Chromovitrectomy is a general term for procedures that use vital dyes to visualize translucent intraocular tissues such as the internal limiting membrane (ILM), vitreous, and epiretinal membrane (ERM) during pars plana vitrectomy (PPV).
The main tissues that require staining during surgery are the following three:
Internal limiting membrane (ILM): The basement membrane of Müller cells. It is transparent, about 2 μm thick, and has a multilayered structure. It accounts for at least 50% of retinal rigidity 3). Around the macula, it is thickest at about 1000 μm from the fovea3).
Vitreous: Composed of collagen, hyaluronic acid, and water. Its volume is about 5 mL and it is essentially transparent.
Blue or green dyes are commonly used because they provide high contrast against the orange-red color of the retinal pigment epithelium (RPE), improving visibility of the stained area.
There are three main methods for injecting the dye.
Fluid-substitution injection: The dye is sprayed under BSS filling.
Air-substitution injection: After fluid-air exchange, the dye is dripped onto the posterior pole. This allows concentrated staining of the target area and reduces exposure to the periphery.
Injection under liquid perfluorocarbon (PFCL): A small amount is dripped under PFCL.
QWhy use dye in vitrectomy?
A
The ILM and epiretinal membrane are semi-transparent tissues only a few micrometers thick, making them difficult to identify under a surgical microscope without staining. Using dye clarifies tissue boundaries, improving the precision and safety of peeling.
The efficacy of ILM peeling in macular hole surgery has been demonstrated in multiple studies.
In the FILMS trial, the anatomical closure rate was 84% in the ILM peeling group and 48% in the non-peeling group, showing a significant difference (P<0.001)3). Since the ILM serves as a scaffold for cell proliferation, failure to remove it may allow cell proliferation to resume2).
A meta-analysis of 5480 cases showed that ILM peeling significantly reduced the reopening of macular holes2). Surgery with ILM peeling has a lower recurrence rate1). Additionally, five RCTs have investigated the extent of ILM peeling3), and research on optimizing the peeling area is ongoing.
The standard peeling technique after staining is the pinch and peel method 3). Grasp the ILM with fine forceps and peel it in a circular manner. A staining time of 5 to 10 seconds is sufficient 3), and excessive exposure increases the risk of toxicity.
QWhich is safer: the air-fluid exchange method or the fluid-filled method?
A
The air-fluid exchange method can confine the staining agent to the posterior pole, avoiding unnecessary exposure to the periphery, and is therefore safer. However, in either method, it is important to keep the staining time to about 5 to 10 seconds and avoid excessive exposure 3).
5. Characteristics and comparison of staining agents used
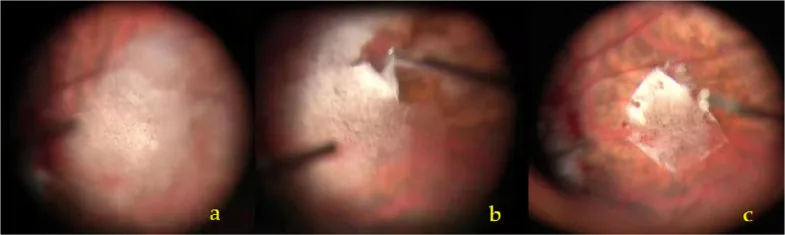
Liyan Ye; Luyun Liang; Xiaolan Liu; Xiaohua Zhu; ZhongPing Chen; Yiqin Duan. A technique of TA-assisted ILM peeling for myopic foveoschisis. BMC Surg. 2025 Dec 11; 26:33 Figure 1. PMCID: PMC12802189. License: CC BY.
a The TA granules were sprinkled evenly on the retina surface of the macular area by a 27G needle with a circular area about 2 PD centered on the macular fovea. b ILM forceps were used to grasp the flap on the temporal quadrant of the TA marked area, and peel off the ILM in the form of multiple small circles. c One optic disc diameter of the ILM was preserved in the fovea. Excessive edge of ILM was repaired with the vitrectomy tip
The main characteristics of each staining agent are shown below.
BBG (Brilliant Blue G): Selective affinity for ILM3). Epiretinal membrane and vitreous are almost unstained. No retinal toxicity. Neuroprotective effects have also been suggested.
ICG (Indocyanine Green): High affinity for type IV collagen and laminin in the ILM3). First ILM staining dye used3). Toxicity concerns exist.
Epiretinal Membrane Stains
TB (Trypan Blue): High affinity for staining epiretinal membranes. Selectively stains glial cells in the epiretinal membrane. Low affinity for ILM and vitreous. Corneal endothelial toxicity at high concentrations.
Vitreous Visualization
TA (Triamcinolone Acetonide): Deposits in the vitreous as white crystals, visualizing the vitreous 3). Not a stain but provides contrast as white crystals on the ILM. Also has anti-inflammatory effects.
A white crystalline aqueous suspension (40 mg/mL), used by injecting 0.1–0.3 mL. It whitens the vitreous and posterior vitreous cortex. Unlike stains, it provides contrast by depositing as white crystals on the ILM3). It also has anti-inflammatory effects, helping to suppress postoperative intraocular inflammation. The half-life is about 18 days in non-vitrectomized eyes and about 3 days in vitrectomized eyes. Side effects include cataract progression and increased intraocular pressure. In Japan, MacuAid (triamcinolone acetonide 40 mg/mL) is approved.
A blue food dye-derived stain with selective affinity for the ILM3). It does not stain the epiretinal membrane or vitreous, so it is used only during ILM peeling. The working concentration is 0.025% (0.25 mg/mL) in an isotonic solution. In vitro and in vivo studies have shown no retinal toxicity, and neuroprotective effects have been suggested. TB and BBG were developed after ICG and have better safety profiles 3).
In Japan, a preparation method involves dissolving 0.1 g of powder in 400 mL of BSS and sterilizing by autoclaving at 115°C for 30 minutes. The shelf life is said to be 3 months after preparation.
A blue organic dye with high staining affinity for ERM. It stains cellular components of the ERM by passing through damaged cell membranes of dead cells, making it suitable for ERM peeling surgery. It has low affinity for the ILM and vitreous. The working concentration is 0.15%, and making it a high-density solution (mixing TB with 10% glucose at a 3:1 ratio) facilitates concentration at the posterior pole. Corneal endothelial toxicity has been reported at high concentrations, and it is teratogenic, so it should be avoided during pregnancy and in children.
A green dye with high affinity for type IV collagen and laminin, which constitute the ILM3). It was the first dye used for ILM staining 3). A partial “peeling” effect (pseudo-peeling effect) on the ILM has also been reported 3). However, concerns about toxicity to the inner retina, optic nerve, and visual field defects exist 3), and current recommendations are to use low concentrations, minimal exposure time, and minimized illumination 3). Initial dilution requires distilled water (precipitation occurs in saline), followed by adjustment to final concentration with BSS. The FDA has approved it only for intravenous use; intraocular use is off-label.
QWhich dyes are available in Japan?
A
TA is approved in Japan as MacuAid. BBG and ICG have no officially approved intraocular products in Japan and are used as self-prepared or off-label. TB is also often used off-label. It is necessary to check the facility’s pharmaceutical management regulations before use.
ICG: Binds to type IV collagen, and light exposure changes the stiffness and physical properties of the ILM. This leads to a pseudo-peeling effect but also causes phototoxicity.
TB: Selectively passes through damaged cell membranes and stains dead cells and glial cell components in ERM. It is not easily taken up by viable cells, providing high selectivity.
BBG: Selectively binds to the ILM. The molecular binding mechanism is not fully understood, but it is thought to have high affinity for collagen.
TA: Water-insoluble crystals deposit in the vitreous cavity and adhere to vitreous fibers, making them visible. This is physical adhesion, not a staining reaction.
The following factors are involved in the development of toxicity.
Cause of toxicity
Relevant dye
Countermeasure
High or low osmolarity
ICG (low osmolarity is problematic)
Prepare in isotonic solution
Phototoxicity
ICG
Minimize illumination
Preservative toxicity
All formulations
Choose preservative-free formulation
Excessive exposure time
ICG, TB
Wash out within 5–10 seconds
Regarding osmotic issues, a hypo-osmotic environment may cause retinal damage due to Ca²⁺ influx. Conversely, hyperosmolarity leads to retinal contraction. One cause of ICG toxicity is thought to be injection under hypo-osmotic conditions3), so preparation in an isotonic solution is important.
Regarding preservative issues, myristyl-γ-picolinium chloride has been reported to cause severe toxicity, and preservative-free formulations are preferable. Data on benzyl alcohol are currently unclear.
Characteristic findings after ILM peeling include the following:
DONFL (dissociated optic nerve fiber layer): Round or oval dark areas appearing 2–3 months after ILM peeling3). Confirmed by fundus autofluorescence (FAF) or OCT. Often improves over time.
SANFL (forceps-related retinal nerve fiber layer changes): RNFL damage corresponding to the forceps grasping site3). Prevention is possible by improving peeling technique precision.
QWhat causes the retinal toxicity of ICG?
A
The toxicity of ICG involves multiple factors. These include Ca²⁺ influx due to injection under low osmotic pressure, photo-oxidation reactions (phototoxicity) from light exposure, and the involvement of iodine components contained in the dye 3). To reduce these risks, it is recommended to use low concentrations, short exposure times, minimize illumination, and prepare the dye in isotonic solutions 3).
7. Latest Research and Future Perspectives (Research-stage Reports)
Research on new vital dyes is ongoing to overcome the toxicity and selectivity issues of existing dyes.
Bromophenol blue: A candidate dye that may stain both ILM and ERM, and is suggested to be less toxic than ICG.
IFCG (ICG derivative without sodium iodide): Studied as a candidate substance to reduce the toxicity caused by the iodine-containing components of conventional ICG.
Patent blue: Being considered as an alternative candidate for ERM staining instead of TB.
This is a technique that promotes closure of macular holes by inverting a part of the ILM (as a flap) rather than removing it completely 3). It is being considered for use in large macular holes or refractory cases. Visualization of the ILM with vital dyes contributes to the precision of this technique.
For evaluating new vital dyes and techniques, the introduction of a stepwise surgical innovation evaluation framework such as the IDEAL framework is required. Systematic evaluation of safety and efficacy remains a future challenge.
QWhat are the promising new staining agents?
A
Bromophenol blue is a candidate staining agent that can stain both ILM and ERM and is considered less toxic than ICG. Additionally, IFCG (sodium iodide-free derivative) is being studied with a design that removes the iodine component, which is thought to contribute to ICG toxicity. Both are currently in clinical trial stages and have not yet reached standard use.
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, et al. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern®. Ophthalmology. 2020;127(2):P145-P183. doi:10.1016/j.ophtha.2019.09.022. PMID:31757497.
Christina J. Flaxel, Ron A. Adelman, Steven T. Bailey, Amani Fawzi, Jennifer I. Lim, G. Atma Vemulakonda, Gui-shuang Ying. Idiopathic Macular Hole Preferred Practice Pattern®. Ophthalmology. 2020;127(2):P184-P222. doi:10.1016/j.ophtha.2019.09.026.
Royal College of Ophthalmologists. Clinical guideline on idiopathic full-thickness macular holes. London: RCOphth; 2024.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.