Optical coherence tomography angiography (OCTA) is a non-invasive fundus angiography technique that adds a blood flow detection function to an OCT device using near-infrared light. First clinically applied in 2014, it has rapidly spread as a contrast-free vascular visualization technology.
OCTA non-invasively visualizes vascular structures from retinal and choroidal blood flow, contributing to the diagnosis and treatment decisions for age-related macular degeneration, diabetic retinopathy, and other conditions.
The basic principle of OCTA is motion contrast (split-flow: OCTA signal). The same site is repeatedly scanned, and blood flow information is extracted by separating temporally varying signal components (i.e., movement of blood cells) from stationary tissue signals. Specifically, the same site is repeatedly OCT-scanned in a short time, and the amplitude and phase changes (decorrelation) between A-scans are calculated. Stationary tissue shows no change, while areas with blood flow show change. From this difference, vascular structures are visualized.
There are two types depending on the light source used: SD-OCT (Spectral Domain) and SS-OCT (Swept Source). SS-OCT has a longer wavelength, so it is superior for imaging deep choroidal structures.
QHow is OCTA different from fluorescein angiography (FA)?
A
FA involves intravenous injection of a contrast agent and records two-dimensional fluorescence patterns including leakage. OCTA does not require a contrast agent and three-dimensionally visualizes only blood flow, enabling layer-specific analysis and quantification. However, it cannot evaluate leakage, staining, or pooling, so it is used complementarily with FA. It is particularly useful for patients with contrast agent allergies or renal impairment. For details, see the section “Main Features and Comparison with FA”.
Dilation: Imaging under mydriasis is recommended. Small pupils (less than 4 mm) significantly reduce image quality.
Fixation check: Poor fixation is a major cause of eye movement artifacts. Have the patient fixate on the fixation light and confirm stable fixation before imaging.
Assessment of cataract and vitreous opacity: Media opacity reduces signal strength and impairs vessel visualization.
In OCTA, the boundaries (segmentation) of each layer are automatically set based on OCT B-scans, but in diseased eyes, automatic segmentation often fails. After imaging, always check the segmentation lines and manually correct any misalignment.
4. Normal Findings and Vascular Plexuses of Each Layer
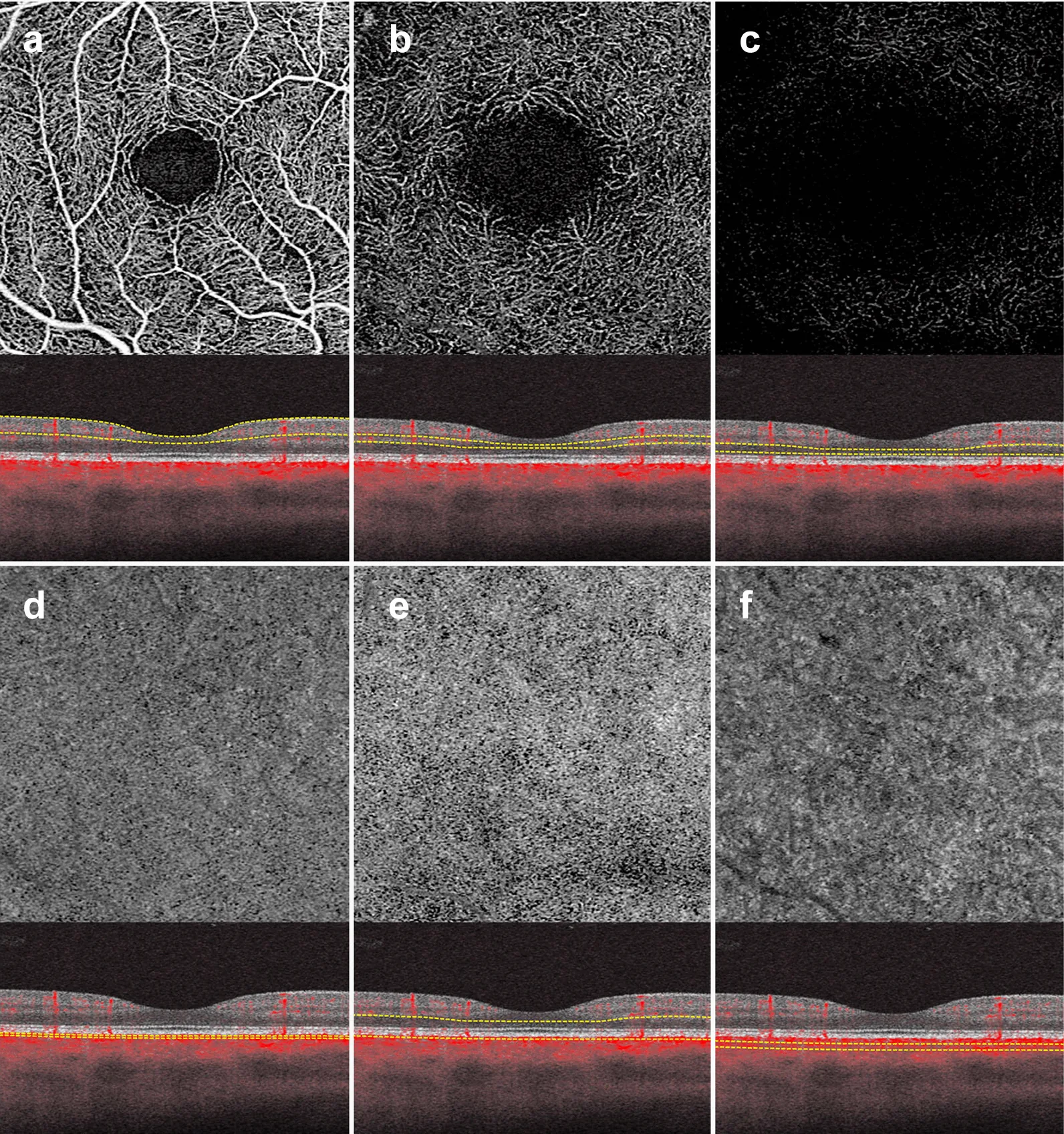
Greig EC, Duker JS, Waheed NK. A practical guide to optical coherence tomography angiography interpretation. Int J Retina Vitreous. 2020;6:55. Figure 3. PMCID: PMC7666474. License: CC BY 4.0.
Six retinal slabs on OCTA. (a) Superficial capillary plexus (SCP), (b) deep capillary plexus (DCP), (c) avascular layer, (d) choriocapillaris (CC), (e) outer retina-choriocapillaris (ORCC), (f) choroid, with en face images and segmentation lines. Corresponds to the layered structure of retinal vascular plexuses discussed in section “4. Normal Findings and Vascular Plexuses of Each Layer”.
SCP (superficial capillary plexus): Large arterioles, venules, and a dense capillary network are distributed. The foveal avascular zone (FAZ) around the fovea is clearly delineated.
DCP (deep capillary plexus): A denser honeycomb-like capillary network. The FAZ often appears smaller than in the SCP.
Outer retina: No blood flow signal is normally present. If a blood flow signal is detected here, suspect type 1, 2, or 3 macular neovascularization (MNV).
CC (choriocapillaris): Granular blood flow pattern. It is visualized as flow spots.
OCTA has specific artifacts that can affect clinical judgment, so understanding them is essential. Some artifacts allow evaluation comparable to angiography, while others make assessment difficult, requiring careful interpretation.
Artifact
Cause
Effect
Signal loss
Media opacity / pigmentation
False flow void
Projection
Shadow of superficial vessels
False flow in deep layers
Segmentation error
Pathological morphological changes
Interlayer signal mixing
Eye movement
Poor fixation
Linear white bands/duplication
Signal attenuation artifact: Cataract, vitreous hemorrhage, or pigmentation reduces deep signal, causing perfused vessels to be misidentified as flow voids.
Projection artifact: Signals from superficial vessels are projected onto deeper slabs, appearing as false flow. Projection removal (PR) algorithms reduce but do not completely eliminate this artifact.
Segmentation error: Retinal edema, atrophy, or epiretinal membrane can cause automatic segmentation failure, mixing vessel information from unintended layers. Manual correction is required.
Eye movement artifact: White linear or zipper-like noise due to poor fixation. Re-scanning is standard, but some devices offer eye-tracker correction.
QHow can artifacts be minimized?
A
Perform pupillary dilation, check fixation, and assess media clarity before imaging; confirm image quality scores. Always visually verify segmentation after acquisition. Enable projection removal if available. Exclude images with motion artifacts, vessel segmentation errors, or media opacities.
OCTA can finely depict capillary abnormalities in DR. It enables detection of FAZ enlargement/irregularity, capillary dropout (flow voids), and neovascularization. Non-perfusion areas (NPA) are delineated more clearly than with FA. Since NV and IRMA shapes can be confusing on en face images, OCT B-scans should be used to confirm flow signals. The AAO Diabetic Retinopathy Preferred Practice Pattern (2024) states that OCTA is a complementary test to FA, particularly useful for evaluating the macular capillary network4).
Vessel density (VD) correlates with the stage of DR and is being studied as an objective indicator of retinal ischemia. Srinivasan et al. (2023) reported in a longitudinal study of DR patients that lower baseline SCP-VD was associated with a higher risk of DR severity progression over one year 2). The median SCP-VD in the progression group was 12.90%, compared to 14.90% in the non-progression group, with a significant difference (p=0.032), and a hazard ratio of 0.825 (AUC=0.643).
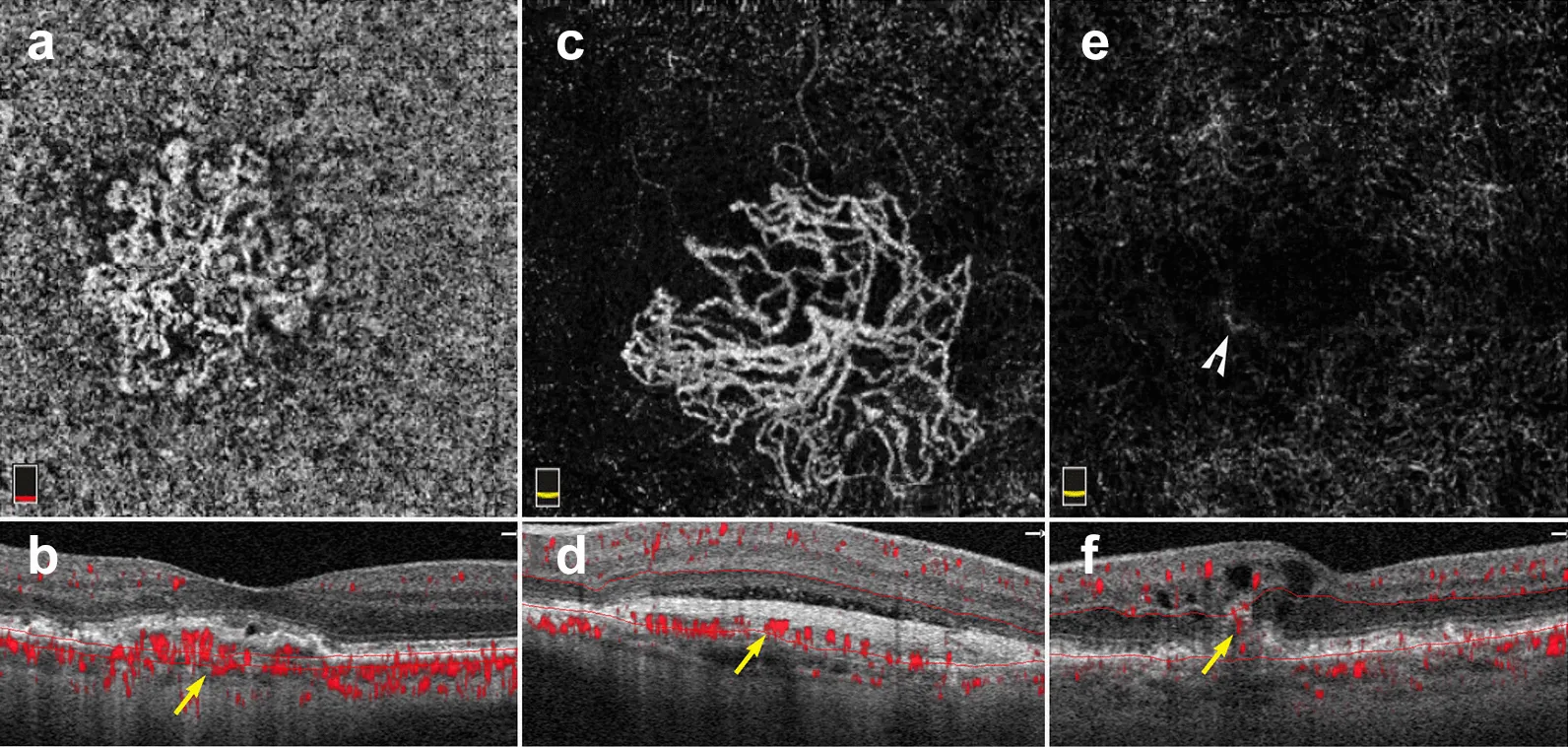
Greig EC, Duker JS, Waheed NK. A practical guide to optical coherence tomography angiography interpretation. Int J Retina Vitreous. 2020;6:55. Figure 9. PMCID: PMC7666474. License: CC BY 4.0.
Three types of macular neovascularization in exudative AMD shown on 3×3 mm en face images and B-scans. (a-b) Type 1 MNV (sub-RPE blood flow), (c-d) Type 2 MNV (vessels between RPE and retina), (e-f) Type 3 MNV (intraretinal bright spots). Corresponds to the detection of choroidal neovascularization (MNV) discussed in section “6. Clinical Applications (Retinal Diseases)”.
Detection of choroidal neovascularization (MNV) is one of the main indications for OCTA. For macular OCTA evaluation, a fine scan angle of 3×3 mm or 6×6 mm is desirable. The AAO AMD Preferred Practice Pattern (2024) reports that OCTA has a sensitivity of 0.87 and specificity of 0.97 for detecting macular neovascularization, with diagnostic accuracy comparable to FA5).
Additionally, OCTA may detect asymptomatic subclinical macular neovascularization (type 1 MNV, drusen-associated MNV) that is not detectable by FA, which is of interest from the perspective of early intervention 5).
In RVO, capillary dropout and flow voids at the occlusion site are clearly visualized on OCTA. It is possible to evaluate vascular structures by retinal layer, and microaneurysms (MA) occurring in the superficial or deep capillary layers can also be identified. The AAO RVO Preferred Practice Pattern (2024) states that OCTA is useful for assessing the extent of ischemia in the macular capillary network 6).
In RAO, flow voids in the superficial capillaries corresponding to the area supplied by the occluded vessel are observed from the acute phase. The AAO RAO Preferred Practice Pattern (2024) states that early blood flow assessment by OCTA is useful for management 7).
Torpedo maculopathy: OCTA reveals avascular areas in the outer retina and choriocapillaris. Knani et al. (2023) performed OCTA on type 1 and type 2 torpedo maculopathy and reported signal defects in the choriocapillaris corresponding to the lesion 1).
Sickle cell disease (SCD): In SCD, it is meaningful to evaluate vascular damage in the conjunctiva and retina at multiple sites. Mgboji et al. (2022) used conjunctival OCTA to record the characteristics of conjunctival microvascular morphology in SCD patients and showed that this method can be applied to monitor vascular complications in SCD 3).
Glaucoma is a leading cause of irreversible blindness. OCTA can detect decreased vascular density in glaucomatous eyes and is expected to be applied for diagnosis and progression assessment. The Glaucoma Practice Guidelines (5th edition) state that OCTA can evaluate superficial and deep retinal blood flow, and it is known that superficial retinal blood flow decreases as glaucoma progresses 8).
In glaucomatous eyes, vascular density (VD) in the peripapillary and macular areas decreases and correlates with disease severity. The decrease in VD is more pronounced in the superficial layer. It is less affected by the floor effect of structural OCT and may be advantageous for assessing progression in advanced glaucoma8). As cupping progresses, capillaries within the optic disc disappear, and radial peripapillary capillaries are lost in correspondence with retinal nerve fiber layer defects.
Microvascular dropout (MvD) refers to the loss of choriocapillaris in the peripapillary atrophic area. It is often observed in the inferotemporal area within the β-zone. MvD is associated with RNFL thinning, lamina cribrosa defects, and visual field defects, and is an indicator predicting faster progression of RNFL thinning and visual field loss.
Longitudinal Progression Assessment and Postoperative Evaluation
Lower baseline peripapillary and macular VD is associated with faster RNFL progression in early to moderate glaucoma. This association is independent of baseline RNFL thickness, suggesting that OCTA may provide additional contribution to risk assessment of progression.
Multiple studies have reported a significant increase in microvascular VD after glaucoma surgery, likely due to increased ocular blood flow resulting from intraocular pressure reduction.
Pathophysiology of Glaucoma and Significance of OCTA
Elevated intraocular pressure and lamina cribrosa deformation: Relative elevation of intraocular pressure causes deformation and thinning of the lamina cribrosa, disrupting axonal transport of retinal ganglion cells (RGCs) and leading to apoptosis.
Rationale for intraocular pressure-lowering treatment: Many large-scale studies identify intraocular pressure as the greatest risk factor for the onset and progression of glaucoma.
Limitations: It cannot fully explain normal-tension glaucoma or cases that progress despite intraocular pressure reduction.
Vascular Theory
Decreased ocular blood flow and ischemia: Reduced ocular perfusion pressure and loss of vascular autoregulation expose the optic nerve to ischemia and oxidative stress.
Role of arteriosclerosis: Arteriosclerosis may create high pulsatility, potentially damaging ocular microvessels9).
Significance of OCTA: OCTA, which can quantitatively assess vessel density, is a powerful tool for investigating the vascular theory.
In recent years, the “mechanical theory” and “vascular theory” are not considered independent; rather, an integrated view as a biomechanical theory of the optic nerve head has become mainstream. Glaucomatous optic neuropathy is thought to result from complex interactions between intraocular pressure-dependent factors and non-intraocular pressure-dependent factors (circulatory disorders, autoimmunity, oxidative stress, etc.)10).
QIs OCTA useful for early detection of glaucoma?
A
In glaucomatous eyes, thinning of the nerve fiber layer and reduction in peripapillary vessel density may precede visual field abnormalities, and research on early detection using OCTA is ongoing. The diagnostic ability of OCTA is generally considered comparable to OCT (RNFL thickness, GCC thickness), but some reports indicate that OCT-measured RNFL thickness has better sensitivity in early glaucoma. In advanced glaucoma, OCTA may be advantageous as it is less susceptible to floor effects8). Currently, OCT structural imaging and visual field testing remain the mainstays for diagnosis and management, with OCTA playing a complementary role.
OCTA is based on SD-OCT or SS-OCT. Repeated B-scans are acquired at the same retinal location, and decorrelation (signal change) between consecutive images is detected. Red blood cells flowing within vessels alter the reflected signal, while surrounding stationary tissue does not. This difference is visualized as a blood flow map.
Major Algorithms
SSADA: Split-spectrum amplitude-decorrelation angiography. Used in AngioVue® (Optovue®).
OMAG: OCT-based microangiography. Used in Angioplex® (Zeiss®).
OCTARA: OCTA ratio analysis. Mounted on the SS-OCTA of Triton® (TopCon®).
Others: Intensity and phase decorrelation combination method of AngioScan® (NIDEK®), etc.
Points to note when selecting a device
Inter-device incompatibility: Because algorithms and default slab depths differ, direct comparison between devices is not possible even for the same patient.
SS-OCTA: TopCon®, Canon®, and Zeiss® provide swept-source OCTA, which improves speed and resolution in evaluating the choroidal layer.
Image quality criteria: Exclude low-quality images with a signal strength index (SSI) less than 40 (less than 6 for Zeiss).
Research is advancing on using OCTA quantitative indicators as biomarkers for predicting DR progression. Srinivasan et al. (2023) longitudinally showed that baseline SCP-VD (vessel density) was significantly associated with the risk of DR progression 2). VD was 12.90% (progression group) vs. 14.90% (non-progression group), p=0.032, hazard ratio 0.825, AUC=0.643.
The development and widespread use of ultra-widefield OCTA exceeding 12×12 mm is expected to improve detection sensitivity for peripheral retinal vascular lesions and neovascularization in preproliferative retinopathy 3).
Early Intervention for Subclinical Macular Neovascularization
Clinical studies are underway to investigate whether anti-VEGF treatment for subclinical macular neovascularization detected by OCTA can suppress progression to exudative AMD5).
Beros et al. (2024) showed in a large cohort that arterial pulse wave velocity (aPWV) is associated with an increased risk of primary open-angle glaucoma9). High arterial stiffness may contribute to glaucoma onset through ocular microvascular damage, suggesting that OCTA vessel density assessment could serve as a biomarker in the future 10).
The main research topics are automated analysis of OCTA images using AI, standardization of quantitative values across devices, and development of progression prediction models. If standardization of quantitative values is achieved, longitudinal comparative studies across multiple institutions will become possible.
QIn what direction will OCTA evolve in the future?
A
The main directions are wider angle, higher speed, AI-based automated analysis, and standardization of quantitative biomarkers. Establishing standardization criteria to eliminate differences in quantitative values between devices is also an important research topic. Application to monitoring systemic diseases using conjunctival OCTA is also expected3).
Mgboji GE, Cain D, Scott AW. Conjunctival optical coherence tomography angiography imaging in sickle cell maculopathy. Am J Ophthalmol Case Rep. 2022;26:101428. doi:10.1016/j.ajoc.2022.101428. PMID:35243165; PMCID:PMC8861406.
Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025 Apr;132(4):P75-P162. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.
Vemulakonda GA, Bailey ST, Kim SJ, Kovach JL, Lim JI, Ying GS, et al. Age-Related Macular Degeneration Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P1-P74. doi:10.1016/j.ophtha.2024.12.018. PMID:39918524.
Kovach JL, Bailey ST, Kim SJ, Lim JI, Vemulakonda GA, Ying GS, et al. Retinal Vein Occlusions Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P303-P343. doi:10.1016/j.ophtha.2024.12.025. PMID:39918523.
American Academy of Ophthalmology. Retinal Artery Occlusions Preferred Practice Pattern. AAO; 2024.
Beros AL, Sluyter JD, Hughes AD, et al. Arterial Stiffness and Incident Glaucoma: A Large Population-Based Cohort Study. Am J Ophthalmol. 2024;266:68-76. doi:10.1016/j.ajo.2024.05.015. PMID:38754800.
Stangos A, et al. Ocular and Systemic Risk Factors and Biomarkers for Glaucoma: An Umbrella Review of Systematic Reviews and Meta-Analyses. Invest Ophthalmol Vis Sci. 2025;66(12):35.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.