Ocular toxoplasmosis is a retinochoroiditis caused by infection of the retina with Toxoplasma gondii, an obligate intracellular protozoan parasite. It is the most common cause of infectious uveitis and accounts for over 50% of all posterior uveitis cases in some countries7).
T. gondii is a zoonotic infection for which felids are the definitive host and almost all mammals, including humans, serve as intermediate hosts. Infection occurs through oral ingestion of soil or water contaminated with oocysts excreted in cat feces, or by consuming tissue cysts in undercooked meat (such as pork, lamb, or venison). Approximately one-third of the world’s population is infected7), and the seroprevalence among Japanese adults is 20–30%. Ocular toxoplasmosis accounts for about 1% of infectious uveitis cases8).
The protozoan has the following three forms.
Oocyst: A soil form excreted in cat feces
Tachyzoite: Rapidly multiplying form during active infection
Tissue cyst: A slow-growing form (bradyzoite) that remains dormant within the retina
The proportion of eye diseases caused by ocular toxoplasmosis is estimated to be about 2% in the United States, 18% in Brazil, and up to 43% in Africa. Infection rates are highest in tropical regions, reflecting the warm, humid environment favorable for the proliferation of the protozoan.
The population structure of T. gondii is highly clonal, with three main lineages—type I, type II, and type III—predominating in North America and Europe 7). Type II accounts for the majority of acquired ocular lesions, while type I is more common in congenital toxoplasmosis. In Brazil, type I and atypical types are involved in acquired infections, and differences in genotype may contribute to the diversity of clinical presentations 7).
QWhat is the difference between congenital infection and acquired infection?
A
Congenital infection occurs when the mother’s primary infection is transmitted to the fetus through the placenta during pregnancy, typically resulting in scarred lesions in the macula of both eyes. The rate of placental infection increases during the second and third trimesters, but the severity of the disease tends to be higher with infection early in pregnancy. Acquired infection occurs after birth through ingestion of contaminated food or water, presenting as localized retinochoroiditis without pre-existing old scars in the peripheral fundus. For details, refer to the “Pathophysiology” section.
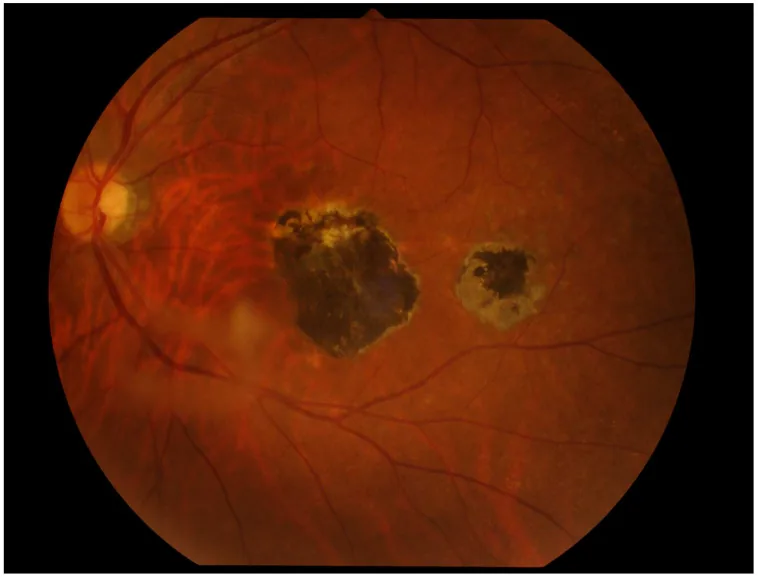
Miyagaki M, et al. Ocular Toxoplasmosis: Advances in Toxoplasma gondii Biology, Clinical Manifestations, Diagnostics, and Therapy. Pathogens. 2024. Figure 2. PMCID: PMC11509995. License: CC BY.
At the posterior pole of the fundus, there is a chorioretinal scar lesion with pigmentation, and nearby small satellite lesions are observed. This shows a typical chorioretinal lesion seen in ocular toxoplasmosis and is suitable for explaining clinical findings.
Anterior uveitis: Secondary non-granulomatous iridocyclitis. Granulomatous stellate keratic precipitates may also be observed.
Atypical Findings
Papillitis/Optic neuritis with retinitis: Swelling of the optic disc. May be accompanied by a macular star.
Punctate outer retinitis (PORT): Multiple small lesions in the deep retina. OCT may reveal huge outer retinal cysts (HORC) 2). HORC are located between the ELM (external limiting membrane) and the inner boundary of the RPE; in one reported case, the highest point of the cyst reached 475 μm 2). During the active phase, loss of the external limiting membrane (ELM) and elongation/splitting of the IS/OS junction are observed, but these recover after treatment response 2).
Retinal vascular occlusion: May cause branch artery occlusion or frosted branch angiitis.
Multifocal diffuse necrotizing retinitis: In immunocompromised patients, it may present with severe bilateral lesions7).
In congenital infection, the main lesions are scarred foci in both maculae (consisting of gray-white fibrous proliferative tissue and dark brown pigmentation in the center, surrounded by a depigmented ring). Small pigmented scars called daughter lesions may be seen nearby. It is accompanied by anterior chamber inflammation and severe vitreous opacity (“headlights in fog”), and unlike acquired infection, it is bilateral. Recurrent lesions do not occur simultaneously in both eyes. In acquired infection, localized white to gray-white exudative chorioretinitis is seen in the peripheral fundus without old scars, accompanied by severe vitreous opacity and retinal vasculitis. With healing, it becomes a well-defined atrophic scar with pigmentation.
Lesions around the optic disc are called Edmund-Jensen type juxtapapillary retinochoroiditis. In fluorescein fundus angiography, early phase shows tissue staining around the lesion and a central filling defect, with progressive fluorescence staining of the defect over time, and marked leakage in the late phase.
In atypical cases, differentiation from acute retinal necrosis (ARN) and intraocular lymphoma can be difficult5). In a Dutch cohort, 4 out of 18 large lesions exceeding 3 disc diameters were initially diagnosed as acute retinal necrosis5).
The main routes of T. gondii infection are the following three.
Oral infection: Ingestion of tissue cysts in undercooked meat (pork, lamb, venison, etc.). Oocysts may also be ingested orally from contaminated water or vegetables.
Infection from felines: Contact with oocysts excreted in cat feces
Transplacental infection: Transmission to the fetus occurs during the mother’s primary infection in pregnancy. The infection rate is low in early pregnancy, but the disease severity is high; the placental infection rate increases as pregnancy progresses to the middle and late stages.
The main risk factors are as follows.
Consumption of undercooked meat: Game meat (venison) poses a particularly high risk. In one case series, systemic symptoms appeared within 1–2 weeks after consuming undercooked venison, and ocular symptoms appeared after an average of 2.6 months4)
Contact with cats: Keeping three or more cats or kittens
Immunocompromised state: AIDS, hematologic malignancies, use of immunosuppressive drugs. In CLL patients, it has been reported as an opportunistic infection during ibrutinib use3). In CLL patients with hypogammaglobulinemia, serum IgG antibodies are not produced, which may lead to false-negative results, so caution is required3)
Elderly individuals: Ocular lesions due to acquired infection tend to occur more frequently7)
Kohler et al. (2023) reported four cases of primary infection associated with venison consumption. All cases were male, with an average age of 56 years, and exposure occurred during the hunting season from October to November. They showed a clear temporal sequence: systemic symptoms appeared within a few weeks, and ocular symptoms appeared 1 to 3 months later 4).
QIf infected during pregnancy, will it always affect the fetus?
A
Even if a primary infection occurs in the mother, it does not always lead to infection in the fetus; most cases remain asymptomatic. However, some cases develop into congenital toxoplasmosis, presenting severe ocular and neurological symptoms (the tetrad of retinochoroiditis, hydrocephalus, intracranial calcifications, and motor nerve disorders), making antibody screening and early treatment in pregnant women important.
The diagnosis of ocular toxoplasmosis is primarily based on clinical findings. The combination of a “headlight in the fog” appearance and retinochoroidal scars with pigmentation is typical, and clinical diagnosis is often possible. The presence of both clinical findings and positive anti-Toxoplasma antibodies strongly supports the diagnosis 8).
Negative result can rule out. Positive rate increases with age.
IgM antibody
Suggests recent infection
May remain elevated for over a year in some cases. Does not rise during recurrence of congenital infection
IgG avidity
Estimates whether infection is recent or past
High avidity suggests chronic infection5)
In immunocompetent individuals, if IgG antibodies are completely negative, toxoplasmosis can be almost ruled out. However, in immunocompromised patients, active infection is possible even if antibodies are negative 3). In CLL patients with hypogammaglobulinemia, caution is needed for false negatives 3).
In cases of acquired infection, a rise in serum IgM antibody titer is observed, and if it later decreases, it has diagnostic value. A rise in IgG antibody titer is also seen, but since subclinical infections are common, a high antibody titer does not necessarily indicate toxoplasmic chorioretinitis. During recurrence of congenital infection, no rise in IgM antibody titer is observed.
Intraocular fluid testing (PCR and Goldmann-Witmer coefficient)
PCR testing of aqueous humor or vitreous fluid is useful in atypical or diagnostically challenging cases.
Sensitivity: approximately 64% for aqueous humor PCR1), and 27–75% for vitreous PCR5)
Specificity: 100%5)
In immunocompromised patients, sensitivity increases to 75%3)
A method that calculates the ratio of Toxoplasma antibody titer to IgG level in intraocular fluid (Goldmann-Witmer coefficient: Q value) is also useful, with reported sensitivity of 29–81% and specificity of 83–100%5). When combined with immunoblotting, the three methods together achieve a sensitivity of 85–97% and specificity of 93%5).
Shakha et al. (2024) reported a 33-year-old man with atypical multifocal retinitis in whom T. gondii was detected by aqueous humor PCR, leading to a definitive diagnosis. The case worsened after sub-Tenon injection of steroids, highlighting the risk of depot steroid administration before a definitive diagnosis1).
The Standardized Uveitis Nomenclature (SUN) Working Group published classification criteria for toxoplasmic retinitis in 2021 9). In addition to focal or few necrotizing retinitis, the criteria require a positive PCR or IgM, or characteristic clinical findings (pigmented scars, round to oval retinitis, recurrent acute course). This criterion, which integrates not only clinical findings but also laboratory findings, is useful for case identification in multicenter studies and clinical trials.
Differential diagnoses requiring special attention: CMV retinitis in immunocompromised patients, acute retinal necrosis, intraocular lymphoma3)5)
In the differential diagnosis from intraocular lymphoma, flow cytometry, cytology, and MYD88 mutation analysis of vitreous fluid are useful 3). If flow cytometry shows T-cell predominance and no abnormal B cells, lymphoma is unlikely. PCR using ITS-specific primers is highly sensitive (reported to detect copy numbers of 5 million or more) and contributes to the definitive diagnosis of toxoplasmosis in immunocompromised patients 3). Prior steroid exposure reduces biopsy sensitivity, so depot steroids are strictly contraindicated before definitive diagnosis 3)5).
In the differential diagnosis from acute retinal necrosis, large multifocal lesions exceeding 3 disc diameters can be confused with intraocular lymphoma or acute retinal necrosis5). Intraocular lymphoma often presents as yellowish-white lesions beneath the retina or retinal pigment epithelium, and tends to have milder anterior inflammation than toxoplasmosis. Differential use of three tests (PCR, Goldmann-Witmer coefficient, and immunoblot): PCR has high sensitivity in early disease and immunocompromised patients, while Goldmann-Witmer coefficient and immunoblot are particularly useful in later stages and immunocompetent patients 5).
QIf the blood test is positive, does it always mean ocular toxoplasmosis?
A
A positive IgG antibody test only indicates past infection and does not necessarily mean that ocular lesions are present. Since subclinical infections are common, a comprehensive assessment with clinical findings is essential for the diagnosis of ocular toxoplasmosis. The Uveitis Clinical Practice Guidelines also strongly support the diagnosis when both clinical findings and antibody positivity are present 8).
Not all lesions require treatment. Mild inflammation confined to the peripheral retina tends to heal spontaneously. Treatment is indicated in the following cases.
Lesions threatening the macula, lesions of the optic disc and papillomacular bundle
Lesions adjacent to major retinal vessels
Severe vitreous opacity
Significant visual impairment, large lesion (≥1/2 disc diameter)
Administer acetylspiramycin (0.8–1.2 g/day, divided into 3–4 doses) for at least 30 days. Treatment may be continued for 2–3 months until active inflammation resolves. Discontinue treatment when exudative lesions have scarred and the toxoplasma antibody titer has decreased.
If vitreous inflammation is severe, oral steroids (starting with prednisone 20–30 mg/day) are used in combination, but it is preferable to wait a few days after starting antibiotics before adding them 8). Combining oral steroids at 0.5 mg/kg/day accelerates improvement in ocular findings. For posterior pole lesions or recurrent foci larger than half the optic disc diameter, combination therapy with anti-Toxoplasma drugs and steroids is necessary.
Another option is to use clindamycin 1.2 g divided into four doses orally, with one course lasting 4 to 6 weeks.
The classic treatment is a triple therapy of pyrimethamine, sulfadiazine, and steroids, and 32% of respondents in a survey by the American Uveitis Society chose it as first-line therapy. Since pyrimethamine is a folate antagonist, folinate (leucovorin) is used concomitantly to prevent bone marrow suppression. It is usually administered for 4 to 6 weeks.
TMP-SMX (160/800 mg) twice daily is a safe and effective alternative to pyrimethamine plus sulfadiazine 7). It has fewer side effects and is more readily available.
Kohler et al. (2023) treated all four cases of primary infection with TMP-SMZ alone and achieved rapid improvement of retinal lesions. However, continuous administration for at least three months was necessary to prevent recurrence of systemic symptoms4).
Intravitreal injection of clindamycin 1 mg plus dexamethasone 0.4 mg shows efficacy comparable to systemic administration, with a recurrence rate of 6–15% after 2 years 5). It is indicated for patients in whom systemic therapy is contraindicated 7). There are almost no side effects, and according to Fernandez Zamora (2015) cited by Dillon et al., the time to resolution was approximately 2.5 ± 1 weeks 5).
Azithromycin 500 mg initially, followed by 250 mg/day, shows efficacy equivalent to TMP-SMX5). When combined with pyrimethamine, it can replace sulfadiazine, with a lower frequency of side effects7).
Syed Mohd Khomsah et al. (2023) administered azithromycin 500 mg/day and a tapering dose of prednisolone for 6 weeks to a 35-year-old woman with bilateral ocular toxoplasmosis. Vitreitis and optic disc swelling resolved in 4 weeks, but right eye visual acuity was poor due to fibrosis of the papillomacular bundle and macular pucker6).
Atovaquone 750 mg four times daily is used in cases of intolerance to first-line drugs 5). Response is obtained within 1 to 3 weeks of starting treatment, and serious side effects are considered rare.
A prospective randomized trial reported that long-term administration of TMP-SMX (160/800 mg) three times per week reduced the recurrence rate from 23.8% to 6.6%7). In another randomized trial, one tablet every other day for 311 days resulted in a recurrence rate of 1.4% at 6 years (vs. 27.5% in the placebo group)5).
Complications of ocular toxoplasmosis may include epiretinal membrane (ERM) and neovascularization4). In ERM cases, vitrectomy and membrane peeling can be expected to improve visual acuity. There are reports that neovascularization may spontaneously regress in response to anti-toxoplasma treatment, but vitreoretinal traction may persist after treatment 4).
Macular pucker is a serious complication of ocular toxoplasmosis that threatens vision. It causes fibrosis and tractional changes in the inner retina, and poor visual acuity may persist even after treatment 6). Vitrectomy (PPV) and membrane peeling are indicated for ERM, macular hole, and retinal detachment, but when extensive fibrosis is present, visual improvement is unlikely, so preoperative OCT evaluation is important 6).
QDo all recurrences need to be treated?
A
Small lesions confined to the peripheral retina may heal spontaneously. However, because the number of intraretinal cysts increases with each recurrence, some believe that all recurrences should be treated with antibiotics to minimize the risk of future recurrence. Treatment is necessary when posterior pole lesions or decreased visual acuity are present.
T. gondii primarily infects the retina and can also spread to the choroid, vitreous body, and anterior chamber7). Choroidal lesions occur secondary to retinal infection and do not appear alone.
Ingested oocysts or tissue cysts transform into tachyzoites in the intestine and are disseminated throughout the body via the bloodstream. Proposed routes for reaching the retina include transport by leukocytes carrying the parasite and direct passage of tachyzoites through vascular endothelium6).
Proliferation and immune response within the retina
Tachyzoites infect various cells in the retina, but the most susceptible host cells are Müller glial cells6). Infection of the retinal pigment epithelium (RPE) leads to abnormal growth factor production, promoting proliferation of adjacent uninfected RPE cells. This mechanism is thought to be involved in the formation of characteristic pigmented scars.
In necrotizing retinitis, vasculitis and retinal destruction progress. Histologically, extensive granulomatous inflammatory infiltration with necrosis of Bruch’s membrane is observed7). Scarring progresses from the periphery toward the center, and the degree of pigmentation varies among cases.
Even if transplacental infection occurs, the onset of disease is rare, and most cases remain asymptomatic. The main symptoms of congenital toxoplasmosis are the four signs: retinochoroiditis, hydrocephalus (or microcephaly), intracranial calcification, and psychomotor impairment. Approximately 70% of infants infected in utero have chorioretinal scars (centered on the macula), and 1–2% of these develop severe visual impairment. Recurrence tends to occur mainly during adolescence, and about one-third of scarred lesions recur.
In an evaluation of 430 cases treated for congenital toxoplasmosis, ocular lesions were observed in 30% of cases after a median follow-up of 12 years 7). However, severe binocular visual impairment occurred in only 2 of 130 cases, and overall functional prognosis was better than predicted in the literature 7).
The cause of recurrence is not fully understood, but it is thought to involve the rupture of dormant cysts within the retina7) or the involvement of Toxoplasma circulating in peripheral blood. Drug-resistant cysts may persist in atrophic scarred lesions even after treatment, and recurrence can be triggered by decreased immunity or pregnancy. The risk of recurrence is highest within one year after the initial episode. The recurrence rate for congenital infection is reported to be approximately 5–30%.
Pidro Miokovic et al. (2024) reported a case of ocular toxoplasmosis in a 16-year-old female, in which a huge outer retinal cystoid change (HORC) was observed in the outer retina2). HORC is a rare finding seen in only 2.5% of all ocular toxoplasmosis cases and is located between the external limiting membrane and the inner boundary of the RPE. During the active phase, elongation and splitting of the IS/OS junction and internal hyperreflective foci are observed, and the ELM cannot be identified near the HORC but can be identified in the surrounding retina2). Seven days after treatment, the HORC decreased in size and completely resolved within two weeks. Visual acuity improved from 0.5 to 1.0 and remained stable for six months. In this case, after treatment, deep hyperreflective material accumulation and spherical structures were observed within the area of RPE atrophy 2).
In atypical ocular toxoplasmosis, OCT of active retinitis shows increased reflectivity of the retinal layers with posterior shadowing, and partial posterior vitreous detachment with vitreous cells is observed 1). In large lesions exceeding 2–3 disc diameters, visual prognosis depends not only on the site of retinitis but also on the degree of vitreous opacity.
In immunocompromised patients, atypical clinical presentations are common, leading to delayed diagnosis. Since conventional serological tests can yield false-negative results, the role of PCR testing becomes even more important. PCR sensitivity increases to 75% in immunocompromised patients, whereas it remains at 30–40% in immunocompetent individuals3).
Yazdanpanah et al. (2021) reported a case of ocular toxoplasmosis in a 74-year-old woman with CLL that was difficult to differentiate from intraocular lymphoma 3). Flow cytometry and cytology of vitreous fluid ruled out lymphoma, and PCR with ITS-specific primers detected over 5 million copies of T. gondii DNA. There have also been reports of Toxoplasma DNA detected in intraocular lymphoma cells, suggesting a possible association between the two 3). In this case, the onset occurred 2 months after starting ibrutinib, highlighting the need to consider ocular toxoplasmosis as an opportunistic infection during CLL treatment. Due to TMP-SMX allergy, the patient was treated with pyrimethamine + leucovorin + prednisone combined with intravitreal clindamycin injection, achieving stable vision after 4 weeks 3).
Dillon et al. (2022) reported two cases presenting with extensive multifocal retinal lesions 5). Case 1 (69-year-old woman) was hospitalized with a clinical diagnosis of acute retinal necrosis and was initially treated with intravenous and intravitreal foscarnet, but was confirmed as ocular toxoplasmosis due to positive Toxoplasma IgG and IgM and positive vitreous PCR. Case 2 (75-year-old woman) underwent PPV and chorioretinal biopsy for differentiation from intraocular lymphoma, and numerous tachyzoites were identified on immunohistochemistry, with positive vitreous PCR confirming the diagnosis 5). Both cases had multifocal lesions exceeding 3 disc diameters, markedly different from the typical solitary 1–2 disc diameter lesion. On FA, the lesions showed occlusive vasculitis, ischemia, and late leakage 5). In refractory cases, multiple intravitreal injections were required after recurrence 5).
Epidemiology of Venison Consumption and Primary Infection
In Minnesota, USA, the seroprevalence of T. gondii in white-tailed deer reaches 22.5–32.2%, with even higher rates in neighboring states4). A pattern has been reported where ocular symptoms appear in winter after consuming undercooked venison during the hunting season (autumn)4). For safe preparation of venison, heating to an internal temperature of at least 64°C is recommended. Since tissue cysts remain infectious even after refrigeration (3 weeks) or freezing (over 11 days), cold storage alone is insufficient4).
Acquired ocular toxoplasmosis from primary infection often presents as a solitary retinochoroiditis without adjacent pigmented scars, and the above epidemiological history is an important clue for differentiation from reactivation 4). OCT findings show full-thickness retinal irregularity and thickening with posterior shadowing, which markedly improve after treatment response at one month 4). In primary infection cases, both IgG and IgM are positive in all cases, which is useful for differentiation from IgM-negative cases (congenital infection reactivation) 4).
Shakha, Chawla R, Sinha A, Meena S.. Atypical acquired toxoplasmosis. Indian J Ophthalmol. 2024;72(6):772-774. doi:10.4103/ijo.ijo_3341_23. PMID:38804796; PMCID:PMC11232862.
Pidro Miokovic A, Ratkovic M, Pidro Gadzo A. Toxoplasmosis in the outer retina. Rom J Ophthalmol. 2024;68(2):198-201. doi:10.22336/rjo.2024.37.
Yazdanpanah O, Monday LM, Surapaneni S, Singh V, Chi J.. Ocular Toxoplasmosis Mimicking Lymphoma: Exploring the Correlation and Distinction. Cureus. 2021;13(1):e13014. doi:10.7759/cureus.13014. PMID:33659144; PMCID:PMC7920518.
Kohler JM, Mammo DA, Bennett SR, Davies JB.. Primary ocular toxoplasmosis secondary to venison consumption. Am J Ophthalmol Case Rep. 2023;29:101776. doi:10.1016/j.ajoc.2022.101776. PMID:36544752; PMCID:PMC9762148.
Dillon AB, Budoff G, McCannel CA, Tsui E, Pullarkat ST, Schwartz SD.. Ocular Toxoplasmosis: No Stranger to the Masquerade Ball. J Vitreoretin Dis. 2022;6(5):391-398. doi:10.1177/24741264211056769. PMID:37006900; PMCID:PMC9954925.
Syed Mohd Khomsah SNH, Muhammed J, Wan Hitam WH.. Macular Pucker: A Devastating Complication in Ocular Toxoplasmosis. Cureus. 2023;15(2):e34617. doi:10.7759/cureus.34617. PMID:36891009; PMCID:PMC9986773.
Commodaro AG, Belfort RN, Rizzo LV, Muccioli C, Silveira C, Burnier MN, Belfort R.. Ocular toxoplasmosis: an update and review of the literature. Mem Inst Oswaldo Cruz. 2009;104(2):345-350. doi:10.1590/s0074-02762009000200030. PMID:19430662.
Jabs DA, Belfort R Jr, Bodaghi B, et al. Classification Criteria for Toxoplasmic Retinitis. Am J Ophthalmol. 2021;228:134-141. doi:10.1016/j.ajo.2021.03.042.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.