Epiretinal membrane (ERM) is a fibrocellular proliferative tissue that forms on the internal limiting membrane (ILM) of the retina. It is also called macular pucker, cellophane maculopathy, premacular fibrosis, or vitreomacular interface syndrome 11). Epiretinal membrane can secondarily cause retinal folds, macular edema, and tractional retinal detachment.
Epiretinal membrane is classified into idiopathic and secondary types. Secondary ERM is also called macular pucker 11).
The prevalence varies depending on the examination method and target population, with a wide range of reports. The prevalence from each study is summarized below.
The prevalence of cellophane maculopathy (asymptomatic ERM) is reported to be 1.8–25.1%, and symptomatic ERM (preretinal macular fibrosis) 0.7–3.9%12). It is estimated that approximately 30 million people in the United States are affected12). Bilateral involvement is seen in 20–35%11). Ethnic differences have also been reported; in the MESA study, the prevalence was 39.0% in Chinese, 29.3% in Hispanic, 27.5% in White, and 26.2% in Black individuals16).
Over 5 years, 29% of ERM progress, 26% regress, and 39% remain stable (Blue Mountains Eye Study)14). Progression of cellophane maculopathy is only 20% over 5 years. Spontaneous separation of ERM with PVD occurs in 1.5% (16 of 1,091 eyes), and without PVD in 13.6% (21 of 157 eyes, mean follow-up 33 months)12). Delaying surgery until symptom onset does not worsen prognosis compared to immediate surgery12). In young patients without posterior vitreous detachment, spontaneous separation rarely occurs, so careful observation is warranted.
In neurofibromatosis type 2 (NF2), the prevalence of epiretinal membrane reaches 80% 9). The prevalence of vitreomacular traction (VMT) is 0.4–2.0% (age ≥63 years), and ERM and VMT often coexist 12).
QIs surgery always necessary for epiretinal membrane?
A
Not all epiretinal membranes require surgery. If there are no symptoms, symptoms are mild, or visual acuity is good, observation is chosen. It has been reported that over 5 years, 29% progress, 26% regress, and 39% remain stable 14), and delaying surgery until symptoms appear does not worsen prognosis 12). Surgery is usually considered when corrected visual acuity is 0.7 or worse and metamorphopsia is severe, or when vision loss is relatively acute and thought to be due to the epiretinal membrane. Ultimately, the decision is made based on the patient’s subjective symptoms.
Epiretinal membrane is often asymptomatic, and it is not uncommon for it to be discovered incidentally during health checkups or follow-up for other diseases. When symptomatic, it presents with the following symptoms.
Metamorphopsia (distortion): Straight lines appear distorted. This is the most characteristic symptom and one that patients easily report.
Decreased visual acuity: Occurs as the membrane contracts and thickens.
Micropsia: Objects appear smaller. Caused by macular distortion due to membrane traction.
Macropsia: Objects may appear larger than they actually are.
Slit-lamp microscopy reveals a glistening appearance on the macular surface, retinal folds, and vascular tortuosity. By widening the slit beam and observing the macula, the thickness and distribution of the membrane can be assessed in combination with OCT images. In the early stages, it is characterized by a shimmering reflection known as water silk reflex. As the disease progresses, macular edema and pseudomacular hole may occur.
Thick, white, opaque membranes are more likely to be symptomatic and cause macular ectopia 12). Loss of the normal foveal depression, cystoid macular changes, lamellar macular hole, and progression to full-thickness macular hole are also possible.
Vitreopapillary traction: Vitreous adhesions around the optic disc may accompany ERM. Caution is needed because it can be misdiagnosed as optic disc edema (congested optic disc)12).
Optical coherence tomography angiography (OCTA) reveals morphological changes in the foveal avascular zone (FAZ). The FAZ area in eyes with epiretinal membrane is 0.11 mm², which is significantly smaller than the 0.24 mm² in healthy eyes2).
The most important factor associated with epiretinal membrane is posterior vitreous detachment (PVD). According to the conventional hypothesis, residual cortical vitreous after PVD causes dehiscence of the ILM, and glial cells and RPE cells migrate into the vitreous cavity, differentiating and proliferating into fibroblast-like cells, leading to the formation of epiretinal membrane11).
A newer hypothesis gaining support suggests that ILM dehiscence is not essential. It proposes that cells in the vitreous cortex remaining on the ILM are activated into myofibroblasts, resulting in membrane formation and contraction12).
Pathophysiology Based on the Vitreous Pocket Theory
Even before posterior vitreous detachment occurs, liquefied spaces (precortical vitreous pockets) exist within the posterior vitreous gel. The posterior wall of the pocket is a thin, elastic vitreous cortex, and it is thought that modifications such as cell proliferation on this posterior vitreous cortex in front of the macula lead to the formation of epiretinal membrane.
There are cases where the posterior wall of the pocket adheres to the macula without PVD, causing traction on the retina, and cases where the posterior wall of the pocket remains on the retinal side after complete PVD, distorting the macula. Cell proliferation on the posterior wall of the vitreous pocket can form an epiretinal membrane, which is often seen in secondary cases or in young individuals. Spontaneous separation may occur when posterior vitreous detachment happens.
Note that in 20.1% of cases, the posterior vitreous was attached at the time of surgery, and the presence of a Weiss ring does not necessarily indicate complete separation of the posterior vitreous12).
In NF2-associated epiretinal membrane, immunohistochemistry shows weak positivity for GFAP and moderate positivity for nestin, suggesting that components derived from Müller cells are predominant9).
The main risk factors are listed below.
Aging: Increases sharply after age 50, with further increase in prevalence after age 75.
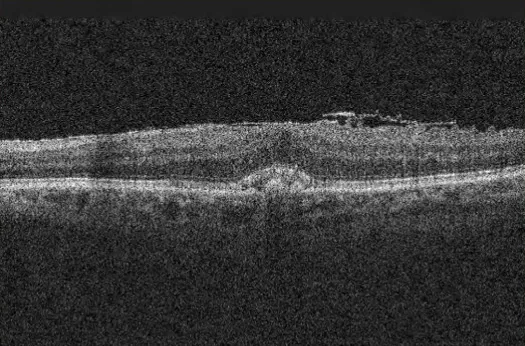
Wikimedia Commons. File:EpiretinalMembrane_OCT.png. License: CC BY-SA.
Optical coherence tomography (OCT) image of an epiretinal membrane in an 89-year-old male. Corresponds to the epiretinal membrane discussed in section “4. Diagnosis and examination methods”.
Optical coherence tomography (OCT) is central to diagnosis. ERM is visualized as a hyperreflective layer on the inner surface on OCT, often attached by pegs from the inner retinal surface, and shows a wavy cross-section. Findings include foveal depression loss, outer retinal elevation, and cystoid changes. OCT also allows assessment of vitreous or membrane traction on the retina, retinal swelling, cystoid changes, presence of retinal detachment, and the state of the ellipsoid zone (EZ). En face OCT is useful for preoperative prediction of ILM defects, and ILM defects are confirmed preoperatively in 22.7% of cases1).
ERM+VMT coexistence is found in 57% of ERM eyes, and ERM is reported to coexist in 65% of VMT eyes12).
OCTA (optical coherence tomography angiography) shows an increase in vascular area density (VAD) of the superficial capillary plexus (SCP)2). It is also useful for detecting epiretinal membrane-induced intraretinal neovascularization6).
Fluorescein angiography (FA): In early ERM, the image is relatively normal. As membrane contraction progresses, vascular tortuosity is observed near the center of traction, and straightening of vessels is seen in the periphery. Leakage patterns from capillaries under traction are also observed. When dye accumulates in cystoid spaces, differentiation from pseudophakic CME is necessary (CME shows a more petaloid pattern with optic disc hyperfluorescence) 12). FA/OCTA is also useful for detecting associated retinal vascular occlusion, diabetic retinopathy, macular telangiectasia, and choroidal neovascularization12).
When the ellipsoid zone (EZ) and interdigitation zone (IZ, cone outer segment tips line) are intact on preoperative OCT, postoperative visual acuity tends to be better 12). The outer retina, EZ, and photoreceptor outer segment length can improve and normalize after surgery (each parameter correlates with visual improvement). In a study of 101 eyes using time-domain OCT, photoreceptor layer damage was reported as a predictor of poor postoperative visual acuity12).
A special type of epiretinal membrane is macular pseudohole. Contraction of the epiretinal membrane causes the foveal depression to become cylindrical, presenting findings similar to a macular hole.
As a clinical differentiating point, visual acuity is often relatively well preserved in macular pseudohole. On slit-lamp examination, the Watzke-Allen sign is useful for differentiation: in macular hole, the patient perceives a break in the slit beam (positive), while in macular pseudohole, the slit beam is perceived as uniform in width (negative). OCT makes differentiation between the two easy.
Visual impairment and retinal thickening are prerequisites for surgical indication. Even if visual acuity is good, surgery is indicated if retinal thickening is marked with severe metamorphopsia, or if a full-thickness macular hole is present.
Relatively acute visual decline and visual impairment attributable to the epiretinal membrane compared to the degree of cataract are also indications for surgery. The rate of symptom progression and impact on the patient’s occupation and daily life (difficulty reading, driving) should be specifically assessed, and the final decision is made in consideration of the patient’s subjective symptoms. Surgery is elective and not urgent 12).
QWhat is the most important test for diagnosing epiretinal membrane?
A
OCT (optical coherence tomography) is the most important test. It can noninvasively visualize the hyperreflective membranous structure on the retinal surface and retinal thickening, and is used for diagnosis, surgical indication, and postoperative follow-up. It also allows evaluation of foveal depression loss, ellipsoid zone status, and intraretinal cystoid changes. Preoperative EZ/IZ integrity is also useful for predicting postoperative prognosis 12).
The standard surgical procedure for epiretinal membrane treatment is pars plana vitrectomy (PPV) + epiretinal membrane peeling + ILM peeling. 23G, 25G, and 27G microincision vitrectomy surgery (MIVS) is standard, enabling minimally invasive and early recovery.
Epiretinal Membrane Peeling
Purpose: To remove the proliferative membrane that is the source of traction and restore retinal morphology.
Technique: Grasp the edge of the membrane with vitreous forceps (microforceps) and gently peel it away from the fovea like peeling a membrane, avoiding creating a macular hole. In cases without posterior vitreous detachment, artificial PVD creation may simultaneously detach the membrane.
ILM Peeling
Purpose: To prevent recurrence of the epiretinal membrane and promote more complete retinal expansion.
ILM border management: Even when only the epiretinal membrane is intended to be removed, the ILM usually cracks. Additional peeling is performed so that the border between the peeled and unpeeled ILM does not cross the macula. Preoperative en face OCT reveals ILM defects in 22.7% of cases1), and the defect-edge technique is useful1).
Use of staining agents: Brilliant blue G (BBG, TISSUEBLUE®) is FDA-approved (2019) for ILM/ERM staining and is widely used. ICG, trypan blue, and triamcinolone are also used off-label. Low concentrations are considered safe, but minimizing light exposure time is important, and debate continues12). Shaving the peripheral vitreous (especially near the cannula) can reduce the risk of iatrogenic retinal tears.
Visual acuity improvement rate: Approximately 80% of cases achieve Snellen 2-line or more improvement in visual acuity12) (73% in previous reports11)). 10–20% have unchanged or worsened vision.
Degree of visual acuity improvement: logMAR improves from 0.4 to 0.1 (preoperative vs. postoperative comparison)2).
Improvement in metamorphopsia: 56% of patients had metamorphopsia preoperatively, which decreased to 13% postoperatively11).
VFQ-25 score: Significantly improves at 6 and 24 months postoperatively12).
Long-term outcomes (Elhusseiny 2020, 49 eyes, mean follow-up 111 months): BCVA improved from 0.56 (20/72) preoperatively to 0.33 (20/42) at 1 year, 0.25 (20/35) at 3 years, and 0.28 (20/38) at 10 years, with improvement continuing up to 3 years and stability maintained up to 10 years17).
Course of visual recovery: Vision gradually improves over 3–6 months postoperatively, and slow improvement may continue up to 12 months. Retinal thickening and associated visual dysfunction may still remain at 1 year postoperatively. Postoperative visual acuity correlates well with preoperative visual acuity, so it is important to perform surgery before significant vision loss occurs.
ILM peeling is effective in preventing ERM recurrence and is now incorporated into standard surgery12).
Recurrence prevention: Without ILM peeling, ERM recurrence rate is 8.6–21%; with ILM peeling, it is 0–2.6%12).
Ducloyer 2024 RCT (213 eyes): Compared spontaneous peeling (101 eyes), active ILM peeling (51 eyes), and no peeling (49 eyes). Recurrence rate was 0% with active peeling vs. 19.6% without, a significant difference. However, recovery of BCVA and microperimetry was slightly delayed in the active ILM peeling group18).
2017 meta-analysis: No clear difference in visual improvement, but ILM peeling was superior in suppressing ERM recurrence19).
Conclusion: ILM peeling is effective in preventing recurrence, but its superiority for visual acuity is not clear. Dissociated optic nerve fiber layer (DONFL) may occur, but its functional impact is unknown.
VMT (Vitreomacular Traction) is closely related to ERM and often coexists.
VMT ≤1500 μm: 23–47% resolve spontaneously within 1–2 years. Observation is an option if vision is stable12).
Extensive VMT (>1500 μm), cases with macular detachment, or poor vision: Spontaneous improvement is unlikely, and vitrectomy is indicated12).
Pneumatic vitreolysis (gas injection to release VMT): Intravitreal injection of 0.3 ml C3F8 showed an 85.7% VMT release rate in one study, but the DRCR Retina Network RCT reported higher-than-expected rates of retinal tear and retinal detachment, leading to early termination due to safety concerns12). Currently, clear evidence is lacking, and individual risk-benefit assessment is necessary.
Ocriplasmin: A recombinant protease. FDA-approved in 2012 for symptomatic VMA/VMT. Phase III trials showed VMA resolution in 27% vs. 10% with placebo (P<0.001)12). Efficacy is limited in ERM-associated VMT (VMA resolution 8.7% vs. 1.5% placebo) and ineffective for ERM alone12). Side effects include vitreous floaters, photopsia, eye pain, and blurred vision (about 10%, first week). Rare serious side effects include acute severe vision loss, ERG abnormalities, and color vision disturbances, but most are reversible12).
Standard treatment is surgery, but the following non-surgical spontaneous or induced detachment has been reported (all at case report level).
Dexamethasone intravitreal implant (DEX implant): Cases of spontaneous detachment of the epiretinal membrane after intravitreal administration have been reported7).
Spontaneous detachment after anti-VEGF + photodynamic therapy (PDT): Cases of spontaneous detachment of the epiretinal membrane after photodynamic therapy have been reported4).
These remain case reports and are not currently standard treatment.
QIs it always necessary to peel the ILM (internal limiting membrane)?
A
ILM peeling is effective for preventing recurrence of epiretinal membrane and is incorporated into current standard surgery. Recurrence rates are reported as 0–2.6% with ILM peeling and 8.6–21% without 12). If an ILM defect is confirmed on preoperative en face OCT (present in 22.7% of cases), peeling from the defect edge is required 1). However, the technical difficulty is high, and the decision should be made considering the balance with the risk of complications such as RPE atrophy. In the active ILM peeling group, visual recovery may be slightly delayed 18).
QWhen will vision recover after surgery?
A
Visual recovery progresses slowly over 3–6 months after surgery, and improvement may continue up to 12 months postoperatively. Even at one year after surgery, retinal thickening and associated visual dysfunction may still remain, making long-term follow-up important. Long-term results show that improvement persists up to 3 years postoperatively and stability is maintained up to 10 years 17). The degree of preoperative retinal deformation and EZ integrity influence the prognosis for recovery.
The formation of epiretinal membrane is understood as a wound-healing-like reaction that proceeds through the following stages 11).
PVD and residual vitreous cortex: During PVD, some vitreous cortex remains on the ILM.
Microbreaks in the ILM (conventional hypothesis): Traction from the residual vitreous cortex creates small breaks in the ILM.
Cell migration: Retinal glial cells (Müller cells, astrocytes), RPE cells, and macrophages migrate through the ILM breaks into the vitreous cavity.
Proliferation and fibroblast differentiation: The migrated cells proliferate and differentiate into fibroblast-like contractile cells, forming the epiretinal membrane.
As the main cellular component of idiopathic ERM, laminocytes (hyalocytes derived from the posterior vitreous membrane) have attracted attention 12). Hyalocytes originate from bone marrow-derived cells and are continuously renewed. Glial cells and hyalocytes differentiate into fibroblasts/myofibroblasts, leading to extracellular matrix formation and fibrosis, resulting in ERM formation. The composition of ERM is diverse, and there are multiple origins and causes.
According to a new hypothesis that does not require ILM breaks, hyalocytes in the residual vitreous cortex on the ILM are activated into myofibroblasts, directly forming and contracting the ERM 12).
In idiopathic cases, proliferation of fibroblasts, myofibroblasts, glial cells, macrophages, inflammatory cells, vitreous cells, and retinal pigment epithelial cells in the vitreous cortex, along with changes in the extracellular matrix, leads to the formation of membrane tissue.
In secondary cases, disruption of the blood-retinal barrier releases cytokines, causing retinal pigment epithelial cells and glial cells to proliferate on the vitreous cortex or internal limiting membrane, forming a membrane.
Vascular effects: Traction by the epiretinal membrane reduces the foveal avascular zone (FAZ) area and significantly increases the vessel area density (VAD) of the superficial capillary plexus (SCP) 2). A significant inverse correlation (r = −0.683) is observed between FAZ area and best-corrected visual acuity (BCVA) 2), making FAZ morphology an important indicator of visual function.
In NF2-associated epiretinal membranes, loss of function of the tumor suppressor gene leads to abnormal proliferation of Müller cell-like glial components, forming an epiretinal membrane. Immunostaining shows a pattern of weak GFAP positivity and moderate nestin positivity 9).
7. Latest Research and Future Perspectives (Investigational Reports)
In an RCT by Ducloyer et al. (2024) involving 213 eyes (101 spontaneous peeling, 51 active ILM peeling, 49 no peeling), the recurrence rate was 0% in the active peeling group vs. 19.6% in the no-peeling group, showing a significant difference 18). However, recovery of BCVA and microperimetry was slightly delayed in the active ILM peeling group. The trade-off between recurrence prevention and visual function recovery requires further long-term outcome evaluation.
In a report by Elhusseiny et al. (2020) on 49 eyes with a mean follow-up of 111 months (approximately 9.3 years), BCVA improved from 0.56 preoperatively to 0.33 at 1 year, 0.25 at 3 years, and 0.28 at 10 years, showing sustained improvement up to 3 years and stability up to 10 years 17). Early surgical intervention is supported from the perspective of long-term visual function maintenance.
Preoperative and Postoperative Vascular Flow Assessment Using OCTA
Frisina et al. (2023) confirmed using OCTA that in eyes with idiopathic epiretinal membrane, the FAZ area is reduced to about half that of healthy eyes (0.11 mm² vs. 0.24 mm²), and the VAD of the SCP is significantly increased 2). They also reported a significant inverse correlation between FAZ area and BCVA (r = −0.683), indicating that OCTA is a promising preoperative prognostic tool. logMAR visual acuity significantly improved from 0.4 to 0.1 postoperatively.
Preoperative Prediction of ILM Defects Using en face OCT
Sasajima and Zako (2023) reported that preoperative en face OCT revealed ILM defects in 22.7% of cases, and the defect-edge technique for peeling from the ILM defect margin was safe and effective 1). Identifying the defect site preoperatively is expected to improve the accuracy of surgical planning.
AI-based diagnosis of ERM from fundus photographs or ophthalmoscopy is under evaluation 12). It has been noted to have advantages in terms of cost and accessibility, and its use in screening is anticipated. However, diagnostic accuracy verification is still ongoing, and OCT remains the de facto standard for ERM diagnosis.
Giachos et al. (2021) reported a case of intraretinal neovascularization triggered by epiretinal membrane traction in a patient without diabetes 6). OCTA enables detailed evaluation of the vessels, and the neovascularization was confirmed to regress after epiretinal membrane surgery.
Venkatesh et al. (2022) reported a case of macular damage due to the combination of BBG and endoillumination light 10), highlighting the importance of limiting exposure time and appropriate light intensity management when using BBG. Establishing a safe staining protocol remains a future challenge.
Recognition and Prevention of PAMM-like Complications
Koiwa et al. (2024) reported a case of PAMM-like parafoveal retinal ischemia after vitrectomy for epiretinal membrane 5), pointing out that preoperative blood flow assessment and intraoperative intraocular pressure management are important for preventing complications.
Sasajima H, Zako M. A useful technique of starting internal limiting membrane peeling from the edge of the internal limiting membrane defect in epiretinal membrane surgery. Clin Case Rep. 2023;11(5):e7279. doi:10.1002/ccr3.7279. PMID:37155426; PMCID:PMC10122716.
Frisina R, De Salvo G, Tozzi L, et al. Effects of physiological fluctuations on the estimation of vascular flow in eyes with idiopathic macular pucker. Eye (Lond). 2023;37(7):1470-1478. doi:10.1038/s41433-022-02158-4. PMID: 35794376.
Mashayekhi A, Shields CL, Shields JA, et al. Malignant Epiretinal Membrane After Proton Beam Radiation of Ciliary Body Melanoma. J Ophthalmic Vis Res. 2023;18(4):445-451. doi:10.18502/jovr.v18i4.14558. PMID:38250230; PMCID:PMC10794798.
Munoz-Solano J, Preziosa C, Staurenghi G, Pellegrini M. Resolution of epiretinal membrane after anti-VEGF and photodynamic therapy of retinal hemangioblastoma. Am J Ophthalmol Case Rep. 2024;33:101994. doi:10.1016/j.ajoc.2024.101994. PMID: 38303898. PMCID: PMC10831802.
Koiwa C, Chi P, Yamamoto S, Nakao S. Extramacular paracentral acute middle maculopathy-like retinal ischemia after vitrectomy for epiretinal membrane. Am J Ophthalmol Case Rep. 2024;36:102221. doi:10.1016/j.ajoc.2024.102221. PMID: 39634097. PMCID: PMC11615521.
Ioannis Giachos, Evangelia Chalkiadaki, Konstantinos Andreanos, Chrysanthos Symeonidis, Alexandros Charonis, Ilias Georgalas, Tryfon Rotsos. Epiretinal membrane-induced intraretinal neovascularization. American Journal of Ophthalmology Case Reports. 2021;23:101180. doi:10.1016/j.ajoc.2021.101180.
Alshahrani ST, Alshahrani ST, Arevalo JF. Epiretinal membrane after branch retinal vein occlusion: Separation after dexamethasone implant injection. Am J Ophthalmol Case Rep. 2022;25:101252. doi:10.1016/j.ajoc.2021.101252.
Rivera-Valdivia N, et al. RPE atrophy after ERM/ILM peeling. Rom J Ophthalmol. 2022;66(1):79-83.
Kunikata H, Nishiguchi KM, Watanabe M, Nakazawa T. Surgical outcome and pathological findings in macular epiretinal membrane caused by neurofibromatosis type 2. Digit J Ophthalmol. 2022;28(1):12-16. doi:10.5693/djo.02.2021.06.001. PMID: 35573141.
Venkatesh R, Gupta A, Yadav NK, Chhablani J. Presumed Combined Brilliant Blue G and Endolight-Induced Macular Damage following Epiretinal Membrane Removal Surgery. J Curr Ophthalmol. 2022;34(2):267-270. doi:10.4103/joco.joco_46_22. PMID:36147266. PMCID:PMC9487014.
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, Ying GS. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern®. Ophthalmology. 2020;127(2):P145-P183. doi:10.1016/j.ophtha.2019.09.022. PMID:31757497.
Bailey ST, Vemulakonda GA, Kim SJ, Kovach JL, Lim JI, Ying GS, Flaxel CJ, American Academy of Ophthalmology Preferred Practice Pattern Retina/Vitreous Committee. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P197-P233. doi:10.1016/j.ophtha.2024.12.019. PMID:39918520.
Xiao W, Chen X, Yan W, et al. Prevalence and risk factors of epiretinal membranes: a systematic review and meta-analysis of population-based studies. BMJ Open. 2017;7:e014644. doi:10.1136/bmjopen-2016-014644. PMID: 28951399.
Fraser-Bell S, Guzowski M, Rochtchina E, et al. Five-year cumulative incidence and progression of epiretinal membranes: the Blue Mountains Eye Study. Ophthalmology. 2003;110(1):34-40. PMID: 12511343.
Meuer SM, Myers CE, Klein BE, Swift MK, Huang Y, Gangaputra S, et al. The epidemiology of vitreoretinal interface abnormalities as detected by spectral-domain optical coherence tomography: the beaver dam eye study. Ophthalmology. 2015;122(4):787-95. doi:10.1016/j.ophtha.2014.10.014. PMID:25556116; PMCID:PMC4372472.
Ng CH, Cheung N, Wang JJ, et al. Prevalence and risk factors for epiretinal membranes in a multi-ethnic United States population. Ophthalmology. 2011;118(4):694-699. doi:10.1016/j.ophtha.2010.08.009.
Ducloyer JB, et al. Pros and cons of internal limiting membrane peeling during epiretinal membrane surgery: a randomised clinical trial with microperimetry (PEELING). Br J Ophthalmol. 2024. doi:10.1136/bjo-2023-324990. PMID: 38901960.
Chang WC, Lin C, Lee CH, Sung TL, Tung TH, Liu JH. Vitrectomy with or without internal limiting membrane peeling for idiopathic epiretinal membrane: A meta-analysis. PLoS One. 2017;12(6):e0179105. doi:10.1371/journal.pone.0179105. PMID:28622372. PMCID:PMC5473547.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.