Acute zonal occult outer retinopathy (AZOOR) is an acute inflammatory disease proposed and established by Gass in the 1990s 3). It is characterized by acute visual field defects, photopsia, and vision loss despite nearly normal fundus findings. The main pathology involves photoreceptors and the outer retina, hence the name “occult” outer retinopathy.
The Japanese Ophthalmological Society has established diagnostic guidelines for AZOOR, defining severe cases as corrected visual acuity < 0.3 in the better eye. AZOOR is also included in the differential diagnosis table (Table 3) of the AZOOR complex in the Uveitis Clinical Practice Guidelines (J Jpn Ophthalmol Soc 2019;123(6):635-696) 1). When visual field abnormalities cannot be explained by fundus findings, AZOOR should always be considered in the differential diagnosis.
AZOOR is positioned as one disease within the AZOOR complex (MEWDS, AZOOR, AMN, PIC, MFC, AIBSE, AAOR), and these diseases are understood as a continuum (spectrum) of inflammatory disorders primarily affecting the outer retina, photoreceptors, and RPE1)2). Advances in multimodal imaging have deepened the integrated understanding of the pathophysiology of the AZOOR complex 2).
The following AZOOR variants have been reported 1):
About 3/4 of patients are women, predominantly young adults around mid-30s
Unilateral onset in 61%, with median 8-year follow-up eventually 76% become bilateral
Onset in the fellow eye is delayed by an average of 50 months
Association with autoimmune diseases: Hashimoto’s disease (most common), multiple sclerosis1)
About 20% of cases have flu-like prodromal symptoms
Regarding clinical features in Japanese patients, a cohort study of Japanese AZOOR cases (Saito S et al., 2015) has been reported, examining the natural course of visual function and prognostic factors 4).
QWhy does vision decrease even though the fundus appears normal?
A
The main site of damage in AZOOR is the photoreceptors (outer retina, ellipsoid zone). Even if the fundus appears normal, OCT shows loss of the ellipsoid zone (IS/OS line) corresponding to the visual field defect. Disruption of the photoreceptor inner/outer segment junction causes visual dysfunction, leading to decreased visual acuity and visual field defects even with a normal-appearing fundus.
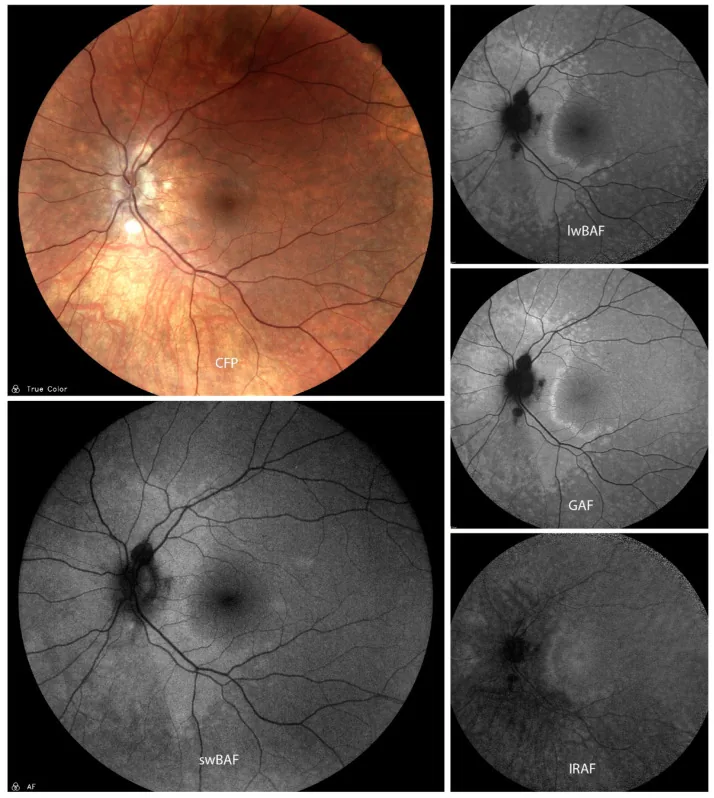
Mauschitz MM, et al. Fundus Autofluorescence in Posterior and Panuveitis-An Under-Estimated Imaging Technique: A Review and Case Series. Biomolecules. 2024. Figure 5. PMCID: PMC11118036. License: CC BY.
Color fundus photograph (CFP) of acute posterior multifocal placoid pigment epitheliopathy (APMPPE) and various autofluorescence images including swBAF (450 nm), lwBAF (488 nm), GAF (518 nm), and IRAF (787 nm) show hypoautofluorescent lesions with hyperautofluorescent borders. This corresponds to the fundus autofluorescence abnormalities discussed in the section “2. Main symptoms and clinical findings.”
Photopsia: One of the most characteristic symptoms. Acute onset.
Acute vision loss and visual field defects (one to several areas) 1)
Enlargement of the Mariotte blind spot, central visual field defects, peripheral visual field defects 1)
Prodromal symptoms: Flu-like symptoms (in about 20% of cases)
Visual field defects often appear as band-shaped or sectoral defects, and because the fundus appears normal, it may be misdiagnosed as optic neuritis1). Goldmann perimetry reveals marked enlargement of the Mariotte blind spot or sectoral scotomas.
The fundus is essentially normal, making differentiation from optic neuritis difficult in some cases 1). An important feature of AZOOR is that fluorescein angiography (FA) usually shows no abnormalities. In long-standing cases, diffuse or sectoral chorioretinal atrophy may appear.
At onset
Fundus: Nearly normal. No anterior chamber or vitreous inflammation. FA usually shows no abnormalities.
OCT: Loss of the ellipsoid zone (IS/OS) and interdigitation zone corresponding to the visual field defect. Outer layer loss indicates no potential for functional recovery and is useful for prognosis 5).
Full-field ERG: Reduced amplitudes in cases with extensive damage. Cone system abnormalities > rod system.
Multifocal ERG: Reduced amplitudes corresponding to the visual field defect. Particularly useful for detecting small lesions 1).
Chronic phase
Fundus atrophy: Diffuse or sectoral chorioretinal atrophy may appear in some cases7).
ERG changes: ERG may improve with treatment or spontaneous recovery in some cases.
OCT changes: Partial recovery of the ellipsoid zone may be observed, but persistent loss of the outer layers indicates poor visual prognosis8).
Visual field changes: In cases of spontaneous recovery, reduction of visual field defects may be observed.
QHow is AZOOR different from optic neuritis?
A
The most important differential diagnosis is optic neuritis. In AZOOR, the fundus is almost normal, and optic disc swelling or hyperemia is often absent. Reduced amplitude on ERG (especially multifocal ERG) is characteristic of AZOOR, while ERG is usually normal in optic neuritis. Also, photopsia is often prominent in AZOOR, and eye movement pain is typically absent1).
In addition, when presenting with unilateral temporal hemianopia, it is due to nasal retinal damage and may appear as temporal hemianopia respecting the vertical meridian, thus mimicking chiasmal lesions and sometimes requiring MRI12). RAPD (relative afferent pupillary defect) may appear during the course in some cases.
The cause is unknown, but viral infection or autoimmune involvement are the main hypotheses.
Approximately 20% of cases have flu-like prodromal symptoms → viral infection trigger hypothesis
Association with Hashimoto’s disease and multiple sclerosis → autoimmune mechanism hypothesis1)
Main sites of damage: photoreceptors (ellipsoid zone), RPE, choriocapillaris (various theories)
Regarding the main lesion site in AZOOR, there are various theories including photoreceptors, retinal pigment epithelium, and choriocapillaris, and no conclusion has been reached yet. Loss of the ellipsoid zone on OCT directly reflects disruption of the inner segment/outer segment junction (IS/OS line), and functional recovery in that area is often difficult8).
Genetic predisposition as part of AZOOR complex + environmental factors (viral infection, autoimmune trigger)2)
Epilepsy: Rat studies have shown that epileptic seizures induce inflammatory responses in the retina, suggesting a possible association13)
After scleral buckling surgery: Case reports of AZOOR-like findings appearing more than 5 years postoperatively14)
Among Gass’s 51 cases, approximately 28% had a history of autoimmune disease. In addition to Hashimoto’s disease and multiple sclerosis, comorbid conditions include Graves’ disease, hypothyroidism, Addison’s disease, myasthenia gravis, Crohn’s disease, and SLE. Anti-retinal antibodies are detected in about 42% of AZOOR patients15).
AZOOR is suspected in young individuals aged 20–50 who present with acute unilateral vision loss, visual field defects, and photopsia. Diagnosis is made by combining OCT and ERG. When visual field abnormalities cannot be explained by fundus findings, it is important to actively consider AZOOR in the differential diagnosis.
In relatively young patients in their 20s to 50s who present with acute unilateral vision loss, visual field defects, and photopsia, OCT should be performed first. If OCT shows abnormalities in the outer retinal layers corresponding to the visual field defect, AZOOR is strongly suspected. Subsequently, ERG and multifocal ERG are used for confirmation1).
May show reduced light rise and decreased Arden ratio
OCT is also useful for prognosis prediction. In areas where the outer layer (ellipsoid zone) is absent, functional recovery cannot be expected, so OCT evaluation of the outer layer provides a basis for treatment decisions and prognosis explanation 5). When the affected area is small, multifocal ERG or focal ERG is more useful for diagnosis than full-field ERG1).
Differential Diagnosis (Uveitis Clinical Practice Guideline Table 3) 1)
Subacute to chronic onset, diffuse hyperautofluorescence on FAF, normal EOG
Syphilitic outer retinopathy (SOR)
Very similar to AZOOR. Syphilis serology is essential 1)
To rule out infectious causes, testing for syphilis, CMV, VZV, and HSV is performed. If temporal hemianopia is present, MRI is used to exclude chiasmal lesions 12).
QWhat test is essential for diagnosing AZOOR?
A
The combination of OCT and multifocal ERG is key to diagnosis. OCT shows loss of the ellipsoid zone corresponding to visual field defects, and multifocal ERG shows reduced amplitudes in the same areas. Full-field ERG is useful for assessing widespread damage, and FA is typically normal, which helps differentiate from other posterior uveitis1). Adaptive optics (AO) fundus imaging can visualize abnormal photoreceptor arrangement in affected areas.
There is no established treatment, and cases include both spontaneous recovery and poor visual prognosis.
Mild cases: Observation without treatment
Severe cases (best-corrected visual acuity in the better eye < 0.3): Consider steroid pulse therapy
Since autoimmunity and inflammation are thought to be involved in the etiology, steroid pulse therapy may be considered, especially in severe cases. However, it is difficult to distinguish whether recovery is due to spontaneous remission or the effect of steroids.
1,000 mg + Solita-T3 500 mL intravenously over 1 hour, for 3 days
Oral (maintenance therapy)
Prednisolone (Predonine®) tablets 5 mg
8 to 6 tablets (40 to 30 mg) in 2 divided doses, then taper
The effect of steroid pulse therapy is difficult to distinguish from natural recovery, and evidence is limited to case reports. No randomized controlled trials (RCTs) exist at present.
Intravitreal steroid injection has also been reported, but attention must be paid to the risk of side effects such as cataracts, increased intraocular pressure, and central serous chorioretinopathy (CSR)16).
In cases of recurrence or chronicity, consider adding immunosuppressive agents (e.g., cyclosporine). Management based on treatment for AZOOR complex-related diseases may be referenced.
QDoes steroid therapy improve visual acuity?
A
There are case reports of efficacy with steroid pulse therapy, but no randomized controlled trials exist, and it is difficult to distinguish from spontaneous recovery. It may be considered only in severe cases (best-corrected visual acuity in the better eye < 0.3), but visual prognosis is poor in cases where outer retinal loss persists despite treatment. Functional recovery is often difficult in areas where the ellipsoid zone is absent on OCT8).
Loss of the ellipsoid zone on OCT directly reflects disruption of the photoreceptor inner segment/outer segment junction (IS/OS line). In areas where this zone is absent, photoreceptor recovery is difficult, leading to long-term visual dysfunction 5)8). In mild cases or during the recovery phase, only the interdigitation zone may be abnormal while the ellipsoid zone is preserved.
Viral infection (about 20% have flu-like prodromal symptoms) or autoimmunity (associated with Hashimoto’s disease or multiple sclerosis) may be involved.
Primary lesion site: photoreceptor inner segment/outer segment junction (ellipsoid zone). Its loss on OCT directly reflects the damage.
There are various theories regarding the involvement of the choriocapillaris, but on OCT-A, the choriocapillaris is often preserved or shows only minimal changes2)
As a disease within the AZOOR complex, it develops due to genetic predisposition plus environmental factors (viral infection, autoimmunity)2)
The AZOOR complex (MEWDS, AZOOR, AMN, PIC, MFC, AIBSE, AAOR) is considered to be a group of related diseases on the same disease spectrum, sharing a common basis of inflammatory disorders primarily affecting the outer retina and RPE2). Jampol and Becker (2003) proposed the hypothesis that these white dot syndromes are based on a common genetic autoimmune/inflammatory mechanism10).
Hashimoto’s disease is the most commonly associated autoimmune disease, followed by multiple sclerosis. These associations suggest an autoimmune attack on photoreceptors and the outer retina, providing important clues for understanding the pathophysiology of AZOOR.
In areas where the ellipsoid zone loss persists, recovery of photoreceptors is difficult, and OCT evaluation directly correlates with long-term prognosis.
Multimodal imaging analysis has shown that the primary lesion site in AZOOR is the photoreceptor outer segment18). ICG angiography shows preservation of the choriocapillaris, indicating that the choroidal capillaries are not initially damaged. Hyperautofluorescence on FAF results from exposure of RPElipofuscin due to loss of photoreceptor outer segments. The choroid is secondarily damaged (collateral damage), leading to chorioretinal atrophy in advanced cases.
Quantitative analysis using adaptive optics fundus imaging (AO-TFI) has confirmed that photoreceptor (PR) density is significantly reduced, while RPE density shows no significant difference, supporting at the cellular level that PRs are the primary target19). Even after EZ recovery, ONL thinning and reduced PR density persist, and there may be a dissociation between morphological recovery and functional impairment.
In a review by Qian et al., it is argued that “AZOOR is a specific form of AIR,” proposing a mechanism in which antibody leakage from the optic disc margin allows immune products to spread into the subretinal space, forming large scotomas contiguous with the optic nerve17).
Integrated understanding of the AZOOR complex: The establishment of a continuum concept sharing a common basis with MEWDS, AMN, PIC, MFC, AIBSE, and AAOR is progressing1)2)
Photoreceptor observation using adaptive optics (AO): Enables visualization of abnormal photoreceptor arrangement in lesions, advancing detailed assessment of lesion extent.
Advances in AO-TFI (adaptive optics fundus imaging): Attracting attention as a non-invasive, in vivo technique for observing and quantifying RPE and photoreceptors at the cellular level19). It provided the first direct evidence that PR density reduction persists even after morphological recovery of the EZ, contributing to the elucidation of the “structure-function dissociation”.
OCT-A choriocapillaris assessment: Research is ongoing to elucidate the involvement of choroidal blood flow2). OCT-A flow void may serve as an indicator for disease evaluation.
Diagnosis and treatment monitoring using OCTA: The starry-sky appearance on en-face outer retinal slab may be useful for diagnostic assistance and treatment response monitoring in AZOOR16).
Disease classification using multimodal imaging: Mrejen et al. (2014) proposed a classification system for AZOOR based on multimodal imaging6). This has advanced the understanding of the relationship between disease type and prognosis.
Recognition and classification of AZOOR variants: Recognition of diverse disease forms, including peripheral-onset variants (centripetal progression, peripapillary sparing), is progressing11).
Association between AZOOR and secondary np-AIR: It has been proposed that progression of AZOOR may cause secondary np-AIR (non-paraneoplastic autoimmune retinopathy), and application to immunotherapy including IVIg is expected17).
Building evidence for steroid therapy: No RCTs currently exist, and accumulation of case reports remains a challenge4).
Long-term prognostic biomarkers: Preservation of the ellipsoid zone on OCT and multifocal ERG patterns are being investigated as indicators to predict differences between spontaneous recovery and progressive cases4)7).
Japanese patient cohort data: Long-term follow-up data of Japanese AZOOR patients by Saito et al. contribute to identifying prognostic factors4)9).
Unresolved issues: Establishment of treatment through RCTs, complete elucidation of etiology (viral vs. autoimmune), verification of prognostic improvement by early intervention, and development of diagnostic biomarkers.
Testi I, Modugno RL, Pavesio C. Multimodal imaging supporting the pathophysiology of white dot syndromes. Journal of ophthalmic inflammation and infection. 2021;11(1):32. doi:10.1186/s12348-021-00261-3. PMID:34529201; PMCID:PMC8446150.
Saito S, Saito W, Saito M, Hashimoto Y, Mori S, Noda K, Namba K, Ishida S.. Acute zonal occult outer retinopathy in Japanese patients: clinical features, visual function, and factors affecting visual function. PLoS One. 2015;10(4):e0125133. doi:10.1371/journal.pone.0125133. PMID:25919689; PMCID:PMC4412707.
Saito W, Kase S, Fujiya A, et al. Multimodal imaging in acute zonal occult outer retinopathy. Br J Ophthalmol. 2019;103(7):908-913.
Mrejen S, Khan S, Gallego-Pinazo R, Jampol LM, Yannuzzi LA.. Acute zonal occult outer retinopathy: a classification based on multimodal imaging. JAMA Ophthalmol. 2014;132(9):1089-1098. doi:10.1001/jamaophthalmol.2014.1683. PMID:24945598.
Gass JD, Agarwal A, Scott IU.. Acute zonal occult outer retinopathy: a long-term follow-up study. Am J Ophthalmol. 2002;134(3):329-339. doi:10.1016/s0002-9394(02)01640-9. PMID:12208243.
Makino S, Tampo H. Changes in optical coherence tomography findings in acute zonal occult outer retinopathy. Case Rep Ophthalmol. 2013;4(3):99-104. doi:10.1159/000355108. PMID:24163675. PMCID:PMC3806683.
Jampol LM, Becker KG. White spot syndromes of the retina: a hypothesis based on the common genetic hypothesis of autoimmune/inflammatory disease. American journal of ophthalmology. 2003;135(3):376-9. doi:10.1016/s0002-9394(02)02088-3. PMID:12614757.
Li D, Kishi S.. Loss of photoreceptor outer segment in acute zonal occult outer retinopathy. Arch Ophthalmol. 2007;125(9):1194-1200. doi:10.1001/archopht.125.9.1194. PMID:17846358.
Ünlü BH, Karti O, Saatci AO.. A Case of an Acute Zonal Occult Outer Retinopathy Variant Characterized With an Insidious Peripheral Onset and Centripetal Progression. Cureus. 2024;16(5):e59600. doi:10.7759/cureus.59600. PMID:38826932; PMCID:PMC11144451.
Ahmed Y, Sayal A, Kaplan AJ, Micieli JA.. Monocular Temporal Hemianopia due to Acute Zonal Occult Outer Retinopathy. Case Rep Ophthalmol. 2022;13(1):44-49. doi:10.1159/000521784. PMID:35350234; PMCID:PMC8921972.
Karska-Basta I, Romanowska-Dixon B, Pojda-Wilczek D, Bakunowicz-Łazarczyk A, Kubicka-Trząska A, Gerba-Górecka K.. Acute Zonal Occult Outer Retinopathy in a Patient Suffering from Epilepsy: Five-Year Follow-Up. Medicina (Kaunas). 2021;57(11):1276. doi:10.3390/medicina57111276. PMID:34833494; PMCID:PMC8624097.
Fung AT, Lo-Cao E, Cornish EE.. Acute zonal occult outer retinopathy-like presentation secondary to scleral buckle. Am J Ophthalmol Case Rep. 2022;28:101716. doi:10.1016/j.ajoc.2022.101716. PMID:36275187; PMCID:PMC9579325.
Roy R, Dutta Majumder P.. Current understanding of acute zonal occult outer retinopathy (AZOOR). Indian J Ophthalmol. 2024;72(7):935-937. doi:10.4103/ijo.ijo_3228_23. PMID:38454854; PMCID:PMC11329826.
Khan S, Saigal K, Moxam J, Maleki A.. A Case of Concomitant Acute Zonal Occult Outer Retinopathy and Secondary Nonparaneoplastic Autoimmune Retinopathy. Case Rep Ophthalmol. 2025;16(1):124-132. doi:10.1159/000543577. PMID:39981532; PMCID:PMC11842096.
Herbort CP, Arapi I, Papasavvas I, Mantovani A, Jeannin B.. Acute Zonal Occult Outer Retinopathy (AZOOR) Results from a Clinicopathological Mechanism Different from Choriocapillaritis Diseases: A Multimodal Imaging Analysis. Diagnostics (Basel). 2021;11(7):1184. doi:10.3390/diagnostics11071184. PMID:34209956; PMCID:PMC8303680.
Iuliano M, Lombardo M, Falsini B, Sebastiani J, D’Ambrosio M, Martelli F, Cusumano A.. Structural, Functional, and Cellular Analysis of a Case of Acute Zonal Occult Outer Retinopathy (AZOOR). Biomedicines. 2025;13(7):1521. doi:10.3390/biomedicines13071521. PMID:40722597; PMCID:PMC12292167.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.