Bacterial endophthalmitis is an intraocular inflammatory disease caused by bacterial invasion into the eye. It is classified into exogenous and endogenous types based on the route of infection. Exogenous endophthalmitis occurs after ophthalmic surgery, intravitreal injection, or penetrating ocular trauma, with gram-positive bacteria (e.g., coagulase-negative staphylococci, enterococci) as the main causative agents. In contrast, endogenous bacterial endophthalmitis develops when bacteria from an infectious focus in another organ spread hematogenously to the retina and choroid. It often occurs secondary to sepsis (bacteremia), and gram-negative rods are the predominant causative organisms.
In general, bacterial endophthalmitis progresses more rapidly than fungal endophthalmitis, and endogenous cases caused by gram-negative rods progress particularly fast and have a poor prognosis. The Uveitis Clinical Practice Guidelines classify it as a type of infectious endophthalmitis, organized by both causative microorganism (bacterial vs. fungal) and route of infection (exogenous vs. endogenous)1).
Endogenous bacterial endophthalmitis does not occur in healthy individuals. Patients always have some underlying disease or risk factor, and it develops in immunocompromised hosts such as the elderly, those with diabetes, organ abscess (lung, liver, kidney), or those undergoing immunosuppressive therapy.
Among these, liver abscess is particularly important as the underlying disease with the highest risk of developing endophthalmitis. In the past, the main causative organism of liver abscess was Escherichia coli, but since the 1990s, Klebsiella pneumoniae has accounted for over 80% of liver abscess cases in Southeast Asia, Europe and the United States, and Japan. Liver abscess caused by Klebsiella pneumoniae is associated with endophthalmitis in 3–8% of cases, and special attention is needed for endogenous endophthalmitis caused by this bacterium. In addition, over 80% of cases are unilateral.
A systematic review of 342 cases showed that the distribution of causative organisms of endogenous bacterial endophthalmitis differs between Asia and Western countries, with Gram-negative rods (especially Klebsiella pneumoniae) predominating in Asia2).
Main underlying diseases/risk factors
Notes
Liver abscess (most common)
Klebsiella pneumoniae accounts for over 80%; endophthalmitis incidence 3–8%
Urinary tract infection
Via bacteremia caused by Gram-negative rods
Lung abscess
Direct hematogenous dissemination from abscess
Infective endocarditis
Gram-positive bacterial endophthalmitis caused by Staphylococcus aureus etc.
Meningitis
Secondary to severe systemic infection
Malignancy
Background of impaired immune function/chemotherapy
Diabetes mellitus
Neutrophil dysfunction due to hyperglycemia
Steroid/immunosuppressive therapy
General decrease in host defense function
Collagen disease
Increased susceptibility due to the disease itself and therapeutic drugs
QHow do endogenous and exogenous endophthalmitis differ?
A
The main differences are the route of infection and causative organisms. Exogenous endophthalmitis occurs after direct invasion into the eye, such as surgery, trauma, or intravitreal injection, and is mainly caused by Gram-positive bacteria (coagulase-negative staphylococci, enterococci, etc.). In contrast, endogenous endophthalmitis develops when bacteria from other organ infections, such as liver abscess or urinary tract infection, reach the retinochoroid via the bloodstream, and is mainly caused by Gram-negative rods (e.g., Klebsiella pneumoniae). Exogenous cases have a clear history of surgery or trauma, while endogenous cases are characterized by preceding systemic infection symptoms such as fever.
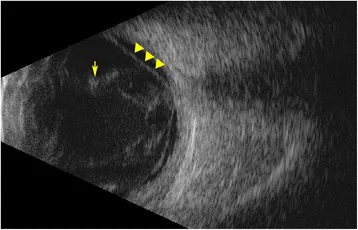
Sadiq MA, et al. Endogenous endophthalmitis: diagnosis, management, and prognosis. J Ophthalmic Inflamm Infect. 2015. Figure 3. PMCID: PMC4630262. License: CC BY.
B-mode ultrasound of the eyeball shows diffuse high-echo opacities in the vitreous cavity, indicating severe vitreous inflammation and exudation. Membranous high-echo lines are also observed, suggesting retinal detachment seen in severe cases.
In endogenous endophthalmitis, systemic signs of infection are observed preceding or concurrent with ocular symptoms. Elevation of procalcitonin (PCT), a serum marker of severe bacterial infection, increased white blood cell count, and high CRP levels are noted. If the patient has diabetes as an underlying disease, hyperglycemia and high HbA1c levels are observed. When the general condition is extremely poor, the patient may not recognize or report ocular symptoms.
Fever and general malaise (always present as signs of infection)
Elevated PCT (serum marker of severe bacterial infection)
Increased white blood cell count and elevated CRP (acute inflammatory markers)
Hyperglycemia and elevated HbA1c (observed in patients with diabetes)
Early subjective symptoms include floaters, blurred vision, and decreased visual acuity. In the acute phase, in addition to vision loss and photophobia, eye pain is perceived. Visual acuity deteriorates rapidly and may drop to hand motion or light perception levels.
Acute phase: from onset to several hours to days
Eyelid redness and swelling: In advanced cases, it becomes difficult to open the eye on one’s own.
Marked conjunctival and ciliary injection: In severe inflammation, conjunctival edema and subconjunctival hemorrhage may also be observed.
Anterior chamber inflammation: Characterized by prominent inflammatory cells, fibrin exudation, hypopyon, and hyphema.
Vitreous opacity: Dense opacity makes the fundus completely invisible (confirmed by ultrasound).
Progressive phase: inflammation spreads to the entire eyeball
Vitreous abscess formation: When formed, it often leads to panophthalmitis and has a very poor prognosis.
Retinal and optic nerve damage: Retinal vascular occlusion, retinal necrosis, and optic atrophy cause irreversible vision loss1).
Spread to periorbital tissues: Inflammation may extend to the orbital tissues, causing proptosis and restricted eye movement.
Need for emergency surgery: Cases that progress to panophthalmitis require urgent surgical intervention.
QWhat are the clues to suspect endophthalmitis when there is eye pain and fever?
A
When systemic infection symptoms (fever, malaise) and ocular symptoms (eye pain, redness, rapid vision loss) occur simultaneously, strongly suspect endogenous endophthalmitis. Especially in patients with risk factors such as diabetes, liver abscess, malignancy, or immunosuppressive therapy, if fever is accompanied by ocular symptoms, urgent ophthalmologic consultation is necessary. The presence of hypopyon, vitreous opacity, and eyelid swelling together indicates a very high likelihood of endophthalmitis. The principle is to start treatment without waiting for test results 1).
The main causative organism of endogenous bacterial endophthalmitis is gram-negative bacilli.
Klebsiella pneumoniae: Most important in endogenous endophthalmitis secondary to liver abscess. Its incidence has markedly increased since the 1990s in Asia (including Southeast Asia and Japan), accounting for over 80% of causative organisms in liver abscess. Liver abscess caused by this organism is complicated by endophthalmitis in 3–8% of cases.
Escherichia coli: Previously a major cause of liver abscess and urinary tract infection, and remains important.
Pseudomonas aeruginosa: Causes severe infections in immunocompromised hosts.
Metastatic endophthalmitis due to Staphylococcus aureus has also been reported, occurring secondary to systemic infections with gram-positive organisms such as infective endocarditis 1).
In Asia, the incidence of Klebsiella pneumoniae liver abscess-associated endophthalmitis is known to be higher than in Western countries 3). Clinical practice in East Asia requires management with this organism in mind for endogenous endophthalmitis.
For endogenous endophthalmitis to develop, in addition to a primary infection focus (e.g., liver abscess, urinary tract infection), host immunocompromising factors are almost always present.
Diabetes mellitus: Hyperglycemia impairs neutrophil function and immune response, promoting infection.
Malignancy: Immunosuppression due to the tumor itself, and bone marrow suppression after chemotherapy or radiotherapy.
Collagen disease: Increased susceptibility to infection due to both disease activity and immunosuppressive drugs
Long-term steroid use/immunosuppressive therapy: Decreased T-cell function and neutrophil dysfunction
Advanced age: Decline in overall immune function with aging (especially humoral and cellular immunity)
When endogenous endophthalmitis is suspected, the principle is to prioritize treatment without waiting for test results. Because acute infection can worsen rapidly within hours, once endophthalmitis is suspected based on history and clinical symptoms, intraocular fluid collection and antibiotic administration should be initiated concurrently.
The most important test for definitive diagnosis is smear and culture examination of intraocular fluid (aqueous humor and vitreous humor).
Smear examination (Gram stain, etc.): Useful for early diagnosis. Allows rapid identification of the type of causative organism (Gram-positive or Gram-negative)
Culture examination: Essential for identifying the causative organism and confirming drug sensitivity. Vitreous humor has a higher detection rate of causative organisms than aqueous humor
PCR (genetic testing): Can detect DNA of causative organisms even in culture-negative cases, and its use has been increasing in recent years
Fungal endophthalmitis: Progression is relatively slow (days to weeks) compared to bacterial (hours to days). Positive β-D-glucan and retinal white exudative lesions (fungus ball) are characteristic1)
Delayed (chronic) bacterial endophthalmitis: Caused by Cutibacterium acnes occurring one month or more after cataract surgery. Chronic iridocyclitis and recurrent hypopyon are characteristic1)
QDoes hypopyon always indicate endophthalmitis?
A
Hypopyon is a characteristic finding of endophthalmitis, but it can also occur in acute anterior uveitis (HLA-B27-associated, Behçet’s disease, etc.), extension of infectious keratitis, and diabetic iritis. Key points for differentiation are: ① history of surgery or trauma (differentiation from exogenous endophthalmitis), ② presence of systemic infection symptoms such as fever (differentiation from endogenous endophthalmitis), ③ degree of eyelid swelling and conjunctival chemosis, ④ depth of vitreous opacity and visibility of the fundus, and ⑤ speed of visual acuity decline. In endophthalmitis, systemic symptoms are present, vitreous opacity is severe, and visual acuity declines rapidly. If suspected, treatment should be initiated without waiting for test results1).
When endophthalmitis is suspected, simultaneous administration of antibiotics via three routes should be initiated immediately without waiting for pathogen identification. The three routes are: ① intravitreal injection, ② frequent topical antibiotic eye drops, and ③ systemic administration (intravenous infusion). Collaboration with internal medicine (gastroenterology, infectious disease) to concurrently treat the primary infection focus (e.g., liver abscess) is essential1).
Pharmacotherapy Protocol (When Pathogen is Unknown)
Used in combination for anti-inflammatory purposes
Systemic administration ①
Imipenem/cilastatin (Tienam®) injection
1 g twice daily intravenous drip infusion for 5 days
Broad-spectrum carbapenem
Systemic administration ②
Levofloxacin (Cravit®) tablets 500 mg
1 tablet once daily orally for 5 days
Used in combination with systemic administration ①
For systemic administration, broad-spectrum antibiotics such as the fourth-generation cephalosporin cefozopran (Firstcin®) may also be selected. After drug susceptibility is determined, treatment is continued by switching to a more specific antibiotic. If Gram-negative bacilli (e.g., Klebsiella pneumoniae) are identified, the optimal drug is selected from carbapenems, fluoroquinolones, and third- to fourth-generation cephalosporins according to the susceptibility pattern.
In cases unresponsive to drug therapy, vitrectomy should be performed as soon as possible if the patient’s general condition allows. Vitrectomy physically removes the vitreous body, which serves as a medium for infection, and delivers antibiotics directly into the eye. The Uveitis Clinical Practice Guidelines recommend early vitrectomy with antibiotic perfusion in cases of rapid progression, inability to visualize the fundus due to vitreous opacity, or subretinal abscess 1).
Indications: Cases unresponsive to drug therapy, inability to visualize the fundus, subretinal abscess formation
Surgical technique: Vitrectomy. Combined with lensectomy, intraocular lens/capsule removal as needed
Perfusion fluid: Use perfusion fluid mixed with antibiotics (e.g., vancomycin)
Limitations: A challenge is that surgery often cannot be performed in patients with poor general condition (e.g., during sepsis management)
QDo antibiotics work quickly?
A
While the causative organism is unknown, broad-spectrum antibiotics are administered via three routes simultaneously. Once drug susceptibility is determined, switching to more specific drugs enhances efficacy. However, endophthalmitis caused by Gram-negative bacilli (e.g., Klebsiella pneumoniae) progresses extremely rapidly (within hours), and antibiotic eye drops alone are insufficient for intraocular penetration; therefore, intravitreal injection and systemic administration must be combined. If drug therapy does not improve the inability to visualize the fundus or if progression occurs, promptly consider switching to vitrectomy1).
6. Pathophysiology and Detailed Mechanism of Onset
Endogenous bacterial endophthalmitis develops when bacteria from an infectious focus in another organ (e.g., liver abscess, urinary tract infection) enter the bloodstream and are hematogenously disseminated to the retinochoroidal tissue. Once bacteria colonize the choroidal capillary bed, a local inflammatory reaction rapidly progresses, spreading from retinochoroiditis to vitritis.
It often occurs in immunocompromised hosts with underlying diseases such as malignancy, diabetes, collagen disease, or use of immunosuppressive drugs. In these hosts, bacterial clearance from the blood is reduced, making intraocular infection more likely to establish.
Tissue Damage by Endotoxin of Gram-Negative Bacilli
When the causative organism is a gram-negative bacillus (e.g., Klebsiella pneumoniae, Escherichia coli, Pseudomonas aeruginosa), progression is particularly rapid. The endotoxin (lipopolysaccharide, LPS) of gram-negative bacilli triggers a strong inflammatory response in intraocular tissues and amplifies the inflammatory cascade, which is a major factor in rapid deterioration. Due to this mechanism, the prognosis tends to be worse compared to exogenous endophthalmitis (mainly caused by gram-positive bacteria).
Establishment of bacteremia from the primary infectious focus
Bacterial colonization of choroidal capillaries → formation of choroiditis and retinochoroiditis
Spread of inflammation to the retina and vitreous cavity → rapid vitreous opacification and vitritis
Advanced cases: formation of vitreous abscess → spread to sclera and orbital tissues (panophthalmitis)
Factors contributing to poor visual prognosis include retinal vascular occlusion, retinal necrosis, and optic atrophy1). If treatment is delayed, many cases eventually result in no light perception, and the speed of treatment initiation directly affects the prognosis.
The visual prognosis of endogenous bacterial endophthalmitis is generally poor. When the causative organism is a gram-negative bacillus, progression is particularly rapid and the prognosis is poor; delay in treatment initiation directly affects visual outcomes. Even after treatment, sequelae such as optic atrophy, retinal necrosis, and retinal vascular sheathing often remain, leading to poor visual prognosis in many cases 1). After healing, choroidal neovascularization and maculopathy may also occur 1).
A systematic review of 342 cases showed that most patients had a final visual acuity of 20/200 (0.1) or worse, and only a limited number of patients were able to maintain adequate vision 2). Studies on prognostic factors for Klebsiella pneumoniae liver abscess-associated endophthalmitis have reported that initial visual acuity and the degree of vitreous opacity at the first visit are major predictors of final visual acuity3).
In cases where vitreous abscess has formed or panophthalmitis has developed, enucleation may be unavoidable.
In the long term, appropriate management of underlying diseases (liver abscess, diabetes, malignant tumors, etc.) is essential for both recurrence prevention and life prognosis. Continued treatment of the primary infection site through multidisciplinary collaboration with internal medicine and infectious disease departments also has a positive impact on ophthalmic prognosis. From an ophthalmological perspective, regular postoperative fundus examinations and OCT follow-up of the retina and macula are important.
It is important for both patients and the medical team to share the understanding that prompt diagnosis and simultaneous treatment of the primary infection site through multidisciplinary collaboration (ophthalmology, internal medicine, infectious disease) are most critical for improving both visual and life prognosis 4)5).
Jackson TL, Paraskevopoulos T, Georgalas I.. Systematic review of 342 cases of endogenous bacterial endophthalmitis. Surv Ophthalmol. 2014;59(6):627-635. doi:10.1016/j.survophthal.2014.06.002. PMID:25113611.
Marcus Ang, Aliza Jap, Soon-Phaik Chee. Prognostic Factors and Outcomes in Endogenous Klebsiella pneumoniae Endophthalmitis. American Journal of Ophthalmology. 2011;151(2):338-344.e2. doi:10.1016/j.ajo.2010.08.036.