This test records the electrical potential changes of the retina induced by light stimulation using electrodes placed on the cornea or skin. It non-invasively and objectively measures electrical signals that combine currents from retinal neurons and contributions from glial cells. It is very useful and considered essential for diagnosing inherited retinal degenerative diseases.
1967: Ragnar Granit received the Nobel Prize for his research on dark-adapted cat retina
1989/2022: ISCEV (International Society for Clinical Electrophysiology of Vision) established and updated standard recording protocols9)
QWhat eye diseases can be diagnosed with electroretinography?
A
It is used to diagnose a variety of hereditary and acquired retinal diseases. These include retinitis pigmentosa, congenital stationary night blindness (CSNB), Leber congenital amaurosis (LCA), cone-rod dystrophy, vitamin A deficiency night blindness, autoimmune retinopathy (AIR), metabolic diseases (cblC type methylmalonic acidemia), and mucopolysaccharidosis (MPS). For the designated intractable disease application for retinitis pigmentosa, ERG is a mandatory test included in the diagnostic criteria.
The indications for ERG testing differ between full-field ERG and multifocal/macular ERG.
Type of ERG
Main indications/conditions
Full-field ERG
Suspected hereditary retinal degeneration, retinal vascular disorders, ischemic diseases, unexplained vision loss or visual field defects, when fundus examination is difficult
ERG findings vary by disease. Typical patterns are shown below.
Rod-dominant dysfunction
Retinitis pigmentosa (RP): Rod responses disappear early, with generalized loss as the disease progresses. ERG (reduced, negative, or extinguished) is a required finding for RP designated intractable disease application. 7)
Vitamin A deficiency (VAD) night blindness: Scotopic response loss at DA 0.01, reduced a-wave and b-wave amplitudes at DA 3.0/DA 10.0, marked reduction of oscillatory potentials. Cone responses show delayed implicit time. 1)
Autoimmune retinopathy (AIR): Both rod and cone responses are reduced to absent. The AAO Task Force (2025) diagnostic criteria include reduced rod and cone responses on ffERG. 3)
Cone dystrophy: Only the cone response is absent. Some cases cannot be diagnosed without ERG.
Occult macular dystrophy (OMD): Full-field ERG is normal, but abnormalities can be detected by macular focal ERG.
Metabolic disease (cblC type methylmalonic acidemia): Reduced amplitudes of scotopic and photopic components. Useful for monitoring progression of maculopathy. 2)
Mucopolysaccharidosis (MPS): Rod-mediated retinopathy progresses to rod-cone dystrophy over 7 years. ERG abnormalities precede fundoscopic findings. 6)
In typical RP, rod responses diminish before cone responses. If cone responses are predominantly impaired, cone dystrophy should be suspected. 7)
Before performing genetic testing for IRD (inherited retinal dystrophy), confirmation of the clinical phenotype by ERG plays an important role. 8)
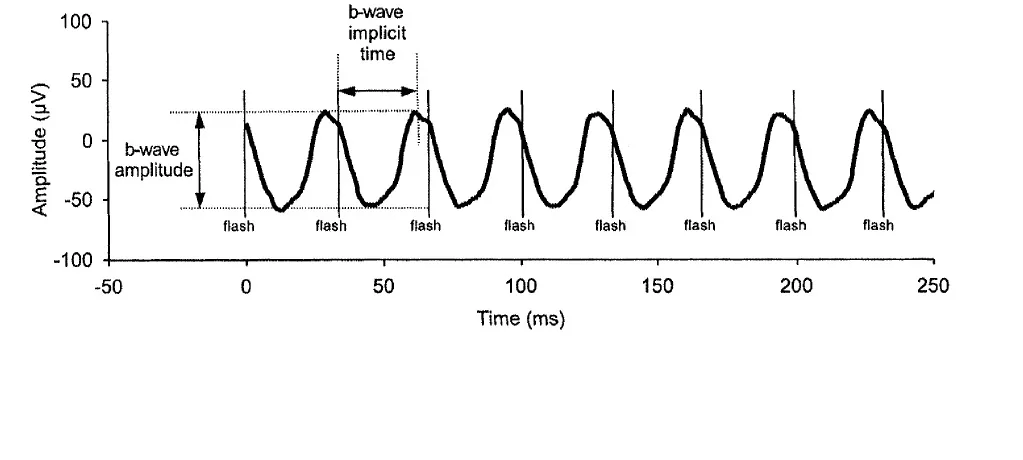
Representative waveform of standard photopic full-field ERG in a healthy subject, illustrating the measurement definitions of amplitude (µV) and peak latency (ms) for the negative a-wave and positive b-wave. This corresponds to the a-wave and b-wave components of the ISCEV standard waveform discussed in section “3. Types and principles of ERG”.
ERG is classified by recording method. Full-field ERG uses a Ganzfeld dome to stimulate the entire retina with light and records the summed response from multiple retinal sources.
Five standard waveforms defined by ISCEV (2022 update9)):
1. Rod response (DA 0.01)
Recorded after at least 20 minutes of dark adaptation with a weak light stimulus. Under dark-adapted conditions, cones do not respond; only rod system cells respond. A slow positive wave (rod b-wave) is recorded. The origin of this b-wave is mainly rod ON bipolar cells.
2. Standard combined response (DA 3.0)
Recorded after at least 20 minutes of dark adaptation with a strong light stimulus. Both cone and rod systems respond. It consists of three components: an initial negative wave (a-wave), followed by a positive wave (b-wave), and oscillatory potentials (OPs) on the rising limb of the b-wave. The a-wave originates from photoreceptors, and the b-wave mainly from bipolar cells.
3. Oscillatory potentials (OPs)
High-frequency components riding on the b-wave ascending limb. When extracted with a frequency band of 75–300 Hz, only the oscillatory potentials are recorded. Their origin is near the inner plexiform layer (e.g., amacrine cells). Reduced amplitude or delayed latency suggests retinal blood flow impairment.
4. Single-flash cone response (LA 3.0)
Recorded with a background light to suppress rods while stimulating with light. The a-wave originates from cone photoreceptors and cone OFF bipolar cells, and the b-wave mainly from cone ON bipolar cells.
5. 30 Hz flicker response
Uses rapid flickering light stimuli that rods cannot follow, recording only cone responses. The waveform resembles a sine wave.
This is a negative wave observed after the b-wave of the cone ERG. It contains potentials derived from retinal ganglion cells and retinal nerve fibers, and the PhNR is reduced in cases of optic atrophy. It is applied in the evaluation of glaucoma and optic nerve diseases.
ON-OFF Response
This is a cone ERG recorded using long-duration light stimulation of 100–200 ms. The origin of the ON response is mainly cone ON-type bipolar cells, and the origin of the OFF response is mainly cone OFF-type bipolar cells. In complete CSNB, the OFF response is normal but only the ON response is reduced.
The retina is stimulated and recorded using a pattern consisting of an array of 61 to 103 hexagons. Local responses within the central 30 degrees are recorded simultaneously, allowing detailed evaluation of macular dysfunction. It is also used for hydroxychloroquine toxicity assessment10).
Evaluates the activity of retinal ganglion cells (RGC) in the macula. It consists of three components: N35, P50, and N95. Transient pERG is recorded with reversal stimulation at 4 reversals per second.
This is an ERG recorded by stimulating the macular area with a circular light of 5°, 10°, or 15° in size while observing the fundus with an infrared fundus camera. It is particularly useful for diagnosing conditions such as occult macular dystrophy (OMD), where abnormalities can be detected by focal macular ERG even when full-field ERG is normal.
QWhat is the difference between ffERG and mfERG?
A
ffERG records the summed response of the entire retina and is suitable for detecting widespread dysfunction (e.g., retinitis pigmentosa, toxic retinopathy). mfERG simultaneously records local responses at 61 to 103 locations within the central 30 degrees and specializes in evaluating localized dysfunction within the macula. Small macular lesions that cannot be detected by ffERG may be detected by mfERG.
4. Examination Procedure and Implementation Method
Avoid strong illumination such as fundus photography and fluorescein angiography (FAG) before the examination (if unavoidable, ensure at least 30 minutes of recovery under room lighting).
Perform maximum pupillary dilation and record the pupil diameter before the examination.
Dark adaptation for 20 minutes, light adaptation for 10 minutes.
Insert the contact lens electrode under dim red light after dark adaptation, and ensure an additional 5 minutes of dark adaptation.
Photograph of a clinical scene where a patient with electrodes attached is undergoing electroretinography in a dark room, showing the placement of corneal and reference electrodes and the light-shielded environment. This corresponds to the electrode placement and examination environment settings discussed in the section “4. Examination Procedures and Methods.”
Place the ground electrode on the earlobe.
Place the reference electrode (−) on the forehead.
Place the corneal electrode (or skin electrode).
Record ERG under dark adaptation (rod response → maximal response → OPs).
Record ERG after light adaptation (about 10 minutes) (cone response → flicker).
Compare the characteristics of the main recording electrodes.
Electrode name
Material/Shape
Features
BA electrode
PMMA contact lens
Reusable, various sizes available
DTL electrode
Silver/nylon thread
Disposable, high comfort
Jet electrode
Gold-plated plastic
Disposable
Skin electrode
Placed under the lower eyelid
Well tolerated in children
Corneal electrodes (contact lens electrodes) are highly sensitive and used as standard electrodes, but they require topical anesthesia and are suitable for upper elementary school students and older, including adults.
The amplitude of ERG recorded with skin electrodes is about 1/4 to 1/5 of that with corneal electrodes, but full standard responses can be recorded. Representative skin electrode ERG devices include the LE-4000 (Tomey Service Corporation) and RETeval® (LKC Technologies). RETeval® allows placement of three electrodes (recording, reference, ground) by simply attaching a single sticker to the lower eyelid.
In electrophysiological testing, especially in children, subjective functional tests (visual acuity, visual field) have low reliability, increasing the importance of objective tests.
Situations where ERG is particularly necessary in children:
When there is opacity of the ocular media that prevents clear visualization of the fundus
When the cause of decreased visual acuity is unknown
In infants and uncooperative patients, selection of recording electrodes and recording under sedation are important.
In infants, skin electrodes and recording under sedation improve diagnostic feasibility 4)
The diagnostic workflow for pediatric IRD includes ffERG ± pattern/mfERG 4)
In the evaluation of infantile nystagmus, to detect sensory system diseases including LCA and other retinal dystrophies, ancillary tests including ERG are selected based on ophthalmic findings 5)
QHow is electroretinography performed in children?
A
In infants and uncooperative children, skin electrodes (placed on the lower orbital rim) or recording under sedation can improve diagnostic feasibility. Infants can also be examined while lying supine on a parent’s lap. Skin electrodes yield smaller amplitudes, so interpretation based on facility-specific reference values and test conditions is necessary. 4)
5. Clinical Application and Monitoring of Test Results
Early RP may be difficult to diagnose based on fundus findings alone, and ERG is key to diagnosis. For new applications for designated intractable diseases of RP, confirmation of ERG abnormalities (reduced, negative, or extinguished type) is included as a mandatory test in the certification criteria. 7)
In typical RP, rod responses diminish before cone responses. If cone responses are predominantly impaired, cone dystrophy should be suspected. 7)
Before performing genetic testing for IRD (inherited retinal dystrophy), it is important to establish a clinical diagnosis using ERG. ERG plays a key role in confirming the phenotype of IRD 8).
ERG Monitoring of Vitamin A Deficiency (VAD) Night Blindness
The effect of vitamin A supplementation for vitamin A deficiency night blindness can be evaluated over time using ERG.
Poornachandra et al. (2022) reported serial ERG findings before and after vitamin A supplementation (intramuscular 100,000 units/day × 3 days → oral 50,000 units/day × 2 weeks) in two cases: a 20-year-old man with intestinal lipofuscinosis and a 50-year-old man with alcoholic liver disease (both with serum vitamin A 0.02 mg/mL, normal 0.3–0.6 mg/mL) 1). Before treatment, ERG showed absent scotopic responses under DA 0.01, reduced a-wave and b-wave amplitudes under DA 3.0/DA 10.0, and markedly reduced oscillatory potentials. Improvement in scotopic responses began 1 week after treatment, and nearly normalized after 1 month.
Key insights from ERG:
Rods depend on vitamin A supply from the RPE and are affected earlier and more extensively than cones 1)
The order of functional recovery is cones → peripheral rods → parafoveal rods 1)
If no response improvement is seen after 1 week of treatment, reconsider causes other than VAD 1)
ERG Monitoring of cblC-Type Methylmalonic Acidemia
Michieletto et al. (2025) reported a case of cblC-type methylmalonic acidemia detected by newborn screening 2). Treatment was started at 8 days of life (OHCbl 1 mg intramuscular/day, betaine 100 mg × 3/day, folic acid 5 mg × 2/week), but at 7 months, ffERG showed reduced amplitudes of scotopic and photopic components, and bull’s eye maculopathy appeared around the same time. Retinal degeneration progressed despite treatment.
Implications for management of cblC patients:
ERG is recommended even in cblC patients without apparent maculopathy 2)
High-dose OHCbl (6.5 ± 3.3 mg/kg/day) has been reported to be associated with better ocular outcomes 2)
Confirmation of reduced rod and cone responses by ffERG constitutes one of the diagnostic criteria.
Chen et al. (2025) reported a total of 7 cases including 3 cases of autoimmune retinopathy (AIR) in patients with myasthenia gravis (MG) 3). In all cases, ERG showed rod and cone dysfunction. Despite improvement in MG with immunosuppressive therapy in 6 ARA-positive cases, visual deterioration continued.
6. Pathophysiology: Mechanisms of Each Waveform Component
A negative-type ERG, where a normal a-wave is combined with a reduced b-wave, indicates that signal transmission from the inner nuclear layer onward is impaired even though photoreceptors are normal. In complete CSNB, the b-wave in DA 0.01 disappears due to ON bipolar cell dysfunction 4).
MMACHC protein deficiency → impaired conversion of vitamin B12 to adenosylcobalamin and methylcobalamin → accumulation of methylmalonic acid (MMA) and homocysteine (Hcy) 2)
Photoreceptors, RPE, and Müller cells in the outer retina have high mitochondrial density and are vulnerable to metabolic impairment 2)
Foveal development progresses from birth to early childhood, making this period vulnerable to toxic accumulation of Hcy and MMA 2)
A small report on high-dose OHCbl therapy (0.4–2.7 mg/kg/day) found that 5 of 6 treated patients did not develop maculopathy/retinopathy. In a historical cohort (0.3 mg/kg/day), all 27 patients developed maculopathy 2). Another report of 4 cases showed that high-dose therapy (mean 6.5±3.3 mg/kg/day) initiated before 5 months of age resulted in favorable ophthalmic and cognitive outcomes 2).
The AAO Task Force (2025) established guidelines for the diagnosis, management, and research of AIR, positioning reduced rod and cone responses on ffERG as one of the diagnostic criteria 3). Standardization of anti-retinal antibody (ARA) detection methods remains a future challenge 3).
Voretigene neparvovec has been approved for LCA and RP associated with RPE65 gene mutations, and ERG is used to evaluate retinal function after gene therapy. Changes in ERG before and after treatment are gaining importance as objective indicators of therapeutic efficacy.
Poornachandra B, Jayadev C, Sharief S, et al. Serial ERG monitoring of response to therapy in vitamin A deficiency related night blindness. BMJ Case Rep. 2022;15:e247856.
Michieletto P, Baldo F, Madonia M, Zupin L, Pensiero S, Bonati MT. Retinal Changes in Early-Onset cblC Methylmalonic Acidemia Identified Through Expanded Newborn Screening: Highlights from a Case Study and Literature Review. Genes. 2025;16(6). doi:10.3390/genes16060635. PMID:40565527; PMCID:PMC12193327.
Chen Y, Zhang Y, Luo J, Liu M, Lin M, Zhu W, et al. Autoimmune retinopathy in patients with myasthenia gravis: cases series and literature review. BMC ophthalmology. 2025;25(1):521. doi:10.1186/s12886-025-04357-5. PMID:41029312; PMCID:PMC12487295.
Mordà D, et al. Pediatric inherited retinal dystrophies: a comprehensive review. Prog Retin Eye Res. 2025;109:101405.
Bertsch M, Floyd M, Kehoe T, Pfeifer W, Drack AV. The clinical evaluation of infantile nystagmus: what to do first and why. Ophthalmic Genet. 2017;38(1):22-33. doi:10.1080/13816810.2016.1266667.
Collin RJ, et al. Retinopathy in mucopolysaccharidoses. Ophthalmology. 2025;132(4):470-.
厚生労働科学研究費補助金難治性疾患等政策研究事業 網膜脈絡膜・視神経萎縮症に関する調査研究班. 網膜色素変性診療ガイドライン [Clinical Practice Guidelines for Retinitis Pigmentosa]. 日眼会誌. 2016;120(12):846-861. PMID:30079711.
Robson AG, Frishman LJ, Grigg J, et al. ISCEV Standard for full-field clinical electroretinography (2022 update). Doc Ophthalmol. 2022;144(3):165-177.
Hood DC, Bach M, Brigell M, et al. ISCEV standard for clinical multifocal electroretinography (mfERG) (2011 edition). Doc Ophthalmol. 2012 Feb;124(1):1-13. doi:10.1007/s10633-011-9296-8. PMID:22038576; PMCID:PMC4466109.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.