Retinopathy of Prematurity (ROP) is a proliferative disease of the developing retinal blood vessels.
Retinal blood vessels begin to develop from the optic disc around the 14th week of gestation and grow anteriorly across the fundus. Superficial vessels reach the periphery by the 30th week, and deep vessels by the 38th to 40th week, completing growth. There are individual differences; the temporal side is longer from the optic disc than the nasal side, so it reaches the periphery later and is more prone to ROP.
In preterm infants, the peripheral retina remains avascular at birth. When the environment changes abruptly from the stable mother, the developing vessels stop growing at the most immature leading edge and proliferate abnormally. VEGF (vascular endothelial growth factor) released from the avascular area is the mechanism.
The period of active proliferation is called the active phase, and the state after quiescence with regression of vascular components and sequelae such as fibrous connective tissue and retinal traction or degeneration is called the cicatricial phase.
The incidence and severity of ROP are higher when retinal vascular growth is more immature. Lower gestational age and birth weight increase the incidence and severity. High-concentration oxygen is the most significant trigger for worsening ROP; other factors include respiratory distress syndrome, exchange transfusion, sepsis, intraventricular hemorrhage, history of surgery, and imbalances in nutrition and fluid administration.
First reported by Terry in 1942, the first photocoagulation treatment in the world was performed by Nagata in 1967, and it has since developed into a standard therapy. There have been three historical epidemics of retinopathy of prematurity 1): the first (1940s–1950s) was caused by high-concentration oxygen in incubators, the second (1970s–1980s) accompanied improved survival of extremely low birth weight infants, and the third is currently ongoing in low- and middle-income countries with limited medical resources 1). The proportion of childhood blindness due to ROP was about 10% in 1990 but has now risen to 30%. Worldwide, an estimated 184,700 preterm infants develop ROP annually, and about 20,000 children become blind or severely visually impaired 1). Among extremely low birth weight infants (<1,000 g), 86.1% develop ROP, and 41% require treatment. The incidence of ROP in the United States increased from 4.4% in 2004 to 8.1% in 2019 1).
The approximate incidence rates are as follows.
Group
Incidence
Extremely low birth weight (<1,000 g), Japan
86.1%
Gestational age ≤27 weeks, United States
89.0%
Gestational age 27–31 weeks, United States
51.7%
Gestational age ≥32 weeks, United States
14.2%
All births (overall), United States
0.12%
The main risk factors are shown below 1).
Risk factors
Details
Gestational age < 32 weeks
One of the most important risk factors
Birth weight < 1.5 kg
One of the most important risk factors
High-concentration, prolonged oxygen therapy
Major trigger for onset
Multiple pregnancy
Leads to low birth weight
Neonatal respiratory distress syndrome (NRDS)
Severe cases requiring respiratory management
Sepsis, intraventricular hemorrhage
Systemic inflammation, circulatory disturbance
Delayed postnatal weight gain
Associated with low IGF-1 levels
Blood transfusion / Erythropoietin administration
Changes in oxygen-carrying capacity
QWhich babies are more likely to develop retinopathy of prematurity?
A
The shorter the gestational age and the lower the birth weight, the higher the risk of developing ROP. Preterm infants born before 32 weeks of gestation or with a birth weight less than 1,500 g are the main risk group. Postnatal environmental factors such as high-concentration oxygen therapy also contribute to the onset. When multiple risk factors overlap, the condition tends to become severe.
Since the acute phase of retinopathy of prematurity occurs during the neonatal and infant periods, the affected infant cannot complain of symptoms. Parents or healthcare providers may notice the following signs.
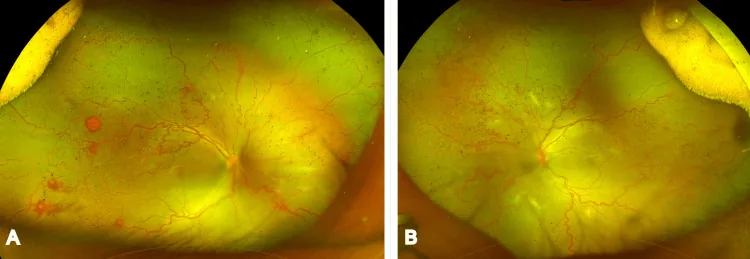
Jain KS, et al. Zone 3 Aggressive Retinopathy of Prematurity in a Near-Term Delivered Big Baby With a Birth Weight of 3,200 g. Cureus. 2026. Figure 1. PMCID: PMC13016036. License: CC BY.
Ultra-widefield fundus photographs of both eyes show marked dilation and tortuosity of retinal vessels, abnormal peripheral retinal vessels, and hemorrhages. These are active clinical findings of retinopathy of prematurity, corresponding to the staging discussed in the section “Main symptoms and clinical findings.”
In Japan, the Ministry of Health and Welfare classification was created in 1975 and revised in 1983. It divided ROP into type I (Classic ROP), which progresses in stages, and type II (fulminant), which rapidly leads to retinal detachment. The International Classification (ICROP) fully incorporated the concepts of the Ministry of Health and Welfare classification in its 2005 revision, and the content is almost the same. The latest ICROP third edition (ICROP3) was published in 20212).
Correspondence between the Ministry of Health and Welfare Classification and ICROP3
Ministry of Health and Welfare Classification
International Classification (ICROP3)
Type I Stage 1: Intraretinal neovascularization
Stage 1: Demarcation line
Type I Stage 2: Demarcation line formation
Stage 2: Ridge
Type I Stage 3: Vitreous exudation and proliferation (early/mid/late)
The location of the lesion is expressed as zones I to III. Zone I is the area inside a circle centered on the optic disc with a radius twice the distance between the optic disc and the fovea, corresponding to the area visible when the edge of a +25 D or +28 D viewing lens is placed at the opposite edge of the optic disc. Zone II is the area outside zone I, inside a circle with a radius from the optic disc to the nasal ora serrata. Zone III is the temporal crescent area outside zone II. The more posterior the lesion (zone I), the higher the severity. ICROP3 added the concept of posterior zone II (a band-shaped area 2 disc diameters from the zone I boundary) 2).
Stage 1 (Demarcation line): A white demarcation line forms within the retina at the leading edge of vascular growth.
Stage 2 (Ridge): Proliferation of mesenchymal cells in the anterior region thickens, and the demarcation line protrudes into the vitreous cavity, forming a ridge.
Stage 3 (Extraretinal fibrovascular proliferation): Vascular tufts fuse to form an arc, and new vessels in the vitreous form vascular lumens, with surrounding connective tissue such as collagen produced. Findings are classified into mild, moderate, and severe. ICROP3 added the concept of flat neovascularization without a ridge to Stage 3 2).
Stage 4 (Partial retinal detachment): Connective tissue within the fibrovascular proliferation contracts, pulling the retina and causing partial retinal detachment. Classified as 4A (not involving the macula) and 4B (involving the macula).
Stage 5 (Total retinal detachment): Fibrovascular proliferation is extensive and strongly contracts, causing total retinal detachment. ICROP3 classified Stage 5 into the following three subtypes 2).
Subtype
Characteristics
5A
Optic disc visible on ophthalmoscopy (open funnel detachment)
5B
Retrolental fibrovascular tissue or closed funnel; optic disc not visible
In stages 1 to 3, when there is dilation of retinal veins and tortuosity of arteries in two or more posterior quadrants, it is defined as plus disease. In ICROP3, plus disease was revised to be understood as a continuous spectrum from normal through pre-plus to plus 2). Evaluation of plus disease is performed on vessels within zone I.
In ICROP3, the former AP-ROP (Aggressive Posterior ROP) was renamed A-ROP. This is because the definition was expanded to include onset in non-posterior locations, as well as in larger preterm infants and in regions with limited resources 2).
The characteristics of A-ROP are as follows. It occurs posteriorly (often in zone I, also including posterior zone II), with prominent plus disease and circumferential shunt formation. The boundary between vascularized and avascular retina is indistinct, and intraretinal neovascularization is flat and translucent, making it difficult to identify. It does not show the usual stepwise progression from stage 1 to stage 3, and if untreated, rapidly progresses to stage 5. There is extensive lack of capillary network including the posterior pole, and widespread VEGF release underlies the rapid progression.
If shunts or intraretinal hemorrhages are seen at the tips of retinal vessels in the early lesions, photocoagulation should be performed immediately.
Cicatricial stage classification (Ministry of Health and Welfare)
The development of retinopathy of prematurity involves an interaction between immature retinal vasculature and the postnatal oxygen environment and systemic condition. High-concentration oxygen is the most significant trigger that worsens ROP, and other factors such as respiratory distress syndrome, exchange transfusion, sepsis, intraventricular hemorrhage, history of surgery, and imbalances in nutrition and fluid administration are also complexly involved.
Risk Factor
Description
Gestational age
<32 weeks is high risk
Birth weight
<1,500 g is high risk
Oxygen therapy
High concentration and long-term administration
Low IGF-1
Postnatal malnutrition and disease1)
Sepsis, anemia, transfusion
Worsening of general condition
Respiratory distress syndrome
Severe infants requiring respiratory management
Multiple birth
Advanced ROP is more common in the smaller twin 1)
Poor postnatal weight gain
Basis for WINROP/G-ROP algorithm 1)
IGF-1 (insulin-like growth factor-1) is an essential signaling factor for retinal vascular development, and low IGF-1 levels after preterm birth promote arrest of vascular growth 1).
Retinal vascular development begins around the 14th week of gestation and is completed by reaching the most peripheral areas before birth. Superficial vessels reach the periphery by 30 weeks, and deep vessels by 38-40 weeks. In preterm infants, avascular areas remain in the peripheral retina at birth.
The pathophysiology of ROP is explained in two phases 1).
Phase 1 (vaso-obliteration phase): When the immature retina of a preterm infant is exposed to a high-oxygen environment (extrauterine), oxygen sensors suppress VEGF and IGF-1. This halts normal retinal vascular development, forming avascular zones.
Phase 2 (vasoproliferative phase): As the avascular retina matures metabolically, VEGF is overproduced to compensate for the ischemic state. This excess VEGF induces abnormal proliferation of vascular endothelium, leading to fibrovascular proliferation into the vitreous cavity (Stage 3 and beyond).
New blood vessels grow along the fibers of the formed vitreous in the vitreous cavity and produce connective tissue such as collagen around them. When this connective tissue contracts and pulls on the attached retina, retinal detachment occurs, leading to severe visual impairment or blindness.
In A-ROP, there is extensive capillary dropout including the posterior pole, and VEGF is released from a wide area including the posterior pole, causing rapid progression.
IGF-1 (insulin-like growth factor-1) is important for coordinating retinal vascular and neural development, and low IGF-1 levels delay normal vascular development and increase susceptibility to ROP 1). Delayed postnatal weight gain is also associated with low IGF-1 and is a risk factor 1).
Crunch syndrome: When VEGF is suppressed after anti-VEGF therapy, the relative increase in TGF-β (a profibrotic factor) disrupts the VEGF-TGF-β balance, leading to rapid contraction of the fibrovascular membrane. This may worsen tractional retinal detachment1).
In the NICU, screening is indicated for infants with gestational age less than 34 weeks or birth weight ≤ 1,800 g. Additionally, infants with oxygen therapy, mechanical ventilation, blood transfusion, sepsis, intraventricular hemorrhage, severe respiratory or circulatory disorders, general anesthesia surgery, or hydrops fetalis are considered high-risk and require fundus examination even if they do not meet the above criteria.
Treatment indications are based on the criteria for type 1 ROP from the ETROP study 1). If any of the following apply, treatment within 72 hours of diagnosis is recommended.
① Any ROP in zone I with plus disease
② Zone I stage 3 ROP without plus disease
③ Zone II stage 3 ROP with plus disease
④ A-ROP (perform as soon as possible)
All other cases are considered type 2 ROP and followed up. Zone II stage 2 ROP with plus disease is managed differently depending on the drug used (excluded in the RAINBOW trial but included in the FIREFLEYE trial) 3).
The recommended examination intervals based on findings are shown below 1).
Finding
Next examination interval
Zone I immature vessels or stage 1-2, posterior zone II immature vessels, suspected A-ROP
Weekly
Posterior zone II immature retina, zone II stage 2, zone I regression phase
1-2 weeks
Zone I stage 1, zone II immature vessels (no ROP), zone II regression phase
2 weeks
Zone III stage 1-2, Zone III regressing
2-3 weeks
Screening termination criteria are complete vascularization up to zone III, or no type 1 ROP at 45 weeks postmenstrual age. After anti-VEGF therapy, observation must continue until at least 65 weeks postmenstrual age 1).
Mydriasis is achieved by instilling Mydrin®P or a mixture of Neosynesin®·Mydrin®P·Cyplegin® in a 2:1:1 ratio (modified Capto eye drop method) three times every 10 minutes starting 1 hour before examination.
Wide-field fundus camera (RetCam, etc.): Enables wide-field fundus photography under mydriasis. Also used for remote reading.
AI-based image diagnosis: Automated detection of plus disease has been reported to have accuracy comparable to or better than that of ophthalmology specialists 1). A deep learning model-based vascular severity score (VSS) has been developed as an objective indicator for plus disease diagnosis 1).
Prediction models (G-ROP, WINROP): Based on gestational age, birth weight, and postnatal weight gain, they achieve 100% sensitivity in predicting type 1 ROP 1).
FIRST-ROP algorithm: For moderate-risk infants (gestational age ≥27 weeks and birth weight ≥800 g), it has been proposed that screening initiation can be delayed until 34 weeks postmenstrual age 1).
Fluorescein angiography: Useful for assessing the presence and extent of recurrence. Expected to be used for PAR evaluation 3).
QWhen and how often will screening examinations be performed?
A
For infants born before 26 weeks gestation, the first examination starts at 29 weeks postmenstrual age; for those born at 26 weeks or later, it starts at 3 weeks after birth. Thereafter, examinations are repeated every 1-3 weeks depending on findings. After anti-VEGF treatment, continued observation until at least 65 weeks postmenstrual age is recommended 3). The examinations end when retinal vascularization is complete without findings requiring treatment.
It depends on the gestational age at birth. For infants born before 26 weeks of gestation, the first fundus examination starts at a corrected gestational age of 29 weeks; for those born at 26 weeks or later, it starts at 3 weeks after birth. Screening is indicated for infants born before 34 weeks of gestation or with a birth weight of 1,800 g or less, but even if outside these criteria, examination is necessary if risk factors such as oxygen therapy, blood transfusion, or sepsis are present.
Since Nagata performed the world’s first photocoagulation treatment in 1967, it has been established as the standard treatment for ROP. The basic approach is photocoagulation of the entire avascular area, performed under indirect ophthalmoscopy. It may be difficult in cases with prominent tunica vasculosa lentis or pupillary rigidity. The procedure is time-consuming and requires operator skill; extensive coagulation may cause visual field constriction and myopia.
In the CRYO-ROP study, the unfavorable structural outcome at 1 year was 25.7% in the cryotherapy group vs. 47.4% in the observation group, and the difference persisted at 15 years (30% vs. 52%)8). The ETROP study showed that early treatment reduced unfavorable structural outcomes from 15.6% to 9.1%9).
Since VEGF is involved in retinal neovascularization, intravitreal injection of anti-VEGF agents has been attempted for ROP. As of December 2022, the following two anti-VEGF drugs are approved for ROP treatment in Japan3).
Ranibizumab (Lucentis®): 0.2 mg/injection (0.02 mL). Approved in Japan in November 2019.
Aflibercept (Eylea®): 0.4 mg/injection (0.01 mL). Approved in Japan in September 2022.
Both are approved for ROP only as vial formulations, and the re-injection interval is at least 1 month according to the package insert3). Bevacizumab is not approved for ROP in Japan or abroad3).
Results of major clinical trials
Trial name
Population/Drug
Main results
BEAT-ROP
zone I Stage 3+, bevacizumab 0.625 mg
Recurrence in zone I: 6% vs laser 42%5, 1)
RAINBOW
Birth weight <1,500 g, ranibizumab 0.2 mg
Treatment success rate 80.0% vs laser 66.2%. High myopia at 2 years: 5% vs 20%6, 1)
FIREFLEYE
Gestational age ≤32 weeks or weight <1,500 g, aflibercept 0.4 mg
Success rate 82.7% vs laser 84.2%. General anesthesia rate 44.0% vs 65.8%7, 1)
Comparison of recurrence rates3):
Aflibercept: recurrence rate 13.9–28%, mean time to recurrence 11–14.2 weeks
Ranibizumab does not show detectable reduction in blood VEGF by day 14 after injection, suggesting minimal systemic effects. With aflibercept, plasma free aflibercept decreases to the lower limit of quantification approximately 8 weeks after injection3).
Injection technique specific to children3):
Insert 1.0–1.5 mm posterior to the limbus (note the difference from 3–4 mm in adults)
Because the lens is relatively large, insert downward (posteriorly). Directing toward the center of the eye carries a risk of lens injury
Use a 30-gauge or smaller needle
Perform in an NICU incubator or operating room
Choose anesthesia from topical, intravenous, or general anesthesia according to the facility
The goals of anti-VEGF therapy can be divided into three categories. First, adjunctive therapy (buying time before vitrectomy); second, salvage therapy (preventing progression of retinal detachment when photocoagulation is ineffective); and third, monotherapy (standalone treatment as an alternative to photocoagulation). After monotherapy, ROP has been reported to regress and blood vessels grow into avascular areas, but proliferation may recur over the long term (smoldering retinopathy).
Surgical treatment is required for retinal detachment at stage 4 or later. In type I/classic ROP, lens-sparing vitrectomy (LSV) is performed, achieving good retinal reattachment rates and visual outcomes. Early surgery in stage 4A affects visual prognosis. In type II/A-ROP, LSV is less effective due to high activity of fibrovascular proliferation, often requiring lens removal.
The anatomical success rate of LSV is reported as 74-91% for stage 4A, 62-92% for stage 4B, and 22-48% for stage 5 1). Expected visual acuity is 20/80 or better after stage 4A reattachment, ambulatory vision after stage 4B repair, and hand motion after stage 5 repair 1). Cataract formation after LSV is rare within 10 years, but when it occurs, it is often within the first postoperative year 1).
QWhich should be chosen: anti-VEGF therapy or laser photocoagulation?
A
The choice depends on the location and severity of the disease. According to the Anti-VEGF Therapy Guidelines (2nd edition), anti-VEGF therapy is advantageous for zone I and A-ROP, while laser remains an important option for zone II lesions 3). Anti-VEGF therapy has advantages such as ease of administration, shorter treatment time, and less burden on the infant for severe zone I cases, but it also carries risks of high recurrence rates and need for long-term regular follow-up. The decision should be made after explaining the advantages and disadvantages of each to the family.
QHow often does reactivation occur after anti-VEGF therapy?
A
It varies by drug. Reactivation has been reported in 13.9-28% with aflibercept and 20.8-83.0% with ranibizumab; in the RAINBOW trial, 31% required additional treatment 3, 1). In A-ROP, 75.0-87.5% require additional treatment, making strict early post-injection observation essential.
In ICROP3, the concepts of regression and reactivation were formally defined 2). Regression is classified into complete regression and incomplete regression. After anti-VEGF, vascular changes begin to regress within 1–3 days, whereas after laser, it takes 7–14 days. Early signs of regression include improvement of plus disease and vascular extension into the peripheral avascular area.
After incomplete regression, persistent avascular retina (PAR) may remain. PAR is more frequent and extensive after anti-VEGF compared to after laser or spontaneous regression 2). Reactivation is more common after anti-VEGF therapy, peaking at corrected age 37–60 weeks. It may be delayed depending on the drug and dose 2).
According to a multicenter retrospective study (363 eyes, 186 patients, mean age 34.5 years, mean gestational age 26.6 weeks, mean birth weight 875 g), the following long-term fundus findings of untreated ROP have been reported 4).
Risk factors for retinal detachment were gestational age ≤29 weeks (P < 0.05) and vascularization up to posterior zone 2 (P = 0.009) 4). 86.4% of retinal detachments were rhegmatogenous or mixed, and 57.9% occurred by age 30 4). 20% (28/140 eyes) of detached eyes were deemed irreparable at initial examination 4). Incomplete vascularization (zone 3 not reached) was found in 71.6% 4).
These results recommend regular examination and evaluation with ultra-widefield fluorescein angiography for untreated ROP 4).
High myopia after laser photocoagulation occurs in 20% at age 2 and 24% at 5 years. In the ranibizumab 0.2 mg group, it was significantly lower at 5% at age 2 and 8% at 5 years 1). Preterm infants have a risk of high myopia and macular abnormalities (reduced foveal avascular zone, blunting or absence of foveal depression) independent of ROP.
In untreated spontaneous regression cases, elevated intraocular pressure is observed in 23.2%, with photocoagulation alone in 23.3%, and after acute-phase surgery in 58.5% 1). In stage 5, 66.7% have elevated IOP, and in aphakic eyes, 69.8% 1). Of advanced ROP (stage 4-5), 10.0% develop glaucoma within 3 years; stage 5 carries a 6.76-fold risk compared to stage 4A, and lensectomy increases risk by 2.76-fold 1).
QCan untreated ROP cause problems in adulthood?
A
It can. In a multicenter study of untreated ROP, late complications such as lattice degeneration (54%), retinal tears (30.6%), and retinal detachment (38.6%) were found at high rates even in adulthood 4). Of retinal detachments, 57.9% occurred by age 30, making lifelong regular fundus examinations essential.
QShould I worry about my child with ROP developing myopia in the future?
A
It is a complication to be concerned about. In the laser group, high myopia at 5 years was observed in 24%, whereas in the ranibizumab 0.2 mg group it was significantly lower at 8% 1). Additionally, prematurity itself is an independent risk factor for high myopia and macular abnormalities. Follow-up including spectacle prescription and regular refraction examinations is important.
The optimal timing of laser photocoagulation for PAR after anti-VEGF therapy has not been established 1). A retrospective study suggests that prophylactic laser at 60 weeks postmenstrual age after bevacizumab is associated with reduced unfavorable structural outcomes 1). Fluorescein angiography for reactivation risk assessment (at 60 weeks PMA) has been reported useful 1).
Oral propranolol: 2 mg/kg/day has been reported to prevent progression of stage 2 ROP, but carries a risk of cardiorespiratory complications 1). Topical propranolol 0.2% eye drops have been reported safe and effective when started from stage 1 1).
AA/DHA supplementation: The Mega Donna Mega Trial (206 infants, <28 weeks gestation) reported severe ROP incidence of 15.8% in the AA+DHA group vs. 33.3% in controls (50% reduction) 1).
Caffeine: Caffeine administered for apnea of prematurity may suppress ROP progression via downregulation of VEGF and MMP 1).
Conbercept (KH902): Approved in China. Reported efficacy comparable to ranibizumab, with recurrence rates of 16.7% vs. 23.3% (ranibizumab) 1).
Deep learning models for automated detection of plus disease have achieved accuracy comparable to that of specialists 1). The Vascular Severity Score (VSS) has been developed as an objective quantitative indicator of plus disease severity 1). Telemedicine programs such as SUNDROP have expanded screening in remote areas, including low- and middle-income countries, and bedside evaluation using portable OCT is also expected 1).
Marra KV, Chen JS, Nudleman E, Robbins SL. Review of Retinopathy of Prematurity Management in the Anti-VEGF Era: Evolving Global Paradigms, Persistent Challenges and Our AI-Assisted Future. Clinical & experimental ophthalmology. 2025;53(9):1202-1217. doi:10.1111/ceo.14598. PMID:40908574; PMCID:PMC12747480.
Chiang MF, Quinn GE, Fielder AR, et al. International Classification of Retinopathy of Prematurity, Third Edition. Ophthalmology. 2021 Oct;128(10):e51-e68. doi:10.1016/j.ophtha.2021.05.031. PMID:34247850; PMCID:PMC10979521.
日本眼科学会・日本小児眼科学会. 未熟児網膜症診療ガイドライン(第2版). 2024.
Hamad AE, Moinuddin O, Blair MP, Schechet SA, Shapiro MJ, Quiram PA, et al. Late-Onset Retinal Findings and Complications in Untreated Retinopathy of Prematurity. Ophthalmology. Retina. 2020;4(6):602-612. doi:10.1016/j.oret.2019.12.015. PMID:32059986; PMCID:PMC7282927.
Mintz-Hittner HA, Kennedy KA, Chuang AZ, BEAT-ROP Cooperative Group.. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011;364(7):603-615. doi:10.1056/nejmoa1007374. PMID:21323540; PMCID:PMC3119530.
Stahl A, Lepore D, Fielder A, Fleck B, Reynolds JD, Chiang MF, et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): an open-label randomised controlled trial. Lancet (London, England). 2019;394(10208):1551-1559. doi:10.1016/S0140-6736(19)31344-3. PMID:31522845; PMCID:PMC12316478.
Stahl A, Sukgen EA, Wu WC, Lepore D, Nakanishi H, Mazela J, et al. Effect of Intravitreal Aflibercept vs Laser Photocoagulation on Treatment Success of Retinopathy of Prematurity: The FIREFLEYE Randomized Clinical Trial. JAMA. 2022;328(4):348-359. doi:10.1001/jama.2022.10564. PMID:35881122; PMCID:PMC9327573.
Cryotherapy for Retinopathy of Prematurity Cooperative Group. Multicenter trial of cryotherapy for retinopathy of prematurity: preliminary results. Arch Ophthalmol. 1988;106(4):471-479.
Good WV, Hardy RJ, Dobson V, Palmer EA, Phelps DL, Quintos M, et al. The incidence and course of retinopathy of prematurity: findings from the early treatment for retinopathy of prematurity study. Pediatrics. 2005;116(1):15-23. doi:10.1542/peds.2004-1413. PMID:15995025.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.