Fungal endophthalmitis is a disease in which various fungi migrate into the eye, causing intraocular inflammation and visual impairment. It is classified into endogenous (hematogenous endophthalmitis), which spreads hematogenously from an extraocular infection focus, and exogenous, which occurs after surgery or trauma. Most cases are endogenous; exogenous cases are rare. It accounts for a portion of infectious uveitis1).
The main causative organisms are Candida species (majority), Aspergillus species, and Fusarium species. Intraocular lesions are reported in patients with candidemia, but the frequency varies greatly depending on the definition and screening method. Unlike bacterial endophthalmitis, it progresses relatively slowly while forming distinct focal lesions in the fundus, making diagnosis often delayed. Endogenous fungal endophthalmitis can occur bilaterally6).
If prolonged, extensive retinal necrotic changes occur, and visual prognosis after treatment is poor. If tractional retinal detachment develops, surgery is required, but visual prognosis is often poor. Early detection and treatment are key to visual prognosis.
QWhat symptoms should raise suspicion for fungal endophthalmitis?
A
When the triad of “floaters + history of IVH (central venous nutrition) + fever” is present, strongly suspect fungal endophthalmitis. Floaters, blurred vision, and decreased visual acuity are common initial symptoms. Early ophthalmologic evaluation should be considered in febrile patients on IVH or those diagnosed with candidemia 2).
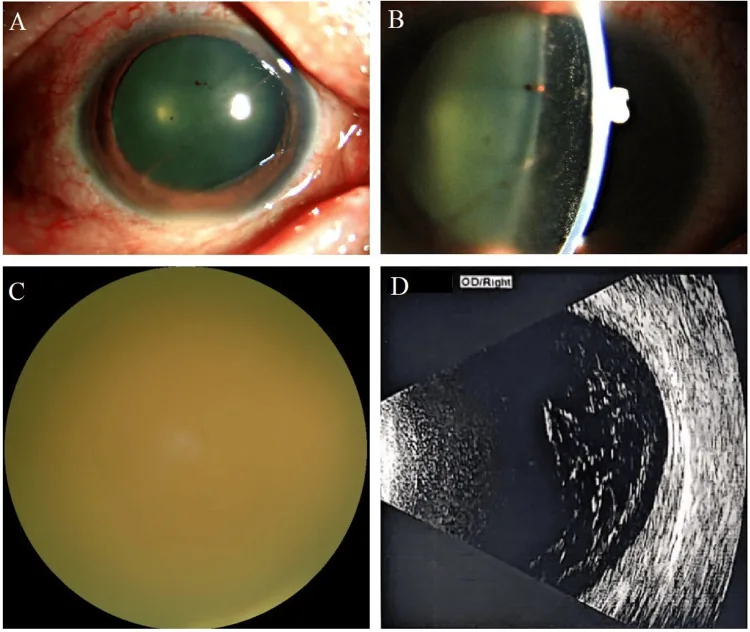
Wang N, et al. Endogenous Fungal Endophthalmitis Following Eyebrow Tattooing: A Case Report. Cureus. 2025. Figure 2. PMCID: PMC12553984. License: CC BY.
Anterior segment and slit-lamp photographs show ciliary injection, inflammatory cells in the anterior chamber, and flare. Fundus photography reveals poor fundus visualization due to severe vitreous opacities, and B-scan confirms extensive opacities within the vitreous.
Since fungal endophthalmitis develops following fungemia, fever is always present. Early ocular symptoms include floaters, blurred vision, and mild visual loss, which objectively appear as fine dust-like vitreous opacities. As the disease progresses, photophobia, eye pain, and severe visual loss develop. About 30% of endogenous cases are bilateral, and the asymptomatic fellow eye may also harbor lesions.
Unlike rapidly progressing bacterial endophthalmitis (hours to days), fungal endophthalmitis progresses slowly over weeks to months while forming distinct focal lesions in the fundus. Systemic background such as history of IVH use, fever, and immunosuppression is also important for differentiation.
Advanced malignancy, bone marrow/organ transplant, hematologic malignancies (leukemia, malignant lymphoma), AIDS, severe infections, diabetes, collagen diseases, heart disease
Others
Trauma, malnutrition, advanced age
Exogenous (rare)
After intraocular surgery, after ocular trauma
IVH (central venous nutrition) is the most important risk factor. Skin commensal yeasts cause systemic infection via central venous catheters, leading to candidemia. Intraocular lesions have been reported in patients with candidemia, and the IDSA 2016 guidelines recommend early ophthalmologic evaluation2,3).
The IDSA 2016 guidelines recommend ophthalmologic evaluation early after initiation of treatment for candidemia2).
QIs ophthalmologic consultation always necessary for candidemia?
A
In patients with candidemia, intraocular lesions may be found even without symptoms, and the IDSA 2016 guidelines recommend early ophthalmologic evaluation after starting treatment2). However, there is debate regarding screening targets and the definition of endophthalmitis; decisions are made jointly by internal medicine and ophthalmology based on the patient’s general condition and ocular symptoms6).
In addition to the “triad (floaters + history of IVH + fever)”, confirmation of characteristic fundus findings (small round white lesions in the posterior pole, fungus ball, diffuse vitreous opacity) is important. Unlike bacterial endophthalmitis, it progresses relatively slowly, which aids in differentiation. It often develops some time after IVH is discontinued.
Diabetic retinopathy: History of diabetes, retinal neovascularization, proliferative membranes.
QHow to differentiate bacterial from fungal?
A
Bacterial endophthalmitis progresses rapidly over hours to days and presents with severe inflammation (hypopyon, intense eye pain). In contrast, fungal endophthalmitis progresses slowly over weeks to months and is characterized by relatively well-demarcated white lesions in the posterior pole or fungus balls. The presence of systemic risk factors such as IVH use, fever, and leukopenia is also an important differentiating point.
Especially when IVH is the source of infection, promptly remove the catheter. As long as the infection source remains, antifungal drugs may not be fully effective.
Start with medical treatment (systemic administration) and decide on the strategy while observing the treatment response. Retinal infiltrates begin to gradually shrink within 1–2 weeks after starting treatment, and continue until the lesions are completely scarred even after switching to oral medication. Usually, 3 weeks to 3 months of medication is required.
Fluconazole (Diflucan®/Prodif®): 200–400 mg/day IV1). High intraocular penetration, standard treatment for Candida endophthalmitis. Water-soluble, penetrates well into aqueous humor and vitreous cavity, particularly effective against Candida albicans.
Severe cases/fluconazole-resistant strains: Liposomal amphotericin B (L-AmB)2).
Voriconazole (Vfend®): Important systemic antifungal for aspergillosis, with switch from IV to oral administration4). Expected intraocular penetration, but monitor for visual symptoms and liver dysfunction.
Micafungin (Fungard®): 50–150 mg/day (IV infusion, once daily)1). Effective against aspergillosis.
For cases that respond poorly to systemic treatment or when intraocular proliferative changes have already progressed, vitrectomy should be performed after consultation with other departments, if possible. When vitreous opacity progresses, early diagnosis and aggressive vitrectomy are desirable.
Indications include cases with fungus ball formation, proliferative membranes, or combined tractional retinal detachment.
Fluconazole 10–20 µg/mL may be added to the irrigation fluid during surgery (off-label use).
QHow long does treatment last?
A
Although it varies depending on the severity of endophthalmitis, the type of causative organism, and treatment response, retinal infiltrates gradually begin to shrink within 1–2 weeks after starting systemic treatment. After switching to oral medication, treatment should continue until the lesion is completely scarred, usually requiring 3 weeks to 3 months of medication. In cases requiring vitrectomy, continued administration of antifungal drugs is necessary after surgery.
6. Pathophysiology and Detailed Mechanism of Onset
Candida species (especially Candida albicans), which are commensals on the skin and gastrointestinal tract, can breach the intestinal mucosal barrier or enter the bloodstream via central venous catheters due to IVH use, long-term antibiotic use, or immunosuppression. Once fungemia is established, the fungi reach the choroidal capillaries hematogenously and establish infection.
Sequence of lesion progression:
Fungal colonization of the choroid → invasion into the inner retina through the retinal pigment epithelium → formation of retinitis → spread into the vitreous cavity → fungus ball formation → formation of inflammatory proliferative membranes → tractional retinal detachment
In hosts with preserved immune function, fungal endophthalmitis progresses relatively slowly and forms well-defined focal lesions in the fundus. In contrast, in neutropenia, AIDS, or post-transplant immunosuppression, it progresses rapidly, and filamentous fungi such as Aspergillus and Fusarium are more likely to cause disease 6).
For fluconazole-resistant Candida glabrata and Candida krusei, selection of antifungal agents based on drug susceptibility testing (minimum inhibitory concentration: MIC measurement) is important 2,7).
Endogenous fungal endophthalmitis can occur in both eyes. If prolonged, it leads to extensive retinal necrotic changes, and the visual prognosis after treatment is poor. In patients with poor general condition, control of fungemia becomes difficult, and ocular symptoms may recur.
In endophthalmitis caused by filamentous fungi (Aspergillus, Fusarium), the use of intravitreal voriconazole (100 µg/0.1 mL) alone or in combination with systemic administration has been reported in case series 5). Accumulation of future dose optimization data is expected.
Regarding routine ophthalmologic screening for candidemia patients, systematic reviews have discussed its usefulness and the potential for overdiagnosis and intervention 8). Standardizing the target, timing, and definition of evaluation including asymptomatic cases remains a future challenge.
To address fluconazole-resistant Candida species, the importance of individualized treatment based on culture identification and MIC is increasing 2,7). When intraocular specimens are available, culture and molecular diagnostics should be combined with systemic testing to identify the causative organism.
Pappas PG, Kauffman CA, Andes DR, et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62(4):e1-e50. doi:10.1093/cid/civ933. PMID:26679628.
Oude Lashof AM, Rothova A, Sobel JD, Ruhnke M, Pappas PG, Viscoli C, Schlamm HT, Oborska IT, Rex JH, Kullberg BJ.. Ocular manifestations of candidemia. Clin Infect Dis. 2011;53(3):262-268. doi:10.1093/cid/cir355. PMID:21765074.
Patterson TF, Thompson GR 3rd, Denning DW, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;63(4):e1-e60. doi:10.1093/cid/ciw326. PMID:27365388; PMCID:PMC4967602.
Sharma S, Padhi TR, Basu S, et al. Endophthalmitis caused by filamentous fungi: treatment outcomes and intravitreal voriconazole. Ophthalmology. 2014;121(3):673-678.
Lingappan A, Wykoff CC, Albini TA, Miller D, Pathengay A, Davis JL, Flynn HW.. Endogenous fungal endophthalmitis: causative organisms, management strategies, and visual acuity outcomes. Am J Ophthalmol. 2012;153(1):162-6.e1. doi:10.1016/j.ajo.2011.06.020. PMID:21917234.
Riddell J, Comer GM, Kauffman CA.. Treatment of endogenous fungal endophthalmitis: focus on new antifungal agents. Clin Infect Dis. 2011;52(5):648-653. doi:10.1093/cid/ciq204. PMID:21239843.
Breazzano MP, Day HR Jr, Bloch KC, et al. Utility of Ophthalmologic Screening for Patients With Candida Bloodstream Infections: A Systematic Review. JAMA Ophthalmol. 2019;137(6):698-710. doi:10.1001/jamaophthalmol.2019.0733. PMID:30998819.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.