Acute retinal necrosis (ARN) is a necrotizing herpetic retinopathy first reported in 1971 by Urayama et al. as “Kirisawa-type uveitis.” 2) Six cases of fulminant uveitis unprecedented at that time were described, becoming the global starting point for the disease concept of ARN.
It is characterized by onset in immunocompetent healthy individuals, and the causative viruses are HSV-1, HSV-2, and VZV. After onset, rapid retinal necrosis and elevated intraocular pressure occur, and if left untreated, it leads to blindness, so it is classified as an ophthalmic emergency. According to the national survey in the Uveitis Clinical Practice Guidelines (2019), 41 cases (1.3% of all uveitis) were reported in the 2002 survey and 53 cases (1.4%) in the 2009 survey. 1)
In immunocompromised patients, the same herpes viruses cause different disease types. CMV retinitis and progressive outer retinal necrosis (PORN) are diseases of immunocompromised patients, while ARN is positioned as a disease of immunocompetent individuals.
Epidemiologically, the annual incidence is reported as 0.5–0.63 per million population (UK) 11), and it is more common in immunocompetent adults in their 50s to 70s. Onset is unilateral in two-thirds of cases and bilateral (Bilateral ARN; BARN) in one-third 13). In recent years, associations with immune checkpoint inhibitors (ICI) 12), natalizumab 13), and dimethyl fumarate (DMF) 14) have been reported. Cases triggered by cataract surgery 15) and COVID-19 infection 16) have also been reported.
QWhat is Kirisawa-type uveitis?
A
It is another name for acute retinal necrosis (ARN), a historical name given by Urayama et al. in 1971 after their mentor, Nagatoshi Kirisawa. Even now that the international disease name ARN is established, the term Kirisawa-type uveitis is sometimes used, especially in Japan.
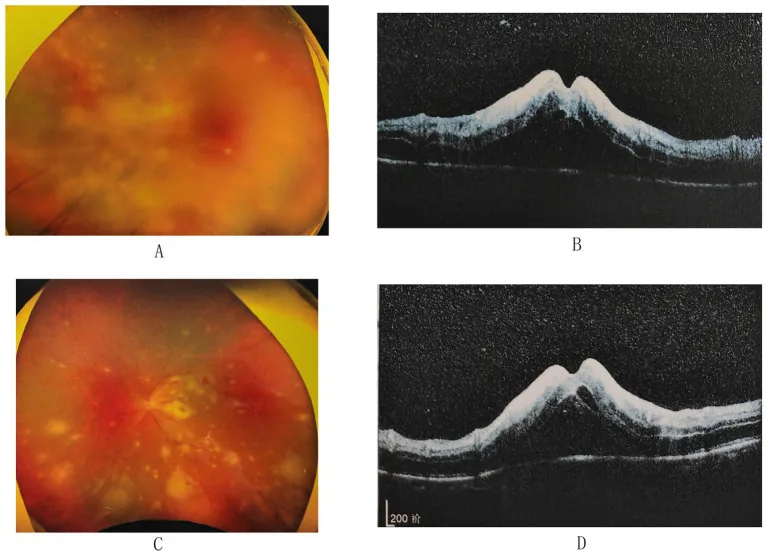
Zhu W, et al. Atypical presentation of acute retinal necrosis mimicking Vogt-Koyanagi-Harada disease leading to misdiagnosis: a case report. Front Med (Lausanne). 2024. Figure 2. PMCID: PMC11620890. License: CC BY.
Fundus photograph shows scattered yellowish-white necrotic retinal lesions, optic disc edema, retinal hemorrhages, and vascular sheathing. OCT reveals retinal thickening and intraretinal/subretinal fluid, indicating clinical findings of acute retinal necrosis.
Mutton-fat keratic precipitates (KP): Densely arranged in an orderly manner covering the entire corneal endothelium, or in an Arlt’s triangle pattern predominantly inferiorly. They become pigmented over time.
Anterior chamber inflammation: Inflammatory cells and flare are present. Anterior and posterior synechiae and iris atrophy are rare.
Elevated intraocular pressure: High and severe in HSV ARN (average around 35 mmHg). In VZV ARN, about half have high IOP (average around 25 mmHg). Even in cases without high IOP, an IOP difference of 6 mmHg or more compared to the unaffected fellow eye is often observed.
Fundus and Retinal Findings
Yellowish-white granular lesions in the peripheral retina: Appear in multiple locations, rapidly expanding circumferentially and posteriorly. Progression stops about one week after antiviral therapy, changing into confluent geographic white lesions.
Retinal arteritis: Vascular sheathing and occlusion. Characteristic club-shaped hemorrhages along veins.
Others: Optic dischyperemia and swelling, inflammatory vitreous opacities. Club-shaped hemorrhages along veins, scalloped edges, and Kyrieleis’ arteriolitis (yellowish-white lesions along arterioles) are also characteristic findings.
Fluorescein angiography reveals an occlusive arteritis pattern and optic disc hyperfluorescence. OCT shows choroidal thickening (pachychoroid) corresponding to the necrotizing retinitis lesions, as reported 18), and is noted as a new diagnostic finding.
The yellowish-white granular lesions (viral proliferation sites) in the peripheral retina extend circumferentially and toward the posterior pole, but their progression stops about one week after administration of antiviral drugs. Subsequently, the granular lesions coalesce into dense, well-demarcated geographic white lesions (a combination of direct viral damage and circulatory disturbance due to occlusive vasculitis).
Approximately one week after starting treatment, anterior chamber symptoms decrease and intraocular pressure normalizes, but anterior chamber inflammation may persist for years. About 3 to 4 weeks after onset, incomplete posterior vitreous detachment occurs due to vitreous organization, and strong vitreous traction on the extremely thinned and fragile necrotic retina leads to multiple tear formation. As a result, retinal detachment occurs in about 70% of cases.
Retinal detachment occurs in about 70% of cases, and ultimately two-thirds of eyes have visual acuity of 0.1 or less, making this a poor-prognosis disease. However, compared to the initially affected eye (first eye), the spread of lesions in the fellow eye (which develops in about 15% of cases) is limited, and the visual prognosis is considered relatively good.
ARN is caused by intraocular reactivation of herpes viruses. After primary infection, the virus remains latent in the trigeminal ganglion and dorsal root ganglia, and reactivates when the host’s immune balance changes, reaching the eye via nerve axons.
Current or past herpes infection: A history of shingles, even more than 30 years ago, can cause ARN due to VZV reactivation. A history of HSV encephalitis can also be a cause.
Topical steroids: Long-term use of topical ocular steroids can rarely be a trigger.
Advanced age: Associated with risk of ARN due to VZV.
Immunosuppressive drugs: Decreased CD8+ T cells and virus-specific T cell immunity are key to reactivation, and have been reported with the following drugs:
natalizumab (multiple sclerosis treatment): Inhibits leukocyte migration into the CNS, leading to decreased CD4/CD8 ratio13)
DMF (dimethyl fumarate): Decreased CD8+ T cell and VZV-specific T cell immunity14)
ICI (immune checkpoint inhibitors): VZV reactivation due to sintilimab12)
Cataract surgery: May trigger VZV reactivation as a physical trigger15)
COVID-19 infection: HSV reactivation due to CD3+ CD8+ T lymphopenia16)
Assumption of immunocompetence: If immunocompromised (HIV infection, immunosuppressant use), prioritize CMV retinitis and PORN.
The pathology involves not only direct viral cytopathy but also occlusive vasculitis and retinal ischemia caused by inflammatory cells recruited to eliminate the virus, which exacerbate tissue damage.5)
Positive for HSV-1, HSV-2, or VZV by intraocular fluid PCR or antibody ratio (Q value)
Definite diagnosis (virus-confirmed group): Initial ocular findings 1a and 1b present, plus at least one item from clinical course and positive virologic test.
Clinical diagnosis (virus-unconfirmed group): At least 4 items including initial ocular findings 1a and 1b, plus at least 2 items from clinical course.
These criteria were developed and validated by Takase et al. (2015). 4)
PCR of intraocular fluid (aqueous humor or vitreous) is the most sensitive and specific diagnostic method for virus identification. 1) Multiplex PCR (advanced medical care) can identify multiple viruses and is useful for differential diagnosis.
Antibody ratio (Q value: Goldmann-Witmer coefficient) is also used as an adjunctive diagnostic tool. However, within 10 days of onset, intraocular antibody production is insufficient, leading to false negatives; PCR is preferred during this period. Serum antibody titers alone cannot establish an etiologic diagnosis. 1)
Case reports with atypical findings such as exudative retinal detachment; broaden differential if presentation deviates from typical 19)
QDo you start treatment even if PCR is negative?
A
Yes. If clinical diagnostic criteria (virus-unconfirmed group) are met, antiviral therapy is started without waiting for PCR results. Within 10 days of onset, the false-negative rate of PCR is high, and because the disease progresses rapidly, it is standard to start treatment immediately if there is diagnostic certainty, following the ASAP principle.
Following the ASAP principle, and referring to domestic guidelines and reported treatment series, initiate four-pillar treatment as soon as possible. 1, 5, 6)
In addition to systemic administration, concomitant intravitreal injection of foscarnet (2.4 mg/0.1 mL) has been reported to improve visual outcomes and reduce the rate of retinal detachment. 7, 8) It should be considered especially in severe cases or when visual impact is imminent. 5)
Prevention of retinal detachment (surgical treatment)
Prophylactic barrier laser photocoagulation: This may be performed during the granular lesion stage on the posterior side of the necrotic lesion, but evidence for its effect in preventing retinal detachment is limited, and its efficacy is not established. 5) Coagulation is applied in 3 to 4 rows just posterior to the granular lesion, avoiding the lesion itself and the peripheral side.
Vitrectomy: Performed when retinal detachment occurs (approximately 70% of cases).
It is not mandatory. Barrier laser (photocoagulation posterior to the necrotic lesions) may be performed, but evidence that it reliably prevents retinal detachment is currently limited. Considering the fragility and traction of the necrotic area, vitrectomy with silicone oil tamponade is the definitive treatment if detachment occurs.
ARN is caused by herpes viruses (HSV-1, HSV-2, VZV) that latently infect the trigeminal ganglion or dorsal root ganglion and reactivate due to some trigger (immunosuppression, aging, stress, etc.), reaching the eye.
Direct viral cytopathology: Viral replication and cell lysis within retinal cells. The area of viral proliferation is observed macroscopically as yellowish-white granular lesions.
Ischemia due to occlusive vasculitis: Inflammatory cell infiltration to eliminate the virus causes vasculitis around the retinal arteries, leading to vascular occlusion and retinal ischemia. Edema and circulatory disturbances due to occlusive vasculitis form well-demarcated geographic white lesions.
The combination of these two mechanisms leads to rapid necrosis, thinning, and weakening of the retina. 5)
Three to four weeks after onset, the vitreous becomes organized and incomplete posterior vitreous detachment occurs. At this point, strong traction from the vitreous on the extremely thinned and weakened necrotic retina leads to the formation of multiple tears. Due to the combination of thinning of the necrotic area and traction, retinal detachment occurs in approximately 70% of cases.
HSV-1 ARN tends to occur in patients with a history or complication of herpes encephalitis, and may present as ocular symptoms following encephalitis.
HSV-2 ARN has been associated with meningitis, requiring particular attention in young patients.
VZV ARN has a higher degree of occlusive vasculitis and frequency of optic nerve involvement than HSV ARN, and is considered to have a worse prognosis.
The risk of fellow eye involvement is approximately 15%. The interval between onset in the right and left eyes is often within one month, but the spread of lesions in the second eye is limited, and visual prognosis is better than in the first eye.
Special mechanisms of ARN associated with immunosuppressive drugs and emerging infectious diseases
ICI (PD-1/PD-L1 inhibitor)-associated ARN: Immune-related adverse events (similar to IRIS mechanism), impaired self-tolerance, and loss of ocular immune privilege have been suggested. 12)
COVID-19-associated ARN: A marked decrease in CD3+ CD8+ T lymphocytes due to SARS-CoV-2 infection is thought to promote reactivation of latent HSV. 16)
Natalizumab-associated ARN: A decrease in the CD4/CD8 ratio due to inhibition of leukocyte migration into the CNS reduces virus-specific immunity. 13)
DMF (dimethyl fumarate)-associated ARN: Decreased CD8+ T cell and VZV-specific T cell immunity increases the risk of reactivation. 14)
7. Latest research and future perspectives (reports at the research stage)
Conventional standard treatment has been inpatient treatment with intravenous acyclovir, but case series have been reported in which active retinitis resolved with oral valacyclovir or famciclovir. 9) The AAO report also states that initial treatment with oral or intravenous antiviral drugs is effective, but intravenous infusion is often prioritized depending on the severity of the case and the patient’s general condition. 5)
A retrospective study of intravitreal foscarnet injection (2.4 mg/0.1 mL) combined with systemic therapy suggested that the addition of intravitreal injection may improve visual prognosis, especially in VZV ARN. 7) It may achieve high local concentrations while minimizing systemic toxicity, and standardization of induction therapy in severe cases is a research topic.
Quantitative PCR monitoring of viral load in intraocular fluid has been reported to be useful not only for diagnostic assistance but also for assessing treatment response. 10) However, challenges remain for incorporation into daily practice, such as the invasiveness of repeated sampling and standardization of measurement methods.
Potential of pachychoroid as a marker of ARN activity
Choroidal thickening (pachychoroid) on OCT has been reported as a finding reflecting the activity of acute retinal necrosis. In a case of secondary VZV-ARN, pachychoroid on OCT occurred coinciding with the area of necrotizing retinitis, suggesting its potential use as a marker of activity during follow-up after treatment. 18)
There is a report that foscarnet 4800 mg/day IV was effective in a case of EBV-ARN that was resistant to acyclovir and ganciclovir. 20) When the cause is a virus other than VZV or HSV, standard treatment may be less effective, and identification of the causative virus by PCR is important for determining the treatment strategy.
Association of immunosuppressive drugs and emerging infectious diseases with ARN
With the widespread use of immune checkpoint inhibitors (ICIs), attention to the risk of ARN due to VZV reactivation is required. 12) In addition, reports of ARN due to HSV/VZV reactivation after COVID-19 infection have been increasing, and ARN associated with immunosuppressive therapy may continue to increase in the future. 14)16)
Urayama A, Yamada N, Sasaki T, et al. Unilateral acute uveitis with periarteritis and retinal detachment. Jpn J Clin Ophthalmol. 1971;25:607-619.
Standardization of Uveitis Nomenclature (SUN) Working Group. Classification Criteria for Acute Retinal Necrosis Syndrome. Am J Ophthalmol. 2021;228:237-244. doi:10.1016/j.ajo.2021.03.057. PMID:33845012. PMCID:PMC8675365.
Takase H, Okada AA, Goto H, et al. Development and validation of new diagnostic criteria for acute retinal necrosis. Jpn J Ophthalmol. 2015;59(1):14-20. doi:10.1007/s10384-014-0362-0. PMID: 25492579.
Schoenberger SD, Kim SJ, Thorne JE, et al. Diagnosis and Treatment of Acute Retinal Necrosis: A Report by the American Academy of Ophthalmology. Ophthalmology. 2017;124(3):382-392. doi:10.1016/j.ophtha.2016.11.007. PMID: 28094044.
Tibbetts MD, Shah CP, Young LH, et al. Treatment of acute retinal necrosis. Ophthalmology. 2010;117(4):818-824. doi:10.1016/j.ophtha.2009.09.001. PMID: 20079537.
Wong R, Pavesio CE, Laidlaw DA, et al. Acute retinal necrosis: the effects of intravitreal foscarnet and virus type on outcome. Ophthalmology. 2010;117(3):556-560. doi:10.1016/j.ophtha.2009.08.003. PMID: 20031221.
Flaxel CJ, Yeh S, Lauer AK. Combination systemic and intravitreal antiviral therapy in the management of acute retinal necrosis syndrome. Ophthalmic Surg Lasers Imaging Retina. 2013;44(6):521-526.
Aizman A, Johnson MW, Elner SG. Treatment of acute retinal necrosis syndrome with oral antiviral medications. Ophthalmology. 2007;114(2):307-312. doi:10.1016/j.ophtha.2006.06.058. PMID: 17123607.
Asano S, Yoshikawa T, Kimura H, et al. Monitoring herpesvirus DNA in three cases of acute retinal necrosis by real-time PCR. J Clin Virol. 2004;29(3):206-209. PMID: 15002491.
Cochrane TF, Silvestri G, McDowell C, Foot B, McAvoy CE.. Acute retinal necrosis in the United Kingdom: results of a prospective surveillance study. Eye (Lond). 2012;26(3):370-7; quiz 378. doi:10.1038/eye.2011.338. PMID:22281865; PMCID:PMC3298997.
Wang P, An M, Zhang M, et al. Acute retinal necrosis in a patient with cervical malignant tumor treated with sintilimab: a case report and literature review. Front Immunol. 2024;15:1301329. doi:10.3389/fimmu.2024.1301329.
Cheraqpour K, Ahmadraji A, Rashidinia A, Irannejad M, Shahriari M.. Acute retinal necrosis caused by co-infection with multiple viruses in a natalizumab-treated patient: a case report and brief review of literature. BMC Ophthalmol. 2021;21(1):337. doi:10.1186/s12886-021-02096-x. PMID:34530769; PMCID:PMC8447524.
Luo T, Wang L, Zhang L, Hu MJ, Zhou SR, He XY, Yang JF.. Acute retinal necrosis following cataract surgery: a case of VZV reactivation and successful management. BMC Ophthalmol. 2025;25(1):131. doi:10.1186/s12886-025-03950-y. PMID:40087671; PMCID:PMC11907935.
Gonzalez MP, Rios R, Pappaterra M, Hernandez M, Toledo A, Santos C, Emanuelli A, Kurup SK, Oliver AL.. Reactivation of Acute Retinal Necrosis following SARS-CoV-2 Infection. Case Rep Ophthalmol Med. 2021;2021:7336488. doi:10.1155/2021/7336488. PMID:34336325; PMCID:PMC8313348.
Rahman EZ, Shah P, Shah R.. Metastatic squamous cell carcinoma masquerading as acute retinal necrosis. Am J Ophthalmol Case Rep. 2023;32:101934. doi:10.1016/j.ajoc.2023.101934. PMID:37869266; PMCID:PMC10585213.
Harbeck K, Ericksen C, Johnson W, Massop D, Bracha P.. Pachychoroid Associated With Acute Retinal Necrosis Secondary to Varicella Zoster Virus. J Vitreoretin Dis. 2024;8(2):196-199. doi:10.1177/24741264241228652. PMID:38465350; PMCID:PMC10924601.
Perhiar BA, Siddiqui MR, Ibrahim S.. Acute retinal necrosis with exudative retinal detachment in a child. BMJ Case Rep. 2021;14(12):e245984. doi:10.1136/bcr-2021-245984. PMID:34911728; PMCID:PMC8679069.
Suzuki K, Namba K, Hase K, Mizuuchi K, Iwata D, Ito T, Kitaichi N, Takase H, Ishida S.. A case of Epstein-Barr virus acute retinal necrosis successfully treated with foscarnet. Am J Ophthalmol Case Rep. 2022;25:101363. doi:10.1016/j.ajoc.2022.101363. PMID:35146210; PMCID:PMC8818534.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.