmation of yellow-white flat to plaque-like lesions and marked serous retinal detachment. Slit-lamp microscopy is also performed.
Ultrasonography (B-mode): Confirms plate-like thickening of the ocular wall and serous retinal detachment. Tumor height is generally low, with a flat morphology compared to malignant melanoma.
Fluorescein angiography (FA): A pattern of granular hyperfluorescence progressing to diffuse hyperfluorescence, with a hypofluorescent rim around the tumor, supports the diagnosis.
OCT/SS-OCTA: Useful for evaluating tumor internal structure and retinal detachment. Swept-source OCT angiography (SS-OCTA) has been reported to visualize abnormal hairpin loop vessels within the tumor, improving diagnostic imaging 1).
Systemic workup when primary tumor is unknown:
- FDG-PET: Comprehensive search for systemic malignancies.
- Serum tumor markers (CEA, organ-specific markers): Performed as screening.
- Imaging studies (chest CT, abdominal ultrasound, etc.): Search for major primary tumors.
Differential Diagnosis
Section titled “Differential Diagnosis”| Disease | Key Points for Differentiation |
|---|---|
| Choroidal malignant melanoma | Black to brown, elevated. Serous retinal detachment is moderate |
| Choroidal hemangioma | Orange-red, spindle-shaped. No growth to slow growth |
| Choroidal osteoma | Bone-like hyperechogenicity. Acoustic shadow on ultrasound |
In lung cancer, metastatic lesions in the fundus may be discovered before the primary tumor. There are cases where a patient visits an ophthalmologist with a chief complaint of decreased vision, and metastatic lesions are found in the fundus, leading to the discovery of lung cancer through systemic examination. It is important to consider metastatic choroidal tumors as a cause of decreased vision and visual field abnormalities.
5. Standard Treatment
Section titled “5. Standard Treatment”Determination of Treatment Strategy
Section titled “Determination of Treatment Strategy”When uveal metastasis is identified, the prognosis is often poor. Not all cases are eligible for treatment; evaluation of the general condition and life prognosis is the first step. The treatment strategy is determined in collaboration with the department managing the primary tumor.
Systemic Treatment
Section titled “Systemic Treatment”If treatment for the primary tumor (chemotherapy, molecular targeted therapy, immunotherapy) is expected to be effective, systemic treatment is prioritized. Systemic treatment may also lead to regression of intraocular metastases. In recent years, with the introduction of molecular targeted drugs and immune checkpoint inhibitors, long-term survival cases have been observed.
Local Ocular Radiotherapy
Section titled “Local Ocular Radiotherapy”Local radiotherapy to the eye can be expected to have a certain effect regardless of the radiosensitivity of the primary tumor. The standard radiation dose is 40-50 Gy to the eye. Radiotherapy often leads to resolution of serous retinal detachment and regression of metastases, and improvement in visual acuity can be expected.
If life expectancy allows, radiotherapy is the basic approach; if systemic drug therapy can be initiated promptly, it may be given first.
Anti-VEGF therapy
Section titled “Anti-VEGF therapy”There are case reports of tumor control with anti-VEGF drugs (e.g., intravitreal aflibercept). In a 38-year-old woman with optic nerve metastasis from breast cancer, intravitreal aflibercept achieved tumor control and visual acuity improved from 20/50 to 20/251). However, systematic evidence for anti-VEGF therapy in ocular metastases is currently limited, and case-by-case consideration is necessary.
Radiotherapy (40–50 Gy to the eye) often leads to resolution of serous retinal detachment and shrinkage of the metastatic lesion, with expected visual improvement. Systemic chemotherapy or molecular targeted therapy has also been reported to reduce ocular metastases. However, treatment effects vary individually and depend on the systemic condition and disease progression.
6. Pathophysiology and detailed pathogenesis
Section titled “6. Pathophysiology and detailed pathogenesis”Hematogenous metastasis and choroidal entrapment
Section titled “Hematogenous metastasis and choroidal entrapment”Tumor cells from the primary lesion disseminate hematogenously throughout the body. Within the eye, the choroid is the most vascularized tissue, and the structure of the choriocapillaris creates an environment that facilitates entrapment of tumor cells.
The capillaries of the choriocapillaris have large diameters, making it easy for tumor cells to be trapped. After entrapment, tumor cells proliferate laterally along the vessels, resulting in a plaque-like morphology. This is a characteristic morphological feature of metastatic choroidal tumors.
RPE damage and exudative retinal detachment
Section titled “RPE damage and exudative retinal detachment”As tumor cells proliferate, the overlying retinal pigment epithelium (RPE) cells are damaged. The RPE is adjacent to the choriocapillaris across Bruch’s membrane, and mechanical compression or metabolic disturbance by the tumor impairs RPE function.
Impaired RPE function leads to leakage of fluid from the choroid into the subretinal space, forming exudative (serous) retinal detachment. This retinal detachment is the main cause of visual field defects, decreased visual acuity, and metamorphopsia. Metastatic choroidal tumors are characterized by prominent serous retinal detachment, which helps differentiate them from other choroidal tumors.
Distribution of metastatic sites
Section titled “Distribution of metastatic sites”Among intraocular metastases, choroidal metastasis is the most common and frequently occurs in the posterior pole. Metastases to the iris and ciliary body are rare. Metastatic lesions may be solitary or multiple within the same eye. Bilateral metastasis occurs in about one-quarter of cases.
7. Latest Research and Future Perspectives (Investigational Reports)
Section titled “7. Latest Research and Future Perspectives (Investigational Reports)”Advances in Imaging Diagnosis with SS-OCTA
Section titled “Advances in Imaging Diagnosis with SS-OCTA”Swept-source OCT angiography (SS-OCTA) provides new insights in the diagnostic imaging evaluation of metastatic choroidal tumors. It has been reported to visualize abnormal hairpin loop-like vascular structures within the tumor, and is useful for noninvasive assessment of tumor vasculature 1). This technique may complement conventional fluorescein angiography and contribute to detailed understanding of intratumoral vessels.
Effects of Molecular Targeted Therapy and Immunotherapy on Ocular Metastases
Section titled “Effects of Molecular Targeted Therapy and Immunotherapy on Ocular Metastases”With the widespread use of EGFR inhibitors, ALK inhibitors, and PD-1/PD-L1 inhibitors for lung cancer, control of ocular metastases accompanying effective systemic treatment has been reported. In breast cancer, the development of anti-HER2 therapy may contribute to increased long-term survival cases.
Local anti-VEGF therapy (e.g., aflibercept) for ocular metastases has been reported at the case report level for metastatic choroidal tumors 1), but evidence from systematic randomized controlled trials is currently lacking. Indication decisions must consider the systemic condition and tumor characteristics of each individual case.
Personalized Imaging Diagnosis and Treatment Monitoring
Section titled “Personalized Imaging Diagnosis and Treatment Monitoring”Advances in OCT and ultrasound have refined treatment monitoring. By quantitatively tracking the resolution of serous retinal detachment and tumor flattening, the effects of radiotherapy and systemic therapy can be evaluated more precisely.
8. References
Section titled “8. References”- Zhou N, Liang L, Wei W. Swept-Source OCT Angiography of Presumed Optic Nerve Metastasis from Breast Carcinoma. Ophthalmology. 2025;132(4):e74. doi:10.1016/j.ophtha.2024.06.025. PMID:39269385.
- Cennamo G, Montorio D, Carosielli M, Romano MR, Cennamo G. Multimodal Imaging in Choroidal Metastasis. Ophthalmic Res. 2021;64(3):411-416. PMID: 33142285.
- Singh A, Malik D, Singh S, Vyas VJ. Choroidal metastasis in pancreatic adenocarcinoma. J Cancer Res Ther. 2022;18(1):263-265. PMID: 35381796.