Proliferative vitreoretinopathy (PVR) is an abnormal wound-healing response triggered by surgery for rhegmatogenous retinal detachment (RRD) or by the RD itself. Retinal pigment epithelium (RPE) cells, glial cells, and myofibroblasts proliferate and form fibrocontractile membranes on the anterior and posterior surfaces of the retina and at the vitreous base. Contraction of these membranes pulls on the retina, creating fixed folds and causing retinal re-detachment.
PVR is the leading cause of RD surgical failure. 75% of RD surgical failures are attributed to PVR, 3) and the overall incidence in RD is reported to be 5–10%. 3) It often develops within 30–60 days after RD surgery. 1)
In 1983, the Retina Society proposed a unified classification for PVR, and revised versions such as the Silverstone classification were published in 1991. PVR is the most important prognostic factor for rhegmatogenous retinal detachment, and early detection and appropriate intervention directly affect visual outcomes.
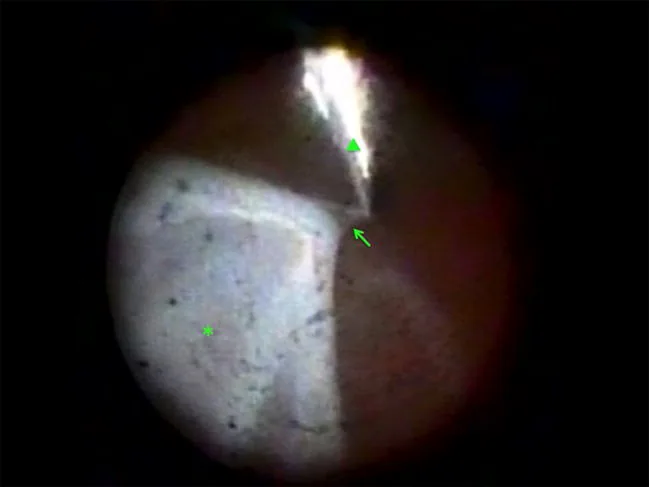
Ajlan RS, et al. Endoscopic vitreoretinal surgery: principles, applications and new directions. Int J Retina Vitreous. 2019. Figure 5. PMCID: PMC6580629. License: CC BY.
Intraocular endoscopic image during peeling of an epiretinal proliferative membrane with forceps in a case with retinal detachment and corneal opacity. This corresponds to the proliferative membrane discussed in the section “2. Main Symptoms and Clinical Findings”.
The subjective symptoms of PVR often overlap with those of the underlying retinal detachment.
Decreased visual acuity: Caused by retinal traction and re-detachment due to contraction of the proliferative membrane. When the macula is involved, significant vision loss occurs.
Metamorphopsia and distortion: In macular PVR (mPVR), caused by membrane formation directly under the macula.
Visual field defect: Visual field defects corresponding to the extent of retinal detachment persist or reappear.
Macular PVR (mPVR) develops relatively early, 10 to 28 days after PPV. 2) In reported cases, visual acuity decreased from BCVA 20/38 to 20/166 postoperatively. 2)
The most characteristic finding of PVR is fixed folds (star folds). Contraction of the proliferative membrane folds the retina, forming so-called “fixed” folds that cannot be unfolded even during vitrectomy.
Anterior PVR
Contraction of the vitreous base: The anterior retina and ciliary body are pulled forward.
Funnel-shaped retinal detachment: In severe cases, the detachment takes a funnel shape that narrows anteroposteriorly.
Strong traction: The membrane adheres to the vitreous base, making detachment difficult to treat.
Posterior PVR
Fixed folds: Contracted radial retinal folds seen from the posterior pole to the mid-periphery.
Epiretinal membrane (ERM)-like morphology: In macular PVR (mPVR), OCT shows finger-like projections. 2)
Star fold: A characteristic morphology where folds in the posterior pole converge in a star-like pattern.
Macular PVR (mPVR) shows characteristic findings on OCT. Central macular thickness (CMT) has been reported to increase markedly from 711 μm to 354 μm. 2) Differentiation from typical epiretinal membrane (ERM) is important. While ERM forms a smooth membrane on the surface, mPVR shows finger-like projections. 2)
Ultrasound shows characteristic findings: a V-shape (posterior PVR) or T-shape (severe funnel detachment).
QHow is macular PVR (mPVR) different from epiretinal membrane (ERM)?
A
Both involve membrane formation on the macular surface, but PVR is characterized by finger-like projections on OCT and early onset (10–28 days post-surgery). 2)ERM shows a relatively smooth membrane and gradual onset. Visual recovery after membrane peeling can be expected even in mPVR. 2)
The fundamental cause of PVR is breakdown of the blood-retinal barrier (BRB). When the BRB is disrupted, serum growth factors (TGF-β, PDGF, IL-6, etc.) enter the vitreous cavity and subretinal space, inducing proliferation and migration of RPE cells and neuroglial cells. RPE cells undergo epithelial-mesenchymal transition (EMT) to differentiate into myofibroblasts, 3) which produce contractile extracellular matrix (ECM).
ARN (acute retinal necrosis) causes massive breakdown of the blood-retinal barrier (BRB) and leads to severe PVR. The incidence of rhegmatogenous retinal detachment after ARN is reported to be over 50%. 5) In addition, after tractional retinal detachment (TRD) surgery in diabetic patients, persistent subretinal fluid (SRF) may occur, and renal dysfunction is a risk factor for its persistence. 4)
The diagnosis of PVR is mainly made by fundus examination using a slit-lamp microscope (with a contact lens) and an indirect ophthalmoscope. Identification of fixed folds is key to diagnosis. Fixed retinal folds that cannot be unfolded even during vitrectomy are definitive findings of PVR.
PVR classification (Retina Society classification)
In Grade C, the extent of folds is quantified by the clock-hour position (CP) they occupy. For example, “C3” means fixed folds occupying 3 clock hours.
OCT (Optical Coherence Tomography): Useful for diagnosing mPVR. It can detect finger-like projections, increased CMT, and subretinal fluid. 2)
Ultrasound (B-scan): Essential when the fundus is difficult to observe due to vitreous opacity or mature cataract. Findings include V-shaped (posterior PVR) or T-shaped (severe funnel detachment) patterns.
It is often discovered during regular follow-up visits within 30 to 60 days after RD surgery. 1) Preoperatively, risk factors such as chronic or inferior rhegmatogenous retinal detachment should be identified, and postoperatively, careful observation for the formation of fixed folds is necessary. In mPVR, detection of finger-like projections on OCT is useful for early diagnosis. 2)
The standard treatment for PVR is vitrectomy (PPV: pars plana vitrectomy) with removal of proliferative membranes and retinal reattachment. The main surgical components are as follows:
Complete vitrectomy: Thorough removal of the vitreous, which serves as a scaffold for proliferation.
Membrane peeling: Careful removal of epiretinal and subretinal membranes using forceps. In anterior PVR, treatment of membranes at the vitreous base is particularly important and technically challenging.
Intraocular tamponade: Use of silicone oil (SO) 1000 cSt or SF6/C3F8 gas. SO is often preferred for PVR.
Addition of encircling band (buckle): Scleral encircling may be effective for anterior PVR.
For macular PVR (mPVR), improvement in best-corrected visual acuity from 20/166 to 20/57 after membrane peeling has been reported, 2) and aggressive surgical intervention is recommended.
Regarding persistent subretinal fluid (SRF) after surgery, a report on diabetic TRD surgery showed residual SRF in 75% at 1 month, 50% at 3 months, 30% at 6 months, and 10% at 12 months. The mean duration was 4.4 ± 4.7 months. 4)
Methotrexate (MTX) is the most promising drug candidate, but see the section “Latest Research and Future Prospects” for details. Steroids are not considered a therapeutic target for PVR. 3)
QAre steroids effective for PVR?
A
Steroids are not considered a therapeutic target for PVR. 3) The main pathogenesis of PVR involves EMT of RPE cells and myofibroblast transformation, which steroids do not effectively suppress. Antiproliferative drugs such as MTX are under investigation.
The central pathogenesis of PVR is epithelial-to-mesenchymal transition (EMT) of RPE cells. 3)RPE cells detached by RD are released into the vitreous cavity and undergo the following changes under the stimulation of growth factors.
EMT induction: TGF-β and PDGF act as major inducing factors. RPE cells lose their epithelial morphology and function and differentiate into contractile myofibroblasts. 3)
Proliferative membrane formation: Myofibroblasts produce ECM such as collagen and fibronectin, forming membranes on the retinal surface, subretinal space, and vitreous base. 3)
Membrane contraction: The contractile activity of myofibroblasts causes the membrane to shrink, forming fixed folds.
The main cellular components of PVR membranes are as follows. 2, 3)
RPE cells (after EMT): The most important constituent cells. Free RPE cells become the core of the proliferative membrane.
Retinal glial cells (Müller cells, astrocytes): Major components of posterior PVR membranes.
Myofibroblasts: Responsible for contractility, the effector cells in the formation of fixed folds.
Anterior PVR occurs at the vitreous base (pars plana to peripheral retina). Membranes in this area pull the ciliary body, anterior retina, and vitreous base forward as a unit, leading to severe conditions such as ocular hypotony, funnel-shaped detachment, and complete blindness. Anatomically, surgery is difficult, and silicone oil tamponade is particularly important.
PVR after ARN (acute retinal necrosis) is particularly severe. 5) Massive BRB disruption caused by ARN viruses (VZV/HSV) leads to a large influx of serum proteins and inflammatory cytokines into the vitreous cavity. This provides a strong proliferative stimulus, resulting in a rhegmatogenous retinal detachment rate of over 50%, and the PVR that develops tends to be severe. 5)
7. Latest Research and Future Perspectives (Research-stage Reports)
MTX is an antifolate drug that inhibits dihydrofolate reductase, with antiproliferative and anti-inflammatory effects. Local intravitreal administration to prevent or treat PVR is being investigated worldwide.
GUARD Trial (Phase 3 RCT): Intraoperative and postoperative administration of MTX has been shown to significantly reduce the rate of redetachment, providing the most reliable evidence. 1)
Ambati et al. (2024) reported treatment of PVR cases with congenital aniridia using MTX 200 μg every 2 weeks for 5 doses followed by monthly maintenance. The GUARD trial (Phase 3 RCT) showed that intraoperative and postoperative MTX significantly reduced redetachment rates. 1)
Babel et al. (2022) reported a case of recurrent retinal detachment with PVR treated with silicone oil 1000 cSt and a single dose of MTX 400 μg/0.10 mL. 3) The half-life of MTX in the vitreous is reported to be 3–5 days, and a mechanism of PVR suppression via IL-6 inhibition has been proposed.
FIXER Trial (NCT06541574): A new Phase 3 RCT evaluating the preventive effect of MTX on PVR is currently ongoing. 1) The results of this trial may determine whether MTX becomes part of standard treatment.
Macular PVR (mPVR), localized to the macula, has recently gained attention as an independent condition occurring early (10–28 days after PPV). 2) Identification of finger-like projections on OCT is key to diagnosis, and early membrane peeling has been shown to improve visual acuity. 2)
Khateb et al. (2021) reported a case where best-corrected visual acuity decreased from 20/38 to 20/166 after PPV; membrane peeling improved it to 20/57 postoperatively. 2) CMT normalized from 711 μm to 354 μm, suggesting mPVR should be recognized as an independent clinical entity.
QIs MTX already an available treatment?
A
Currently, it is an investigational treatment at the research or clinical trial stage and is not included in standard treatment in Japan. Its efficacy is being validated in clinical trials such as the GUARD and FIXER trials, 1) which may influence future guideline revisions. Patients wishing to receive this treatment should consult their physician.
Ambati NR, et al. Intravitreal methotrexate for proliferative vitreoretinopathy. Am J Ophthalmol Case Rep. 2024;36:102216.
Khateb S, Aweidah H, Halpert M, Jaouni T. Postoperative Macular Proliferative Vitreoretinopathy: A Case Series and Literature Review. Case Rep Ophthalmol. 2021;12(2):464-472. doi:10.1159/000512285.
Babel A, Chin EK, Almeida DRP. Vitrectomy with Silicone Oil Tamponade and Single-Dose Intravitreal Methotrexate for Recurrent Retinal Detachment with Proliferative Vitreoretinopathy. Case Rep Ophthalmol. 2022;13(3):777-782. doi:10.1159/000526091.
Kang YK, Shin JP. Clinical Analysis of Persistent Subretinal Fluid after Pars Plana Vitrectomy in Macula with Diabetic Tractional Retinal Detachment. J Clin Med. 2021;10(24):5929. doi:10.3390/jcm10245929.
Tsiogka A, et al. Proliferative vitreoretinopathy following acute retinal necrosis. Cureus. 2021;13:e12430.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.