
Circumscribed Choroidal Hemangioma
1. What is circumscribed choroidal hemangioma?
Section titled “1. What is circumscribed choroidal hemangioma?”Circumscribed choroidal hemangioma (solitary choroidal hemangioma) is a sporadic benign vascular tumor of the choroid. It occurs as a well-defined, solitary lesion and is clearly distinguished from diffuse hemangioma associated with Sturge-Weber syndrome. It may be completely asymptomatic or cause vision loss and visual field defects.
A rare benign tumor that commonly occurs in middle-aged and older adults. The tumor often develops in the posterior pole (central part of the back of the eye), especially near the macula. It is not hereditary and appears sporadically. In contrast to choroidal hemangiomas associated with Sturge-Weber syndrome, which are diffuse and poorly defined, circumscribed (solitary) choroidal hemangioma is characterized as a well-defined single lesion.
Differential diagnosis from the three major choroidal tumors
Section titled “Differential diagnosis from the three major choroidal tumors”The following three diseases are important to differentiate from tumors arising in the choroid.
| Disease | Color | Shape/Height | Characteristics |
|---|---|---|---|
| Circumscribed choroidal hemangioma | Orange-red | Roundish, relatively flat | Benign, may be associated with serous retinal detachment |
| Choroidal malignant melanoma | Black to brown | Dome-shaped to mushroom-shaped, tall | Malignant, hematogenous metastasis possible |
| Metastatic choroidal tumor | Yellow-white | Flat, plate-like | Prominent retinal detachment, history of systemic malignancy |
| Choroidal nevus | Gray-black to brown | Small, flat | No growth, usually asymptomatic |
It is a benign vascular tumor and does not metastasize. However, tumor growth or serous retinal detachment on or around the tumor can cause decreased vision and visual field defects, so treatment is necessary when visual function declines. During follow-up, if changes in vision, metamorphopsia, or visual field abnormalities occur, prompt ophthalmologic consultation is recommended.
2. Main symptoms and clinical findings
Section titled “2. Main symptoms and clinical findings”Subjective symptoms
Section titled “Subjective symptoms”Circumscribed choroidal hemangioma often occurs in the posterior pole of the fundus. When serous retinal detachment occurs on or around the tumor, it can cause visual field defects, and if the detachment extends to the macula, it leads to decreased vision. Additionally, if the tumor occurs in the macula, tumor growth may cause hyperopia due to shortening of the axial length. The main subjective symptoms are as follows:
- Decreased vision: Occurs when serous retinal detachment extends to the macula or when the tumor directly infiltrates the macula
- Visual field defect: Appears as retinal detachment on or around the tumor expands
- Metamorphopsia (distorted vision): Due to retinal detachment or edema in the macular area
- Hyperopic shift: When the tumor causes shortening of the axial length, the usual prescription may no longer be adequate
- Asymptomatic: Small lesions located at the posterior pole periphery or mid-periphery may cause no symptoms at all
Fundus Findings
Section titled “Fundus Findings”On fundus examination, it appears as a localized, slightly elevated lesion with an orange-red color due to abnormal proliferation of blood vessels within the choroid. Typical fundus findings are shown below.
- Color: Well-defined orange-red to red lesion (color and appearance vary depending on the degree of retinal pigment epithelium atrophy)
- Shape: Roundish elevated lesion
- Ultrasonography (B-mode): The cross-section is fusiform, and the height is often less than one-third of the maximum diameter
- Serous retinal detachment: Frequently observed on or around the tumor
- Retinal pigment epithelium changes: Chronic lesions may be accompanied by RPE atrophy and pigmentation
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”Circumscribed choroidal hemangioma is thought to be formed by ectopic proliferation of neural crest cells during the embryonic period. Abnormal proliferation of blood vessels occurs within the choroid, forming a benign tumor. Exudate from the tumor accumulates in the subretinal space, leading to serous retinal detachment.
No clear risk factors have been established, and it is not hereditary. The pathogenesis differs from diffuse hemangioma associated with Sturge-Weber syndrome, and there is no association with systemic diseases. No links to ultraviolet light, lifestyle, diet, etc., have been shown.
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”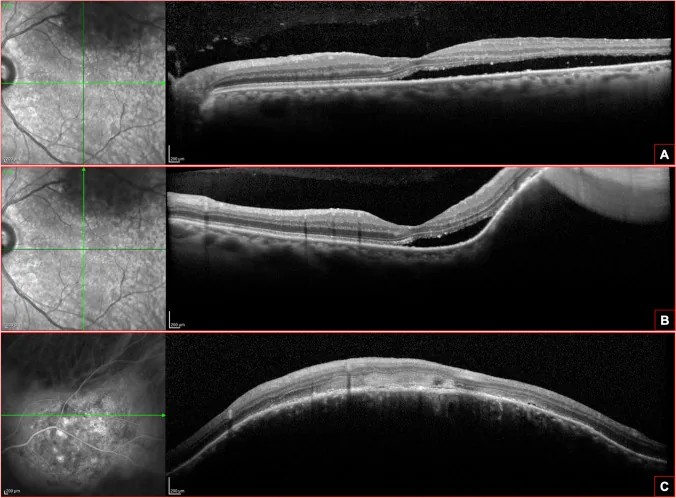
Circumscribed choroidal hemangioma can often be diagnosed by ophthalmoscopic findings (fundus examination). However, the color and appearance of the tumor vary depending on the degree of retinal pigment epithelium atrophy, and it is important to combine multiple tests for differential diagnosis.
Main Examinations
Section titled “Main Examinations”- Fundus examination: Confirms a well-defined, round or oval elevated lesion with an orange-red color. Commonly located in the posterior pole.
- Fluorescein angiography (FA) / Indocyanine green angiography (ICGA): In the early phase (arterial phase), a reticular hyperfluorescence corresponding to the tumor is observed. This is a key diagnostic finding.
- Ultrasonography (B-mode): The cross-section is fusiform, with height less than one-third of the maximum diameter. It shows high internal reflectivity.
- Optical coherence tomography (OCT): Used to quantify tumor height and extent, and to evaluate subretinal fluid. Also useful for monitoring treatment response.
- CT / MRI: Not necessarily required for diagnosis, but contrast-enhanced imaging shows diffuse, homogeneous enhancement. Also helpful for excluding extraocular lesions.
Differential Diagnosis
Section titled “Differential Diagnosis”| Disease | FA/ICGA Findings | Ultrasound Findings | Other Features |
|---|---|---|---|
| Circumscribed choroidal hemangioma | Reticular hyperfluorescence in arterial phase | Fusiform, height ≤ 1/3 of diameter | Orange-red, well-defined borders |
| Choroidal malignant melanoma | Double circulation pattern | Dome-shaped to mushroom-shaped, large height | Black to brown, acoustic hollow zone |
| Metastatic choroidal tumor | Hyperfluorescence corresponding to tumor | Flat, low height | Yellow-white, marked retinal detachment, history of systemic malignancy |
| Choroidal nevus | Hypofluorescence (blocking) | Flat, thin | Gray-black, small, no growth |
The diagnosis is confirmed by fundus examination showing an orange-red, well-defined elevated lesion, and by fluorescein angiography (FA/ICGA) revealing a reticular hyperfluorescence in the arterial phase. Ultrasound shows a spindle-shaped cross-section with a height less than one-third of the maximum diameter. OCT is used to evaluate tumor height and subretinal fluid, and is also used to monitor treatment effects.
5. Standard Treatment
Section titled “5. Standard Treatment”The treatment strategy for circumscribed choroidal hemangioma depends on the presence of symptoms and the degree of visual impairment.
Asymptomatic cases: Observation
Section titled “Asymptomatic cases: Observation”If there is no serous retinal detachment and no symptoms, no specific treatment is required. Regular follow-up with fundus examination and OCT is continued. If the tumor enlarges and serous retinal detachment appears, the need for treatment is reassessed.
Cases with serous retinal detachment or visual impairment: Active treatment
Section titled “Cases with serous retinal detachment or visual impairment: Active treatment”When visual impairment due to serous retinal detachment is present, the following treatments are indicated.
Photodynamic therapy (PDT): Currently the most widely used treatment. Verteporfin (6 mg/m²) is administered intravenously, and a laser with a wavelength of 690 nm is applied to the tumor. Although any treatment may cause strong scarring after irradiation, PDT minimizes damage to adjacent retinal tissue and is therefore often used as first-line therapy. Not covered by insurance.
Transpupillary thermotherapy (TTT): Thermotherapy using an 810 nm infrared laser. It is performed to coagulate and shrink the tumor. Like PDT, strong scarring may occur after irradiation.
Photocoagulation: A long-wavelength laser (e.g., 590 nm) absorbed by hemoglobin is used. The output is set to produce coagulation spots on the tumor surface, and coagulation is performed in several sessions. Due to scar formation after irradiation, PDT is often preferred nowadays.
Beta-blockers (oral propranolol): Reported to potentially shrink the tumor, but not covered by insurance, and evidence is limited to case reports.
If there are no symptoms and no serous retinal detachment, observation is sufficient. When visual function (visual acuity, visual field) declines due to serous retinal detachment, PDT or laser treatment is indicated. Response to laser treatment is often good, and tumor scarring and absorption of subretinal fluid can be expected. However, in treatment-resistant cases or cases with macular damage, visual function decline may persist.
6. Pathophysiology and Detailed Mechanisms
Section titled “6. Pathophysiology and Detailed Mechanisms”Tumor Formation
Section titled “Tumor Formation”Circumscribed choroidal hemangioma is formed by ectopic proliferation of neural crest cells during the embryonic period. Abnormal proliferation of blood vessels within the choroid forms a benign tumor, appearing as an orange-red elevated lesion on the fundus. The mechanism differs from diffuse hemangioma associated with Sturge-Weber syndrome, and there is no association with systemic neurocutaneous syndromes.
Mechanism of Serous Retinal Detachment
Section titled “Mechanism of Serous Retinal Detachment”Serous retinal detachment occurs when exudate from the tumor accumulates in the subretinal space. The mechanism of exudate production is thought to involve increased permeability of the tumor vessel walls. When retinal detachment extends to the macula, visual acuity decreases, and if chronic, photoreceptor cell degeneration can lead to irreversible visual function impairment.
Tumor Course
Section titled “Tumor Course”Rapid enlargement of the tumor itself is rare, and it often follows a slow course. As the tumor enlarges, the ocular axis shortens, leading to hyperopia. Chronic damage to the retinal pigment epithelium may result in incomplete recovery of visual function even after the serous retinal detachment resolves.
Mechanism of Action of Treatment
Section titled “Mechanism of Action of Treatment”PDT: The photosensitizer (verteporfin) selectively accumulates in tumor vessels, and laser irradiation produces reactive oxygen species within the tumor vessels, leading to vascular occlusion and tumor regression. An advantage is that damage to surrounding normal retina can be minimized.
TTT/Photocoagulation: Laser thermal energy directly coagulates and scars the tumor tissue. Because scarring is strong, attention must be paid to effects on surrounding normal tissue.
7. Latest Research and Future Prospects (Investigational Reports)
Section titled “7. Latest Research and Future Prospects (Investigational Reports)”Long-term Outcomes of PDT
Section titled “Long-term Outcomes of PDT”PDT is currently positioned as the main treatment for circumscribed choroidal hemangioma with serous retinal detachment. Tumor regression and absorption of subretinal fluid after treatment are reported to be good in many cases, but recurrence and cases requiring retreatment have also been reported. Standardization of optimal irradiation conditions (light dose, spot size, irradiation time) continues to be investigated.
Intravitreal Anti-VEGF Injection
Section titled “Intravitreal Anti-VEGF Injection”Based on the possibility that vascular endothelial growth factor (VEGF) is involved in the production of exudate from the tumor, there are case reports that intravitreal injection of anti-VEGF drugs is effective in controlling serous retinal detachment. However, the evidence for anti-VEGF therapy for circumscribed choroidal hemangioma remains at the case report level and is not covered by insurance.
Oral Propranolol
Section titled “Oral Propranolol”It has been reported that the beta-blocker propranolol may contribute to the shrinkage of tumor blood vessels. This treatment was inspired by the effectiveness of propranolol for infantile hemangiomas (superficial hemangiomas) in pediatric ophthalmology, and case reports of tumor shrinkage effects in choroidal hemangioma are accumulating. Further research is needed regarding specific dosage, treatment duration, and long-term efficacy.
8. References
Section titled “8. References”- Madreperla SA, Hungerford JL, Plowman PN, Laganowski HC, Gregory PT.. Choroidal hemangiomas: visual and anatomic results of treatment by photocoagulation or radiation therapy. Ophthalmology. 1997;104(11):1773-8; discussion 1779. doi:10.1016/s0161-6420(97)30027-x. PMID:9373106.
- Blasi MA, Tiberti AC, Valente P, et al. Intralesional bevacizumab for choroidal hemangioma with exudative retinal detachment: an optical coherence tomography evaluation. Ophthalmology. 2010;117(8):1606-1611.
- Boixadera A, García-Arumí J, Martínez-Castillo V, Encinas JL, Elizalde J, Blanco-Mateos G, Caminal J, Capeans C, Armada F, Navea A, Olea JL.. Prospective clinical trial evaluating the efficacy of photodynamic therapy for symptomatic circumscribed choroidal hemangioma. Ophthalmology. 2009;116(1):100-105.e1. doi:10.1016/j.ophtha.2008.08.029. PMID:18973950.
- Anand R. Transpupillary thermotherapy for circumscribed choroidal hemangioma. J Pediatr Ophthalmol Strabismus. 2003;40(1):43-44.