Tractional retinal detachment (TRD) is a retinal detachment that occurs when strong vitreous traction is exerted on the retina in the absence of complete posterior vitreous detachment. It is a non-rhegmatogenous retinal detachment caused by proliferative tissue on the retina or vitreous traction. The detachment is often localized, flat or tent-shaped, and characteristically has little mobility.
TRD is broadly classified into the following two types based on the cause.
Traction by fibrovascular membranes (including neovascularization): Representative diseases are proliferative diabetic retinopathy (PDR), retinal vein occlusion (RVO), and retinopathy of prematurity (ROP). It is based on neovascularization in response to intraocular ischemia, and contraction of the fibrovascular membrane generates traction.
Vitreoretinal traction without neovascularization: Representative diseases are vitreomacular traction syndrome and perforating ocular trauma. It is based on proliferation after inflammation or trauma.
Retinal detachment is generally classified into three types: rhegmatogenous, tractional, and exudative. Tractional detachment is clinically distinguished from rhegmatogenous (which is bullous and mobile) and exudative detachment as a localized, immobile detachment. Some cases may have a concurrent retinal break, which is called combined tractional-rhegmatogenous RD. Combined RD is a more urgent condition and its management differs from that of pure tractional RD.
QHow is tractional retinal detachment different from rhegmatogenous retinal detachment?
A
Rhegmatogenous RD occurs when liquefied vitreous flows into the subretinal space through a retinal break, presenting as a bullous, mobile detachment. Tractional RD occurs when the retina is pulled by proliferative membranes or vitreous contraction, presenting as a tent-shaped, immobile detachment. Combined tractional-rhegmatogenous RD also exists. Differentiation is made by fundus examination, OCT, and B-scan ultrasonography.
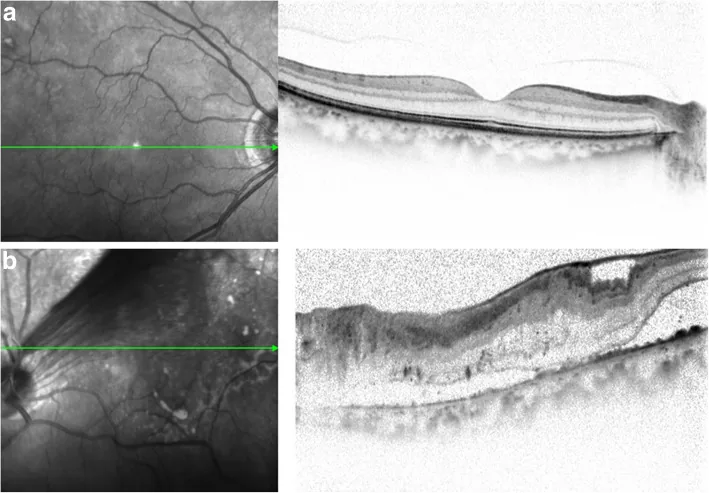
Miyamoto T, et al. A case of tractional retinal detachment associated with congenital retinal vascular hypoplasia in the superotemporal quadrant treated by vitreous surgery. BMC Ophthalmol. 2020. Figure 2. PMCID: PMC7542339. License: CC BY.
Optical coherence tomography (OCT) at initial visit shows no abnormality in the right eye (a), but tractional retinal detachment (TRD) extending to the macula is observed in the left eye (b). This corresponds to the tractional retinal detachment discussed in the section “2. Main Symptoms and Clinical Findings.”
Subjective symptoms of TRD vary greatly depending on the location and extent of the detachment.
Asymptomatic: Localized TRD outside the macula is often asymptomatic. It is often discovered incidentally during regular ophthalmologic checkups for diabetes.
Visual loss: When the detachment involves the macula, marked visual loss occurs.
Metamorphopsia: Traction or detachment involving the macula causes metamorphopsia, where objects appear distorted.
Visual field defect: A visual field defect corresponding to the area of detachment is observed.
Increased floaters: May increase with the formation of fibrovascular membranes or worsening of vitreous hemorrhage.
The characteristic morphological findings of TRD are shown below.
Tent-shaped Detachment
Mechanism: Formed when traction occurs at the base of new vessels (epicenter) or along retinal vessels.
Features: The detached area has a reverse-arch (tent-like) shape. It is immobile and often limited in height. Typical in early to mid-stage PDR.
Tabletop Detachment
Mechanism: Formed when adhesion between the fibrovascular membrane and retina is extensive. Also called Mount Fuji type.
Features: Forms a broad, flat detachment surface. It is immobile, and if it covers the entire macula, the visual prognosis is poor.
Assessment of mobility: The lack of mobility in tractional RD is an important finding. If the detachment has a dome shape or mobility, concurrent rhegmatogenous RD (combined RD) should be considered.
Presence of fibrovascular membrane: In PDR-derived TRD, a membrane structure formed by fusion of retinal new vessels and fibrous tissue is observed. The activity of the membrane (richness of vascular components, bleeding tendency) affects surgical difficulty.
Complicated vitreous hemorrhage: In proliferative diabetic retinopathy, bleeding from fibrovascular membranes may obscure the view. In such cases, B-mode ultrasound is necessary because fundus examination is difficult.
Tractional retinoschisis: When strong traction occurs on the retinal surface in proliferative diabetic retinopathy, the inner and outer layers of the retina may separate, resulting in retinoschisis. The surface shape is tent-like, and OCT is useful for diagnosis.
TRD is caused by the following underlying diseases.
1. Proliferative Diabetic Retinopathy (PDR): The most common cause of TRD. Neovascularization forms as compensation for retinal ischemia, and fibrovascular membranes proliferate and contract on the retina, leading to TRD. The Diabetic Retinopathy Clinical Practice Guidelines (1st edition) clearly state that tractional retinal detachment is one of the serious complications of PDR 1).
2. Retinopathy of Prematurity (ROP): TRD occurs in Stage 4 (partial TRD) and Stage 5 (total TRD) 4). In the immature retina with avascular zones where retinal vessels have not developed, the postnatal hyperoxic environment causes relative ischemia, leading to neovascularization.
3. Penetrating Ocular Trauma: Inflammatory cell infiltration from the perforation site and breakdown of the blood-retinal barrier (BRB) lead to intraocular proliferation, resulting in membrane formation and traction.
OCT is particularly effective for diagnosing tractional retinoschisis. It can visualize the tent-shaped surface contour caused by traction on tomographic images. It allows quantitative assessment of the degree of macular traction, separation of inner and outer retinal layers, and the extent of detachment progression toward the macula.
This is an essential examination when fundus observation is not possible due to vitreous hemorrhage or severe cataract. It can assess the presence, extent, morphology, and degree of traction of retinal detachment. Proliferative membranes may appear as high-intensity echoes.
FA is useful for assessing neovascular activity and detecting non-perfusion areas (NPAs) 1). In PDR-related TRD, understanding the extent of non-perfusion areas preoperatively helps in planning intraoperative photocoagulation.
The differential diagnosis of conditions similar to TRD is summarized below.
Differential Diagnosis
Features
Mobility
Morphology
Rhegmatogenous RD
Retinal break present
Present
Bullous
Tractional RD
Proliferative membrane present
None
Tent-shaped or tabletop
Exudative RD
No tear or proliferative membrane
None to mild
Smooth dome-shaped
Combined TRD-RRD
Tear + proliferative membrane
Present
Mixed tent-shaped and bullous
QHow is diagnosis made when the fundus is not visible due to vitreous hemorrhage?
A
B-mode ultrasound is essential. It can assess the presence, extent, and degree of traction of retinal detachment. If PDR is suspected as the cause of vitreous hemorrhage, fundus findings of the fellow eye are also used as a reference for diagnosis. OCT is used adjunctively when observation near the retinal surface is possible.
Proliferative membrane that may cause macular displacement
Consider surgery1)
Localized TRD outside the macula (no progression)
Observation possible
For localized TRD outside the macula, if there is no enlargement of the detachment or macular displacement, observation is possible with regular fundus examination and OCT monitoring. However, if signs of progression are observed, early surgery should be considered1).
The definitive treatment for TRD is traction removal via vitrectomy. In recent years, 25G and 27G microincision vitrectomy surgery (MIVS) has become mainstream, and surgery under a wide-angle viewing system is standard1).
The basic surgical procedure is as follows.
Lensectomy: Lensectomy is performed as needed to secure access to the posterior segment. In young patients (e.g., ROP), lens preservation is considered to maintain accommodative function.
Vitrectomy: The vitreous is thoroughly removed up to the periphery.
Membrane peeling: Membrane peeling is performed from the posterior pole toward the periphery using a pick or vitreous forceps. Bimanual technique may be useful in some cases.
Use of vitreous scissors: Vitreous scissors are used as appropriate in areas where the proliferative membrane is firmly adherent to the retina.
Retinal reattachment: Retinal reattachment is achieved by pneumatic retinopexy or using liquid perfluorocarbon (PFCL).
Endophotocoagulation: Endophotocoagulation is applied around the retinal breaks; in cases of PDR, panretinal photocoagulation is added intraoperatively.
Encircling band: An encircling band may be combined to counteract residual vitreous traction in the periphery.
Tamponade: Gas tamponade with long-acting gases such as 20% SF₆ or 14% C₃F₈, or silicone oil (1000 cSt) tamponade is performed.
Preoperative intravitreal anti-VEGF injection may help reduce intraoperative bleeding, iatrogenic breaks, and surgical time 3). It is considered in PDR-associated TRD with high fibrovascular membrane activity.
Postoperative vitreous hemorrhage (rebleeding): Rebleeding may occur from residual fibrovascular membranes or neovascularization1).
Iatrogenic tears and reproliferation of fibrovascular membranes: Membrane reformation may occur after vitrectomy1).
Retinal redetachment (anterior PVR, etc.): Redetachment due to anterior PVR is a serious complication after TRD surgery1).
Persistent subretinal fluid (SRF): SRF may remain postoperatively. Spontaneous absorption may take an average of 7–10 months6).
Management of silicone oil-filled eyes: Postoperative intraocular pressure management and appropriate timing of oil removal are necessary.
QIs surgery necessary for localized tractional retinal detachment outside the macula?
A
If there is no risk of progression to the macula, observation is possible. However, if there is an enlarging detachment or proliferative membranes that may cause macular ectopia, earlier surgery should be considered. Regular fundus examination and OCT monitoring for progression are important.
TRD derived from proliferative diabetic retinopathy develops through the following stages.
Formation of retinal ischemia: Diabetic vascular complications progress, impairing retinal blood flow, leading to hypoxia and ischemia. HIF-1α (hypoxia-inducible factor) is activated.
Elevation of VEGF: Through activation of HIF-1α, VEGF (vascular endothelial growth factor) is overproduced.
Formation of new blood vessels: Stimulated by VEGF, new blood vessels form on the optic disc (NVD) or on the retina (NVE).
Formation of fibrovascular membrane: Fibrous tissue proliferates along with new blood vessels, forming a fibrovascular membrane on the retina.
Contraction of the membrane and generation of traction: The fibrovascular membrane contracts, generating traction on the retina.
Onset of TRD: When the traction force exceeds the adhesion between the retinal pigment epithelium (RPE) and the sensory retina, TRD occurs.
Pathology of TRD from PDR
The chain of ischemia → VEGF → new blood vessels forms the basis.
Contraction of the fibrovascular membrane generates traction on the retina, leading to TRD. Cytokine leakage due to breakdown of the blood-retinal barrier (BRB) promotes proliferation.
Pathology of TRD from ROP
Immaturity of retinal vessels → avascular zone → ischemia → new blood vessels form the basis.
The relative ischemia caused by the high-oxygen environment after birth leads to fibrovascular proliferation on the ridge, which extends into the vitreous, resulting in Stage 4-5 TRD.
The basis of TRD is disruption of the blood-retinal barrier (BRB). When the BRB is disrupted, the intraocular inflammatory and angiogenic environment intensifies, and fibrovascular proliferation progresses. RPE, glial cells, macrophages, fibroblasts, and others are involved in the formation of proliferative membranes 9).
Not only RPE but also glial cells, macrophages, fibroblasts, and others are complexly involved in the proliferative membrane. Contraction of collagen causes traction on the retina, leading to the development of TRD.
In TRD after penetrating ocular trauma, intraocular proliferation progresses due to inflammatory cell infiltration from the perforation wound and BRB disruption. Proliferation of fibroblasts and RPE forms a proliferative membrane, which contracts and causes traction, leading to TRD.
The Diabetic RetinopathyVitrectomy Study (DRVS), which examined the efficacy of early vitrectomy for severe diabetic vitreous hemorrhage, provides evidence that forms the basis of TRD management. In type 1 diabetes with severe vitreous hemorrhage, the proportion achieving corrected visual acuity of 20/40 or better at 2 years was 25% in the early vitrectomy group (vs. 15% in the observation group), and in type 1 diabetes, 36% vs. 12%, showing a significant difference 5). No significant difference was observed in type 2 diabetes 5).
In a trial comparing intravitreal aflibercept injection and vitrectomy plus panretinal photocoagulation (PRP) for diabetic vitreous hemorrhage, no significant difference in visual improvement was observed at 24 weeks. However, resolution of vitreous hemorrhage was faster in the surgery group (4 weeks vs. 36 weeks) 2).
Meta-Analysis of Preoperative Anti-VEGF Administration
A meta-analysis examining the usefulness of preoperative anti-VEGF administration reported a reduction in intraoperative bleeding and iatrogenic tears 3). However, it has been pointed out that traction may temporarily worsen after anti-VEGF injection, and early surgery within 1–2 weeks after injection is recommended 2).
With the widespread use of 25G and 27G systems and wide-angle viewing systems, the indications for minimally invasive vitrectomy for PDR-derived TRD have expanded 1). Small-incision techniques contribute to reduced postoperative inflammation and faster recovery, and their application in outpatient surgery is increasing 8, 9).
Potential and Limitations of Anti-VEGF Monotherapy for PDR Management
In DRCR Protocol S, anti-VEGF (ranibizumab) showed non-inferiority to PRP at 2 years 2). However, there was no significant difference in the rate of progression to TRD, and anti-VEGF alone cannot manage existing TRD. Anti-VEGF may be considered for TRD prevention, but once TRD develops, vitrectomy is the definitive treatment.
QCan tractional retinal detachment be treated with anti-VEGF injections alone?
A
Improvement of TRD with anti-VEGF injections alone is generally not expected. Anti-VEGF is effective for regression of neovascularization but cannot control contraction of existing fibrous proliferative membranes; some reports even indicate worsening of traction after injection 2). The principle treatment for TRD is vitrectomy. Preoperative anti-VEGF administration may be useful in some cases, potentially reducing intraoperative bleeding and iatrogenic breaks 3).
Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025 Apr;132(4):P75-P162. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.
Dervenis P, Dervenis N, Smith JM, Steel DH. Anti-vascular endothelial growth factors in combination with vitrectomy for complications of proliferative diabetic retinopathy. Cochrane Database Syst Rev. 2023;5(5):CD008214. doi:10.1002/14651858.CD008214.pub4.
Aggarwal D, et al. Persistent subretinal fluid following vitrectomy for tractional retinal detachment in diabetic eye disease. BMJ Case Rep. 2022;15:e249745.