Retinal tears, retinal holes, and lattice degeneration are peripheral retinal lesions that are closely involved in the development of rhegmatogenous retinal detachment (RRD).
Lattice degeneration is a well-defined oval to band-shaped degenerative lesion in the peripheral retina, from the equator to the posterior border of the vitreous base, arranged parallel to the ora serrata. Inside, blood vessels become white-lined and appear lattice-like (hence the name). Within the lesion, neuronal degeneration and localized retinal thinning with internal limiting membrane defects occur, and the overlying vitreous liquefies. Firm vitreoretinal adhesions form at the margins.
Retinal tear is a full-thickness break in the sensory retina. It occurs due to vitreous traction at sites of vitreoretinal adhesion, often resulting from lattice degeneration. It frequently follows posterior vitreous detachment (age-related change).
Retinal hole is a full-thickness defect of the neurosensory retina, caused by retinal atrophy. It most commonly occurs within lattice degeneration. Atrophic hole is a hole without a flap (operculum) formed by chronic retinal atrophy within lattice degeneration, without vitreous traction. Since traction may be applied to the degeneration itself, holes within lattice degeneration may require management similar to retinal tears depending on the situation.
The prevalence of lattice degeneration is reported to be 6–10% of the general population1)6). Some autopsy studies report up to 10.7%6). It reaches maximum frequency by age 20, with little difference between races or sexes. The most common location is the inferotemporal quadrant, and the nasal quadrant is the least frequent.
The annual incidence of RRD is 10–18 per 100,000 people7). Lattice degeneration is found in 20–40% of RRD patients1)6), but only 0.3–0.7% of eyes with lattice degeneration actually develop RRD8). In a long-term study of 423 eyes followed for an average of about 11 years, only 3 eyes (0.7%) developed clinical RRD6). About 20–35% of lattice degeneration is associated with atrophic holes, but progression to retinal detachment is even more limited2). A large registry study reported that the incidence of RRD after cataract surgery is 0.21% (about 1 in 500) within the first year postoperatively11).
When associated with traumatic tears, progression is rapid: RRD occurs in 12% immediately after injury, 30% within 1 month, 50% within 8 months, and 80% within 24 months.
QDoes lattice degeneration always lead to retinal detachment?
A
The probability of developing retinal detachment from lattice degeneration is very low, at 0.3–0.7%. Most lesions are stable and remain asymptomatic. However, if risk factors such as a history of retinal detachment in the fellow eye or high myopia are present, regular follow-up is important.
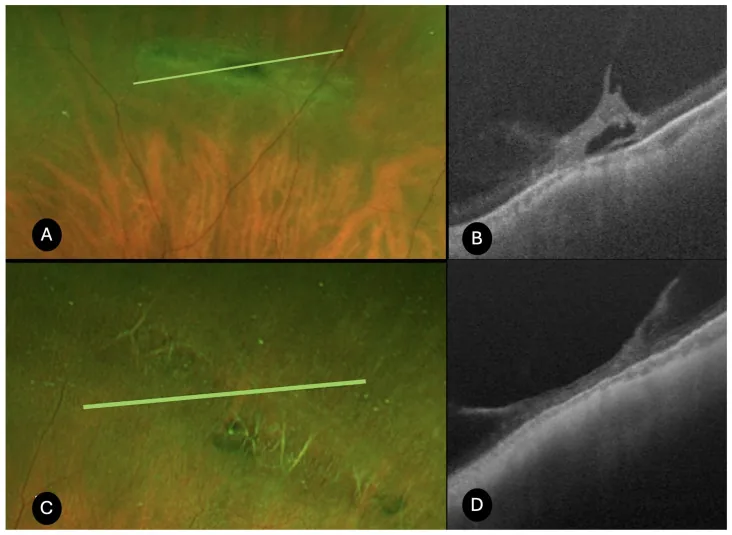
Bacherini D, et al. Characterization of Peripheral Retinal Degenerations and Rhegmatogenous Lesions Using Ultra-Widefield Swept Source OCT Integrated with a Novel Scanning Laser Ophthalmoscope. Diagnostics (Basel). 2025. Figure 1. PMCID: PMC12650825. License: CC BY.
Fundus images (A, C) and SS-OCT images showing vitreous traction, hyperreflective deposits, localized subretinal fluid (B), and extensive vitreous traction with choroidal thinning (D). Corresponds to lattice degeneration discussed in section “2. Main Symptoms and Clinical Findings”.
Lattice degeneration alone or with atrophic holes is mostly asymptomatic. When symptoms appear, they are often due to complications (tears, retinal detachment).
Photopsia: Occurs before tear formation when traction is applied at the vitreoretinal adhesion site. It intensifies in dark environments and is often noticed even with eyes closed. It may also be induced by eye movements.
In acute PVD, “seeing a black round object” (due to glial ring at the optic disc)
When a retinal tear causes vascular disruption, “seeing many small black objects”
Described in various forms such as cobwebs, veils, bugs, rings, dots, etc.
Visual field defect: When retinal detachment occurs, the defect appears on the opposite side of the detachment. Often described as “a curtain coming down”.
Visual acuity loss: Occurs with retinal detachment involving the macula.
Approximately 15% of patients who experience posterior vitreous detachment develop retinal tears 1). In acute PVD with vitreous hemorrhage, 70% have retinal tears, whereas without vitreous hemorrhage, only 2-4% develop tears 13). The rate of retinal tears in symptomatic PVD is 8.2%, and 21.7% in meta-analysis. Delayed tears missed at initial examination occur in 1.8%, and most were accompanied by vitreous hemorrhage, retinal hemorrhage, or new symptoms 12).
Shape: U-shaped or triangular full-thickness defect. The flap remains attached to the posterior vitreous membrane and is turned over.
Wet edge: The edge of the tear is elevated and appears white (indicator of active traction).
Shaffer’s sign: Pigment cells derived from the RPE float in the anterior vitreous (predictor of about 90% of tears)1)
Weiss ring: A ring-shaped opacity formed by the detachment of the vitreous attachment around the optic disc1)
Common location: Superotemporal quadrant in 60%; 50s (after PVD)
Atrophic Hole
Shape: Round or oval. Lacks a flap (no cover).
Pigmentation: Chronic cases may have pigmentation around the lesion.
Buried: May be hidden within lattice degeneration; careful not to overlook.
Asymptomatic: Most are asymptomatic; discovered incidentally during routine fundus examination.
Lattice Degeneration
Localized retinal thinning: Well-demarcated oval to linear lesion; vitreous over the degeneration is liquefied.
White sheathing of vessels: Retinal vessels crossing the degeneration appear white (origin of lattice pattern).
Associated atrophic holes: About 20-35% of lattice degeneration have atrophic holes2)
Snail-track degeneration: A subtype seen in young individuals; white frost-like changes.
QShould I see a doctor immediately if I have floaters?
A
Approximately 15% of patients who experience posterior vitreous detachment develop retinal tears. Sudden increase in floaters, photopsia (flashes of light), or visual field defects are warning signs of a retinal tear or detachment. If these symptoms occur, it is strongly recommended to promptly visit an ophthalmologist for a dilated fundus examination.
Posterior vitreous detachment (PVD): The main cause of flap tears. With aging, vitreous collagen fibers aggregate and liquefy, causing the vitreous cortex to detach from the inner surface of the retina15). The retina is pulled at the strong adhesion site at the posterior border of the vitreous base 1).
Chronic retinal atrophy: Cause of atrophic holes. In lattice degeneration, progressive neuronal degeneration leads to extreme thinning and hole formation.
Mechanism of lattice degeneration: The cause is unknown, but several hypotheses exist, including abnormal development of the internal limiting membrane and local ischemia.
Traumatic mechanism: Blunt ocular trauma often causes tears in the inferotemporal equatorial region. Direct or indirect forces concentrate at the vitreoretinal adhesion sites, leading to tear formation.
Increased traction due to ciliary muscle contraction3)
Traumatic retinal break
80% progress to RRD within 24 months
In traumatic retinal breaks, the time course from injury to onset of retinal detachment is rapid. RRD occurs in 12% immediately after injury, 30% within 1 month, 50% within 8 months, and 80% within 24 months. It may be associated with posterior pole breaks, ora serrata tears, and ciliary epithelial breaks, and is often accompanied by vitreous hemorrhage or angle recession. A 360-degree examination under dilated pupils is essential for full circumferential evaluation.
QAre people with myopia more prone to retinal tears?
A
Myopia (over -3D) increases the risk of rhegmatogenous retinal detachment by about 10 times, and low myopia (1-3D) increases the risk by 4 times. In myopic eyes, axial elongation often accompanies lattice degeneration, further increasing the risk. Regular dilated fundus examination screening is important.
Dilated 360-degree fundus examination: Binocular indirect ophthalmoscopy with scleral depression is most useful. Most retinal tears and holes occur anterior to the equator, making them difficult to diagnose with fundus cameras.
Slit-lamp biomicroscopy (three-mirror lens, wide-field indirect lens): Evaluate horseshoe tears, opercula, traction, bridging vessels, and the extent of surrounding detachment three-dimensionally. Ideally, examine the patient in a supine position for full circumferential observation.
Check for Shaffer’s sign: RPE-derived pigment cells (tobacco dust) in the anterior vitreous are about 90% predictive of a tear 1).
Search for multiple tears: There is a 75% probability that multiple tears exist within the same 90-degree quadrant, so even if one is found, examine the entire retina1).
In slit-lamp observation, for tears at the edge of lattice degeneration, design the coagulation area to surround not only the tear but the entire lattice degeneration. For isolated tears, coagulation around the tear alone is sufficient. Placing the patient in a supine position avoids difficulty in stereoscopic viewing of the nasal and temporal sides and improves the accuracy of full circumferential observation.
OCT: Evaluation of posterior vitreous detachment and macular lesions1); peripheral OCT detects retinal thinning 92%, vitreoretinal adhesion 72%, retinoschisis 44%, and retinal tear with subretinal fluid 4%2)
Ultra-widefield fundus photography (UWF): Useful for screening; sensitivity 65–89%2)
Retromode scanning laser ophthalmoscopy (SLO): Detects 31–55% more peripheral findings than conventional methods2)
Ultra-widefield swept-source OCT (including integrated devices such as IIVO): Enables simultaneous evaluation of peripheral retinal degeneration and rhegmatogenous lesions, improving diagnostic accuracy2)
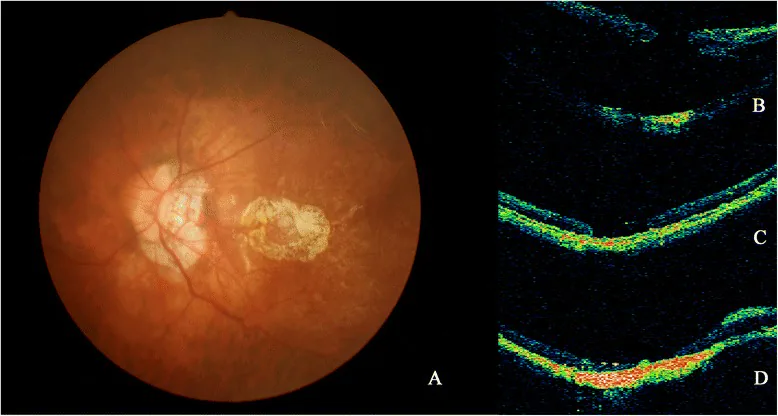
Nan Hong; Bai-shuang Huang; Jian-ping Tong. Primary silicone oil tamponade and internal limiting membrane peeling for retinal detachment due to macular hole in highly myopic eyes with chorioretinal atrophy. BMC Ophthalmol. 2015 Nov 11; 15:165 Figure 2. PMCID: PMC4642637. License: CC BY.
Fundus photograph and OCT images (a, b, c and d) from Patient 20. a PCA around MH was shown on fundus photograph. b RD caused by MH developed. c After the SO removal, retinal reattachment was achieved, MH was still open on OCT. d After the second silicone oil removal, the patient achieved retina reattachment despite persistent open of the MH
Differential diagnoses include cystoid degeneration, paving stone degeneration, and white without pressure. Paving stone degeneration is due to choroidal capillary insufficiency and does not cause vitreous liquefaction or holes/tears. White without pressure presents as a whitish change without scleral indentation and may need differentiation from lattice degeneration. Cystoid degeneration is cavitation of the inner nuclear layer and is a different mechanism from hole formation.
QWhat tests can detect retinal tears?
A
The basic examination is dilated 360-degree fundus examination (binocular indirect ophthalmoscopy with scleral indentation). Checking for Shaffer’s sign (pigment cells in the anterior vitreous) is also an important clue. In cases with vitreous hemorrhage, B-scan ultrasound is useful, and OCT can provide detailed evaluation of the tear. If one tear is found, examine the entire retina to avoid missing multiple tears.
For typical lattice degeneration alone, prophylactic coagulation is not necessary (even if performed, the incidence of retinal detachment does not change). Prophylactic treatment is considered when one or more of the following risk factors are present1).
For confirmed Stickler syndrome, 360-degree prophylactic laser photocoagulation is recommended1). There are currently no randomized controlled trials (RCTs) evaluating the efficacy of prophylactic photocoagulation, and the Cochrane systematic review (2014) also confirmed no RCT evidence14).
Laser photocoagulation can reduce the risk of retinal detachment to less than 5%, but it cannot be completely prevented 1). The most common cause of treatment failure is insufficient coagulation at the anterior margin of the tear, and it is important to ensure that the coagulation range extends to the ora serrata. Even after laser coagulation, if vitreous traction becomes strong, retinal detachment can occur beyond the scar. As posterior vitreous detachment progresses, new tears may also form.
For clinical RRD, the primary reattachment rate with vitrectomy or scleral buckling is over 90%, and including multiple surgeries, it reaches 98% 1). A Cochrane systematic review found no significant difference in anatomical or visual outcomes between the two procedures 1).
Symptomatic PVD (no tear, with vitreous/retinal hemorrhage)
1–2 weeks later 1)
After treatment of symptomatic horseshoe tear
1–2 weeks → 4–6 weeks → 3–6 months → annually 1)
Asymptomatic atrophic hole
Every 1–2 years 1)
Asymptomatic lattice degeneration
Annually 1)
Lattice degeneration/atrophic hole in fellow eye with history of RRD
Every 6–12 months1)
If vitreous hemorrhage prevents photocoagulation, follow with ultrasound and observe for 2–3 months. If detachment progresses or hemorrhage does not absorb, consider vitrectomy.
Prompt treatment can reduce the risk of rhegmatogenous retinal detachment to less than 5%, but cannot completely prevent it. The most common cause of treatment failure is inadequate coagulation at the anterior border of the tear; thorough laser application is important. Regular follow-up with dilated fundus examination is necessary even after treatment.
With aging, vitreous collagen fibers aggregate and form lacunae15). Posterior vitreous detachment (PVD) occurs when the vitreous cortex separates from the inner retina; firm adhesions, especially at the posterior border of the vitreous base (2–3 mm posterior to the ora serrata), are involved in tear formation1).
PVD is classified into the following stages (equivalent to AAO PPP Table 1)1)15):
Stage 1: Separation at the parafovea; vitreous attachment remains at the fovea
Stage 2: Complete separation from the fovea
Stage 3: Extensive vitreous separation; residual attachment at the optic disc
Stage 4: Complete PVD (complete separation also from around the optic disc)
During posterior vitreous detachment, the vitreous attached to the posterior border of the vitreous base is strongly pulled 1). The neurosensory retina is torn, forming a horseshoe tear. The apex of the flap remains attached to the posterior vitreous membrane and flips forward, while only the base remains on the retina. If traction persists, the base of the flap may be torn off, converting it into an operculated hole (reducing RRD risk with release of traction).
Thinning of the neurosensory retina (focal degeneration with internal limiting membrane defect)
Vitreous liquefaction directly over the degeneration (dome-shaped liquefaction cavity)
Strong vitreoretinal adhesion at the margin (U-shaped pattern) 2)
Electron microscopy reveals vascular fibrosis (white sheathing), accumulation of glial material, pigment changes, absence of basement membrane and replacement by glial cells. Capillaries within the degeneration are occluded.
Furthermore, choroidal thinning and rarefaction of choriocapillaris in the central area of degeneration, and dome-shaped scleral indentation directly beneath the degeneration have been reported 2), and an association with COL2A1 gene mutation has also been suggested 2).
In lattice degeneration, neuronal degeneration and internal limiting membrane defect occur, leading to progressive focal retinal thinning. As vitreous liquefaction over the degeneration progresses, the inner retinal layers disappear, and an atrophic hole without a lid forms at the site of extreme thinning.
Via atrophic hole: Liquefied vitreous flows into the subretinal space through the hole → localized shallow detachment; unlikely to expand without PVD. Over a long course, a demarcation line may form, and progression may stop spontaneously. Accounts for 2.8–13.9% of all retinal detachments.
Via tractional tear: During PVD, a horseshoe tear forms at the edge of a degenerative lesion → liquefied vitreous rapidly flows into the subretinal space → tall bullous retinal detachment. Progression is rapid, with high risk of macular detachment. Accounts for 16–18% of all retinal detachments.
Complications and prognosis after untreated or treated retinal tears
Regarding pilocarpine 1.25% (Vuity), approved by the FDA in 2021 for presbyopia, retinal tears and retinal detachment have been reported in 6 eyes post-approval. A case report by Eaddy et al. describes a patient who developed a horseshoe tear within 10 minutes of using Vuity, emphasizing the importance of dilated fundus screening before prescription and patient education 3). Miotics may increase traction on the vitreous base via ciliary muscle contraction. Postoperative visual acuity was reported to recover to 20/15-1 3).
Macular horseshoe tear is a rare condition, but vitrectomy, flap removal, and short-term gas tamponade may yield good results. In a case report by Manoli et al., a macular horseshoe tear associated with chronic cystoid macular edema (CME) was treated with 25G vitrectomy, flap removal, and 20% SF6 tamponade, achieving tear closure and stable vision at 6 months 4). SF6 is absorbed more quickly than C2F6 or C3F8, offering an advantage for early visual recovery.
Scleral perforation from periocular cosmetic filler injection can cause large tears and retinal detachment. Sasongko et al. reported a case of a large stellate retinal tear after periocular filler injection, highlighting the risk of ocular complications associated with cosmetic procedures 5).
Automated Diagnosis Using Artificial Intelligence (AI)
Automated detection of lattice degeneration using deep learning models has reported high diagnostic accuracy with an AUROC of 0.999, sensitivity of 98.7%, and specificity of 99.2%2). The improved YOLOX model achieved a detection accuracy of 96.0%, sensitivity of 82.7%, and specificity of 96.7%2). Future applications are expected in automated screening from wide-angle fundus photographs.
Combining OCT and OCTA has clarified choroidal circulatory abnormalities in lattice degeneration, contributing to the elucidation of disease mechanisms2). Ultra-widefield swept-source OCT enables simultaneous acquisition of ultra-widefield fundus photography and OCT, improving the accuracy of evaluating peripheral lesions2).
COL9A3 gene mutations have been reported to be associated with severe peripheral vitreoretinal degeneration and RRD2), and identifying high-risk groups for RRD with hereditary connective tissue disorders is a future challenge.
Selection of Prophylactic Treatment for the Fellow Eye
Curran et al. examined the outcomes of prophylactic coagulation for lattice degeneration in the fellow eye in cases of unilateral uncomplicated RRD. At 5-year follow-up, new retinal tears or RRD occurred in 17% of the prophylactic treatment group and 41% of the untreated group, suggesting the usefulness of prophylactic intervention in high-risk eyes16). However, this is not an RCT, and caution is needed in interpretation given the lack of evidence from the aforementioned Cochrane 2014 review.
Kim SJ, Bailey ST, Kovach JL, Lim JI, Vemulakonda GA, Ying GS, et al. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P163-P196. doi:10.1016/j.ophtha.2024.12.023. PMID:39918519.
Maltsev DS, Kulikov AN, Shaimova VA, Burnasheva MA, Vasiliev AS. Spotlight on Lattice Degeneration Imaging Techniques. Clinical ophthalmology (Auckland, N.Z.). 2023;17:2383-2395. doi:10.2147/OPTH.S405200. PMID:37605766; PMCID:PMC10440085.
Eaddy IC, Moushmoush O, Sabbagh O, Barazi MD, Sabbagh O.. Horseshoe Retinal Tear Minutes After Use of a New Pilocarpine Formulation in a Presbyopic, Emmetropic Man. J Vitreoretin Dis. 2025;9(1):105-108. doi:10.1177/24741264241255589. PMID:39554627; PMCID:PMC11562214.
Sasongko MB, Wan R, Ho IV. Large, star-shaped retinal tear associated with orbital cosmetic filler. American journal of ophthalmology case reports. 2022;25:101342. doi:10.1016/j.ajoc.2022.101342. PMID:35243133; PMCID:PMC8859732.
Byer NE. Long-term natural history of lattice degeneration of the retina. Ophthalmology. 1989;96(9):1396-401; discussion 1401-2. doi:10.1016/s0161-6420(89)32713-8. PMID:2780007.
Haimann MH, Burton TC, Brown CK. Epidemiology of retinal detachment. Archives of ophthalmology (Chicago, Ill. : 1960). 1982;100(2):289-92. doi:10.1001/archopht.1982.01030030291012. PMID:7065947.
Byer NE. Subclinical retinal detachment resulting from asymptomatic retinal breaks: prognosis for progression and regression. Ophthalmology. 2001;108(8):1499-1503; discussion 1503-1504. PMID: 11470709. doi:10.1016/S0161-6420(01)00652-2.
The Eye Disease Case-Control Study Group. Risk factors for idiopathic rhegmatogenous retinal detachment. Am J Epidemiol. 1993;137(7):749-757. doi:10.1093/oxfordjournals.aje.a116735.
N Byer. What happens to untreated asymptomatic retinal breaks, and are they affected by posterior vitreous detachment?. Ophthalmology. 1998;105(6):1045-1050. doi:10.1016/s0161-6420(98)96006-7.
Morano MJ, Khan MA, Zhang Q, Halfpenny CP, Wisner DM, Sharpe J, Li A, Tomaiuolo M, et al. Incidence and Risk Factors for Retinal Detachment and Retinal Tear after Cataract Surgery: IRIS® Registry (Intelligent Research in Sight) Analysis. Ophthalmology science. 2023;3(4):100314. doi:10.1016/j.xops.2023.100314. PMID:37274012; PMCID:PMC10239011.
Coffee RE, Westfall AC, Davis GH, Mieler WF, Holz ER.. Symptomatic posterior vitreous detachment and the incidence of delayed retinal breaks: case series and meta-analysis. Am J Ophthalmol. 2007;144(3):409-413. doi:10.1016/j.ajo.2007.05.002. PMID:17583667.
Michael I. Seider, Carol Conell, Ronald B. Melles. Complications of Acute Posterior Vitreous Detachment. Ophthalmology. 2022;129(1):67-72. doi:10.1016/j.ophtha.2021.07.020.
Wilkinson CP. Interventions for asymptomatic retinal breaks and lattice degeneration for preventing retinal detachment. The Cochrane database of systematic reviews. 2014;2014(9):CD003170. doi:10.1002/14651858.CD003170.pub4. PMID:25191970; PMCID:PMC4423540.
Johnson MW. Posterior vitreous detachment: evolution and role in macular disease. Retina. 2012;32 Suppl 2:S174-S178. doi:10.1097/IAE.0b013e31825bef62.
Curran CD, Adams OE, Vagaggini T, Sodhi GS, Prairie ML, Baker MJ, Sastry A, Ryan EH, Parke DW, Mittra RA, Dev S, Tang PH.. PROPHYLACTIC TREATMENT OF LATTICE DEGENERATION IN FELLOW EYES AFTER REPAIR OF UNCOMPLICATED PRIMARY RHEGMATOGENOUS RETINAL DETACHMENT. Retina. 2024;44(1):63-70. doi:10.1097/iae.0000000000003908. PMID:37536462.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.