Punctate inner choroidopathy (PIC) is an idiopathic inflammatory choroidal disease first reported by Watzke et al. in 1984. It is classified as one of the white dot syndromes, belonging to a group of inflammatory diseases that affect the outer retina, choriocapillaris, and choroid7). According to the Uveitis Clinical Practice Guidelines (Jpn J Ophthalmol 2019;123(6):635-696), it is categorized as non-infectious posterior uveitis primarily involving the fundus, with characteristics of insidious onset and unilateral or bilateral involvement 8).
It mainly occurs in young myopic women (approximately 90% female) 5). Large studies report a mean age of onset of 36 years and a mean myopic refractive error of −4.5 diopters 5). It preferentially affects young women with moderate myopia. In the acute phase, several small yellow-white lesions appear in the posterior pole, which become atrophic over time.
Punctate inner choroidopathy and multifocal choroiditis (MFC) share involvement of the choroid, retinal pigment epithelium (RPE), and outer retina, suggesting they may represent a spectrum of the same disease 7). The key differentiating features are the presence of vitritis and the distribution of lesions. PIC does not have vitritis and lesions are confined to the posterior pole, whereas MFC has vitritis and lesions extend to the periphery 6).
QHow do punctate inner choroidopathy and multifocal choroiditis (MFC) differ?
A
PIC does not have vitritis and lesions are confined to the posterior pole, whereas MFC has vitritis and anterior chamber inflammation, and lesions extend to the mid-periphery. Both diseases may represent a spectrum of the same condition.
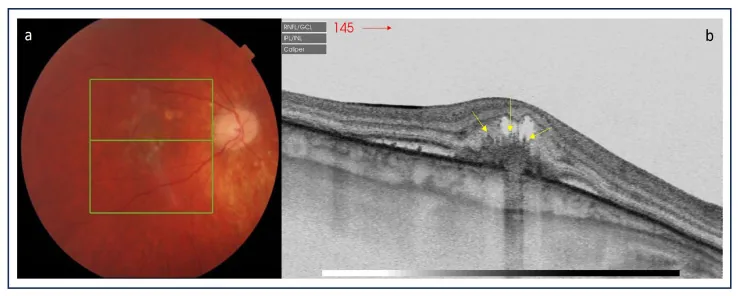
The left fundus photograph shows small yellowish-white lesions in the posterior pole. The right OCT reveals hyperreflective lesions in the macula with subretinal and intraretinal fluid, indicating active PIC lesions.
The most common initial symptoms of punctate inner choroidopathy are unilateral scotoma and decreased visual acuity.
Decreased visual acuity: Visual acuity at initial visit ranges from 0.4 to 0.05. According to reports, about 67% maintained corrected visual acuity of 0.4 or better. During remission, well-defined round atrophic scars with pigmentation remain 8).
Scotoma: Patients notice central or paracentral scotomas.
Photopsia: Flashes of light may be perceived.
Metamorphopsia: Patients may complain of distorted vision.
Fundus findings include 12 to 25 small yellowish-white spots, 100–300 μm in size, localized to the posterior pole and distributed in a random pattern. Lesions occur at the level of the outer retina, RPE, and inner choroid. 80% are bilateral but often asymmetric 1).
The characteristics of punctate inner choroidopathy lesions are summarized below.
Active Lesions
Yellow-white chorioretinal lesions: Small, well-defined yellowish-gray spots in the posterior pole. The peripapillary area is spared.
Absence of intraocular inflammation: Punctate inner choroidopathy is characterized by the absence of anterior chamber inflammation and vitritis 3).
Neurosensory retinal detachment: Serous retinal detachment may occur overlying active lesions.
Scar stage lesions
Atrophic chorioretinal scar: After inflammation subsides, a well-demarcated “punched-out” scar remains. It may be accompanied by pigmentation and a depigmented halo.
Progressive enlargement of scar: Even after inflammation subsides, the scar gradually enlarges, and near the fovea it can cause vision loss.
The etiology of punctate inner choroidopathy is unknown, but it is thought to be an autoimmune disease with a polygenic susceptibility, triggered by environmental stimuli such as infection, vaccination, or stress.
Onset and reactivation of punctate inner choroidopathy after COVID-19 infection have been reported. SARS-CoV-2 infection may induce autoimmune dysregulation in genetically predisposed individuals. Furthermore, relapse of punctate inner choroidopathy after COVID-19 vaccination has also been reported 3).
Scott et al. (2024) reported a case of a 38-year-old woman who experienced relapse of punctate inner choroidopathy with inflammatory choroidal neovascular membrane (iCNVM) 7 days after receiving the Pfizer-BioNTech COVID-19 vaccine. No relapse occurred with vaccination under immunosuppression, but relapse occurred after the fourth dose without immunosuppression 3).
QCan the COVID-19 vaccine worsen punctate inner choroidopathy?
A
Recurrence of punctate inner choroidopathy after COVID-19 vaccination has been reported 3). However, the benefits of vaccination greatly outweigh the risk of ocular inflammation recurrence. Those with a history should consult an ophthalmologist about monitoring before and after vaccination.
The diagnosis of punctate inner choroidopathy is based on clinical findings. Confirmatory diagnosis is made by combining ancillary imaging tests. The histoplasmin skin test is negative.
In FA, active lesions show hyperfluorescence in the early arterial phase and leakage/staining in the late phase 7). More lesions are detected than by clinical examination. CNVM appears as an irregular lacy network of new vessels.
ICG shows mid-phase hypofluorescent lesions in the posterior pole and peripapillary area 7). It detects subclinical hypofluorescent spots in 32% of affected eyes, enhancing diagnostic capability.
SD-OCT is useful for diagnosis and follow-up of punctate inner choroidopathy. Active lesions show focal hyperreflective elevation of the RPE and disruption of the ellipsoid zone (EZ) 7). Choroidal neovascularization (CNV)-positive lesions have greater height, width, and volume compared to CNV-negative lesions, with disruption of the EZ and Bruch’s membrane and obscuration of the outer retina.
Enhanced depth imaging OCT (EDI-OCT) shows increased choroidal thickness directly beneath active lesions, which decreases after treatment (“sponge sign”). This helps differentiate from myopic choroidal neovascularization.
OCTA is an important imaging modality in the diagnosis of punctate inner choroidopathy. It can identify secondary choroidal neovascularization at a high rate, which is difficult to detect with conventional FA or SD-OCT.
Using OCTA, the presence of choroidal neovascularization can be demonstrated in many patients with punctate inner choroidopathy, including cases where FA was inconclusive.
Leclaire et al. (2021) reported cases where secondary choroidal neovascularization not detected by FAG or SD-OCT was identified only by OCT-A, suggesting that there may be a large number of clinically asymptomatic secondary choroidal neovascularizations 5).
Stattin et al. (2021) reported using SS-OCTA to monitor changes in vascular density of choroidal neovascularization secondary to punctate inner choroidopathy, and used this as a guide for anti-VEGF treatment decisions 4).
Active punctate inner choroidopathy lesions appear as hypoautofluorescence 1). A halo of hyperautofluorescence surrounding active lesions may be an indirect sign of uncontrolled inflammation. Atrophic scar lesions are also seen as hypoautofluorescent spots 1).
Fundus autofluorescence is a non-invasive and rapid test, useful for assessing lesion distribution, monitoring treatment response, and detecting recurrence 1).
Subretinal fibrosis and uveitis syndrome: Accompanied by progressive subretinal fibrosis 8).
Ocular toxoplasmosis / ocular tuberculosis: Must be excluded as infectious diseases 8).
Fuchs spot in high myopia: Differentiated as a degenerative disease 8).
QWhat is the difference between punctate inner choroidopathy and multiple evanescent white dot syndrome?
A
Multiple evanescent white dot syndrome is almost always unilateral and resolves spontaneously within a few weeks, leaving almost no scars or choroidal neovascularization6). Punctate inner choroidopathy is often bilateral, leaves atrophic scars, and is frequently complicated by choroidal neovascularization. The presence or absence of blood flow findings on OCTA also helps in differentiation.
If there is no evidence of choroidal neovascularization, the visual prognosis is good and treatment is unnecessary in most cases. The only exception is when there is an active inflammatory lesion very close to the fixation point, in which case medical treatment may be considered.
For active lesions near the fovea, posterior sub-Tenon injection of triamcinolone acetonide or oral steroids (prednisolone 40–60 mg/day with gradual tapering) are used 8). If extrafoveal choroidal neovascularization does not respond to steroids, photocoagulation may be attempted.
Treatment for Cases Complicated by Choroidal Neovascularization
This is the main treatment for punctate inner choroidopathy complicated by choroidal neovascularization. Bevacizumab, ranibizumab, and aflibercept are used.
Stattin et al. (2021) achieved a final visual acuity of 20/20 with a total of 6 injections of ranibizumab (0.5 mg) administered pro re nata under SS-OCTA monitoring for choroidal neovascularization secondary to punctate inner choroidopathy 4).
A bidirectional approach with anti-VEGF agents and steroids is considered effective 4). For cases with CNV, intravitreal bevacizumab injection is sometimes used as first-line therapy 8).
Systemic steroids are usually started at 1 mg/kg/day (60–80 mg/day) for 3–5 days, then tapered 4). Oral steroid use has been reported to reduce the risk of iCNVM by half 3).
Intravitreal steroid preparations include the following:
Fluocinolone acetonide implant (0.59 mg): Sustained release for 36 months. Useful in patients intolerant to systemic therapy or women planning pregnancy.
The efficacy of PDT has been reported in cases with choroidal neovascularization. Combined with oral prednisolone (1 mg/kg/day), a mean of 2 PDT sessions resulted in a 15-letter visual acuity improvement.
QHow many anti-VEGF injections are needed for choroidal neovascularization in punctate inner choroidopathy?
A
It varies by case. Six injections have been reported with pro re nata dosing guided by SS-OCTA4). Regular imaging is used to assess choroidal neovascularization activity, and additional doses may be needed upon recurrence.
The pathophysiology of punctate inner choroidopathy is not fully understood. A leading hypothesis is that it is an inflammatory disease originating in the inner choroid.
Pathological studies of CNVM secondary to punctate inner choroidopathy have shown that the choriocapillaris is preserved, while lymphocytic infiltration is present at the inner choroidal level. This finding ultrastructurally supports the hypothesis that punctate inner choroidopathy is an inflammatory disease originating in the choroid.
On ICG, hypofluorescent areas correspond to focal choroidal hypoperfusion, and focal hyperfluorescent spots on vessel walls may suggest vasculitis. Since large choroidal vessels cross these hypofluorescent areas, the vasculitic process is thought to be confined to small vessels and the choriocapillaris.
Choroidal neovascularization associated with punctate inner choroidopathy is type 2 (subretinal pigment epithelium) and develops through damage to Bruch’s membrane and the retinal pigment epithelium. Neovascular units with few pericytes have been shown to be highly sensitive to anti-VEGF drugs, suggesting that pericytes may be an important therapeutic target.
On OCT-A, active inflammatory chorioretinal lesions show undetectable blood flow signals at the choriocapillaris level 7). Whether primary involvement of the choriocapillaris precedes outer retinal changes or vice versa remains debated 7).
Patients with white dot syndromes and their families have a higher prevalence of systemic autoimmune diseases 6). Patients with punctate inner choroidopathy have been reported to carry IL-10 haplotypes and HLA-DRB1*15 alleles, suggesting that genetic predisposition combined with environmental factors leads to disease onset 6).
Jampol and Becker (2003) proposed integrating MEWDS, MCP, PIC, and AZOOR into a single clinical concept called the “AZOOR complex.” The hypothesis is that genetic predisposition combined with various environmental triggers results in different clinical phenotypes 6).
Liu et al. (2024) reported a 91-month follow-up case of solitary punctate chorioretinitis (SPC), a subtype of punctate inner choroidopathy. SPC is a subtype in which a single lesion appears near the fovea, and the secondary incidence of choroidal neovascularization is lower than that of punctate inner choroidopathy (16% vs. approximately 50%). During the 91-month course, the lesion remained solitary, and the vascular-like structure on OCTA spontaneously regressed. Final visual acuity recovered to 0.8, and anti-VEGF therapy was not required 2).
Stattin et al. (2021) demonstrated that en face images from SS-OCTA can track changes in the vascular structure of choroidal neovascularization (branching, loops, anastomoses) over time, and that SS-OCTA can detect changes in neovascularization even in the absence of indirect activity findings on SD-OCT4). Assessment of choroidal neovascularization activity and treatment decisions based on OCTA findings may become a standard approach for managing punctate inner choroidopathy in the future.
Vaccine-Associated Recurrence and Prophylactic Immunosuppression
In the report by Scott et al. (2024), no recurrence of punctate inner choroidopathy was observed during COVID-19 vaccination under immunosuppression 3). The role of prophylactic immunosuppression during vaccination in high-risk patients is a topic for future investigation.
Coexistence of Punctate Inner Choroidopathy and Multiple Evanescent White Dot Syndrome
Walters et al. (2021) reported a rare case of acute-onset multiple evanescent white dot syndrome occurring in a patient with long-standing punctate inner choroidopathy. The coexistence of punctate inner choroidopathy and multiple evanescent white dot syndrome supports the concept of the AZOOR complex and suggests a common genetic basis 6).
Olazaran L, Jiménez A, González de Los Mártires P, Guerrero G, Gangoitia N, Salmeron I, Galarza A, Argüelles AS, Elso B, Reyzabal I, Compains E, Heras H, López S.. White Dot Syndromes: Report of Three Cases. Case Rep Ophthalmol. 2024;15(1):202-211. doi:10.1159/000536336. PMID:38487796; PMCID:PMC10939511.
Liu C, Liu M, Lan X, Zhu J, Zhang Z.. 91-month follow-up of solitary punctate chorioretinitis in a Chinese patient. BMC Ophthalmol. 2024;24(1):297. doi:10.1186/s12886-024-03576-6. PMID:39030539; PMCID:PMC11264762.
Daniel Andrew Richard Scott, Rachael Louise Niederer. Punctate Inner Choroidopathy (PIC) disease recurrence with inflammatory choroidal neovascular membrane (iCNVM) post-COVID-19 vaccine. European Journal of Ophthalmology. 2024;34(5):NP78-NP82. doi:10.1177/11206721241257969.
Stattin M, Forster J, Ahmed D, Krepler K, Ansari-Shahrezaei S. Swept Source-Optical Coherence Tomography Angiography for Management of Secondary Choroidal Neovascularization in Punctate Inner Choroidopathy. Case reports in ophthalmology. 2021;12(1):232-238. doi:10.1159/000511669. PMID:33976688; PMCID:PMC8077444.
Leclaire MD, Clemens CR, Eter N, Mihailovic N. Choroidale Neovaskularisation infolge einer “punctate inner choroidopathy”, dargestellt mittels optischer Kohärenztomographie-Angiographie. Ophthalmologe. 2021;118:842-846. doi:10.1007/s00347-020-01200-8.
Walters AR, Choi RY, Flaxel CJ.. Multiple Evanescent White Dot Syndrome Presenting in a Patient With Punctate Inner Choroidopathy. J Vitreoretin Dis. 2021;5(3):270-274. doi:10.1177/2474126420965031. PMID:37006511; PMCID:PMC9979046.
Testi I, Modugno RL, Pavesio C. Multimodal imaging supporting the pathophysiology of white dot syndromes. Journal of ophthalmic inflammation and infection. 2021;11(1):32. doi:10.1186/s12348-021-00261-3. PMID:34529201; PMCID:PMC8446150.