Morning glory disc anomaly is a congenital optic disc abnormality reported by Kindler. The disc area is enlarged and funnel-shaped, and the bottom of the excavation is covered with white tissue (glial tissue or persistent fetal vasculature = PFV). It is named because its appearance resembles the morning glory flower.
The main features of this disease are as follows:
Enlargement of the gray-white disc area and funnel-shaped excavation
Prepapillary white tissue (glial tissue or PFV) at the bottom of the excavation
Peripapillary chorioretinal pigmentary abnormality and annular elevation
Retinal vessels originate from beneath a white tissue, are numerous, and run radially and linearly.
The macula may be observed or may not be visible due to traction into the excavation.
Epidemiology: Usually unilateral; bilateral cases are rare. No clear hereditary pattern or specific risk factors are known. Visual acuity ranges from hand motion to 1.0. Quantitative epidemiological data on prevalence and incidence are not established (rare disease).
Pathophysiology: The peripapillary retina is folded into the excavation due to traction by the white tissue. It is thought that optic nervecoloboma or peripapillary staphyloma due to incomplete closure of the optic cup fissure, combined with proliferation of glial tissue or PFV on the optic disc, pulls the peripapillary retina into the excavation.
QWhat is the origin of the name "morning glory syndrome"?
A
It was named because the funnel-shaped excavation of the optic disc and the radially running vessels resemble the morning glory flower. First reported by Kindler.
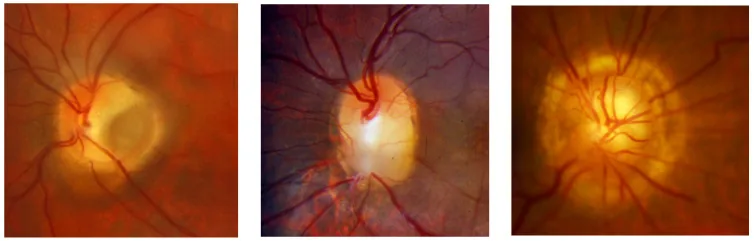
Cennamo G, et al. Congenital Optic Disc Anomalies: Insights from Multimodal Imaging. J Clin Med. 2024. Figure 1. PMCID: PMC10932420. License: CC BY.
In the fundus photograph on the right, the optic disc is deeply excavated in a funnel shape, with central white tissue and vessels extending radially to the periphery. This finding is characteristic of the optic disc morphology in morning glory syndrome.
Decreased visual acuity: Ranges from hand motion to 1.0. Depends on the size of the excavation, the position of the macula (relationship to the excavation), and the degree of retinal detachment.
Unilateral poor vision: Often present from birth; children may present with unilateral poor vision as the chief complaint.
Strabismus: May occur as disuse strabismus in cases of severe visual impairment.
Enlargement of the optic disc area and a funnel-shaped excavation are characteristic. The floor of the excavation is covered with white tissue (glial tissue or PFV), and a ring-shaped elevation is observed around the optic disc. The morphology of the optic disc itself is often unclear due to coverage by white tissue.
Vascular findings
Retinal vessels originate from beneath the white tissue. They are numerous and run radially and linearly. Because the peripapillary retina is displaced into the excavation, the vessels appear more numerous than usual.
Retinochoroidal findings
Peripapillary retinochoroidal pigmentary abnormalities are observed. A tongue-shaped area of retinochoroidal atrophy is often present inferior to the optic disc, suggesting an association with incomplete closure of the optic fissure. Peripapillary staphylomatous excavation is also characteristic.
Macular findings
The macula may be observable or may be located within the excavation and not visible. If the macula is identifiable, visual acuity is often 0.1 or better. If the macula is absent, visual acuity is severely impaired.
Morning glory syndrome is often complicated by retinal detachment that begins near the optic disc. The following mechanisms are considered as sources of subretinal fluid:
Cerebrospinal fluid theory: Cerebrospinal fluid enters the subretinal space from the subarachnoid space through fragile optic disc tissue (lamina cribrosa abnormality).
Vascular leakage theory: Serous leakage from abnormal vessels.
Traction plus hole formation theory: Tractional detachment due to vitreous traction is combined with a hole within the optic disc excavation, leading to rhegmatogenous detachment.
In the early stage, it may be exudative or tractional detachment and can resolve spontaneously. In advanced cases, a tear often develops near the prepapillary tissue. It may remain localized around the optic disc without progression, but can also progress to bullous total detachment and lead to blindness.
Incomplete closure of the optic cup fissure (embryonic fissure) is the common developmental abnormality. The optic cup fissure forms during the 4th week of gestation and closes by the 6th–7th week. In morning glory syndrome, it is thought that in addition to incomplete closure, proliferation of glial tissue or PFV at the optic disc occurs. The proposed developmental process is: optic nervecoloboma or peripapillary staphyloma + glial/PFV proliferation on the disc → pulling of the peripapillary retina into the depression.
In many cases, a tongue-shaped area of chorioretinal atrophy is seen inferior to the disc, considered a remnant of incomplete optic cup fissure closure. Whether the white tissue at the bottom of the depression is glial tissue or PFV is debated, and both may be present. Heredity is not clear, and familial occurrence is rare.
An association with transsphenoidal encephalocele is known, where meninges, optic chiasm, and hypothalamus can herniate through a bone defect in the skull base (sphenoid bone)1). Bhatti reported a 20-year-old woman with unilateral morning glory syndrome and transsphenoidal encephalocele; this case also had a history of amenorrhea, suggesting an endocrine abnormality1).
When morning glory syndrome is diagnosed, all patients should undergo head MRI to evaluate for intracranial abnormalities. Encephalocele may involve herniation of the hypothalamus or optic chiasm, and endocrine function evaluation (hypothalamic-pituitary axis) should be considered1).
Small optic disc (morning glory is enlarged). Double ring sign. Associated with maternal diabetes.
Optic nerve pit
Localized small depression. No funnel-shaped enlargement. Associated with macular schisis.
QHow is morning glory syndrome different from optic nerve coloboma?
A
Morning glory syndrome is characterized by funnel-shaped enlargement of the optic disc area, white glial tissue, and radial vascular pattern. Optic nervecoloboma is a cuplike defect below the disc, without glial tissue and with a different vascular pattern. Both are due to incomplete closure of the optic fissure, but the presence or absence of glial/PFV proliferation on the disc is key for differentiation.
Even without retinal detachment, regular fundus examinations are necessary. For localized peripapillary retinal detachment where subretinal fluid is likely derived from cerebrospinal fluid, careful observation is often chosen first.
Even without retinal detachment, if the macula is confirmed in children aged 6 years or younger, amblyopia treatment should be considered. The main approach is amblyopia training through occlusion (patching) of the healthy eye. If the macula is involved in the optic disc excavation and visual acuity is at the level of light perception, it is not indicated.
Surgical indications: Retinal detachment that has progressed beyond the peripapillary area. Often associated with a tear within the optic disc excavation.
Surgical procedure:
Vitrectomy (removal of vitreous gel and treatment of proliferative membranes)
Fluid-air exchange and drainage of subretinal fluid
First choice. Requires prone positioning postoperatively.
Silicone oil
Pediatric cases, refractory cases, cases unable to maintain prone positioning. Caution for risk of migration into the subarachnoid space.
Butyl cyanoacrylate (retinal glue)
Application to the tear site has been attempted in recurrent or refractory cases.
Prognosis: Surgery is often resistant and difficult to treat. Particularly in children under 10 years old, the peripapillary depression is severe and the lamina cribrosa abnormality is serious, leading to a tendency for poor prognosis. Even if reattachment is achieved, good visual acuity is difficult to obtain.
Incomplete closure of the optic fissure (embryonic fissure) is the common developmental abnormality underlying morning glory syndrome. The optic fissure formed in the 4th week of gestation normally closes by the 6th to 7th week; incomplete closure leads to structural abnormalities of the optic disc.
In morning glory syndrome, it is thought that incomplete closure is accompanied by proliferation of glial tissue or PFV at the optic disc. The proposed developmental process is: optic nervecoloboma or peripapillary staphyloma + glial/PVF proliferation on the disc → involvement of the peripapillary retina into the depression. The presence of a tongue-shaped chorioretinal atrophy lesion inferior to the disc in many cases is considered a remnant of incomplete optic fissure closure.
Mechanisms of retinal detachment (three hypotheses)
Multiple hypotheses exist regarding the origin of subretinal fluid.
Cerebrospinal fluid hypothesis: In morning glory syndrome, there is a structural abnormality of the lamina cribrosa, and cerebrospinal fluid from the subarachnoid space enters the subretinal space through the fragile optic disc tissue. The risk of silicone oil migration into the subarachnoid space indirectly supports the existence of this route.
Vascular leakage hypothesis: Serous leakage from abnormal vessels on the disc (vessels within white tissue) is the source of subretinal fluid.
Traction plus tear hypothesis: Tractional detachment due to vitreous traction is combined with a tear within the optic disc depression, leading to rhegmatogenous detachment. In advanced cases, tears are often found near the prepapillary tissue, and in clinical practice, the involvement of rhegmatogenous detachment is considered important.
The white tissue on the optic disc is located at the site corresponding to the lamina cribrosa and lacks normal supporting structures. This abnormality of the lamina cribrosa is thought to be associated with specific pathological conditions such as transmission of intraocular pressure, formation of cerebrospinal fluid inflow pathways, and intrusion of silicone oil.
Bhatti reported a case of a 20-year-old female with left eye morning glory syndrome complicated by transsphenoidal encephalocele1). Right eye visual acuity was 20/20, and left eye was hand motion. She had a history of amenorrhea and endocrine abnormalities. MRI confirmed an encephalocele through a sphenoid bone defect, which may involve not only the meninges but also the hypothalamus and optic chiasm1). When diagnosing morning glory syndrome, it is recommended to consider the possibility of basal encephalocele and perform a detailed head MRI in all cases1).
If detailed evaluation of optic disc and macular structures (layer-by-layer analysis) using OCT advances, the accuracy of visual prognosis prediction may improve. Elucidation of the mechanism of retinal detachment (verification of the cerebrospinal fluid theory and vascular leakage theory) is also an important issue. Accumulation of multicenter data on vitrectomy outcomes is expected to standardize surgical indication criteria and tamponade selection. Regarding the genetic background (search for causative genes), many aspects remain unclear, and accumulation of genomic research is awaited.
QIs head MRI always necessary in morning glory syndrome?
A
Since complications such as transsphenoidal encephalocele and intracranial abnormalities have been reported, detailed head MRI is recommended in all cases. Encephalocele may involve herniation of the hypothalamus and optic chiasm, and screening for endocrine abnormalities (e.g., amenorrhea) should also be considered.