Angle recession is a condition in which a tear occurs between the circular (Müller’s) and longitudinal (Brücke’s) muscles of the ciliary body, causing the ciliary body to move posteriorly along with the iris. It is also called angle dissociation.
Angle recession occurs as a complication of blunt ocular trauma. Many patients with blunt trauma accompanied by hyphema have angle recession, and the incidence increases with the severity of trauma. Rather than causing immediate problems, it is often recognized only years later when glaucoma develops.
Angle recession
Site of tear: Between the circular (Müller’s) and longitudinal (Brücke’s) muscles of the ciliary body
Features: The ciliary body moves posteriorly, making the angle appear widened.
Complications: Late-onset intraocular pressure elevation due to trabecular meshwork dysfunction (angle-recession glaucoma).
Cyclodialysis
Site of tear: Attachment between the ciliary body and sclera
Features: The ciliary body detaches from the sclera, creating a communication between the angle and the suprachoroidal space.
Complications: Marked hypotony, hypotony maculopathy. Causes more severe hypotony than angle recession.
QDoes angle recession require treatment?
A
No specific treatment is needed for angle recession itself. However, treatment for associated hyphema and hypotony, as well as long-term follow-up to monitor for future glaucoma development, is necessary. It is important to explain the possibility of increased intraocular pressure to the patient and ensure regular follow-up visits.
Angle recession itself does not cause any subjective symptoms. Symptoms vary depending on the type and severity of associated injuries.
When associated with hyphema: Decreased vision, redness, eye pain. The impact on vision varies with the extent of hyphema.
When associated with hypotony: Extreme hypotony can cause decreased vision due to hypotony maculopathy. In addition to decreased vision, choroidal folds and optic disc edema may occur.
When angle recession glaucoma develops: Glaucomatous visual field defects due to elevated intraocular pressure occur. Often asymptomatic until advanced.
Clinical Findings (Findings Confirmed by Physician Examination)
Intraocular pressure: often temporarily elevated due to hyphema. Even if normal in the chronic phase, there is a risk of future increase.
QWhat should be done while hyphema is present?
A
The basic approach is to maintain rest and sleep with the head elevated. Because of the risk of rebleeding, gonioscopy should be avoided while hyphema is present. Also avoid medications that promote bleeding, such as aspirin. If intraocular pressure is high, manage with eye drops.
Angle recession is caused by a sudden increase in anterior chamber pressure due to blunt trauma. When external force is applied to the eye, the intraocular pressure rises momentarily, causing a tear between the ciliary muscle layers at the angle, which is under the greatest stress.
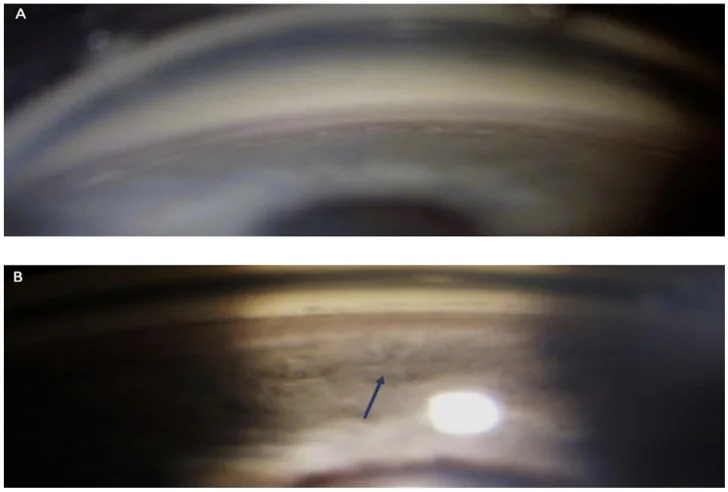
Iannucci V, Manni P, Alisi L, Mecarelli G, Lambiase A, Bruscolini A. Bilateral Angle Recession and Chronic Post-Traumatic Glaucoma: A Review of the Literature and a Case Report. Life (Basel). 2023;13(9):1814. Figure 1. PMCID: PMC10532958. DOI: 10.3390/life13091814. License: CC BY 4.0.
Comparative images of the right eye by gonioscopy. The superior angle (A) shows normal angle structures, whereas the inferior angle (B) demonstrates marked widening and recession (pathological deepening) of the ciliary band as indicated by the arrow, directly confirming posterior displacement of the ciliary body due to a tear between the longitudinal and circular muscles. This corresponds to the gonioscopic findings (widening of the ciliary band and asymmetry with the fellow eye) discussed in the section “Diagnosis and Examination Methods.”
Gonioscopy is essential for the definitive diagnosis of angle recession. When hyphema is present after ocular trauma, the possibility of angle recession should always be considered.
Characteristic findings include an increased distance from the iris root to the scleral spur and a wide gray band of the ciliary body. Comparison with the fellow eye (uninjured eye) is important for accurately assessing the extent and severity of angle recession.
Gonioscopy should be avoided while hyphema is present due to the risk of rebleeding.
Ultrasound biomicroscopy (UBM): Useful for observing from the iris root to the ciliary body. Can be performed even with hyphema, suitable for assessing the extent of angle recession and detecting concurrent cyclodialysis.
Anterior segment OCT: Allows non-contact evaluation of angle structures. Simpler than UBM and less burdensome for the patient.
Cyclodialysis: A condition where the ciliary body is detached from the sclera. It causes more pronounced hypotony than angle recession. It may occur when the trauma is severe.
Primary open-angle glaucoma: Angle-recession glaucoma that develops several years after injury resembles primary open-angle glaucoma clinically. Taking a history of trauma and comparing the angle morphology of both eyes are important for differentiation.
Iridodialysis: A condition where the iris root is detached from the sclera. It is observed as a deformation of the pupil.
Rest: Bed rest with the head elevated. Avoid strenuous activity to prevent rebleeding.
Mydriatics: Relaxation of the ciliary muscle to reduce pain and immobilize the iris.
Topical corticosteroids: To suppress inflammation and promote absorption of blood.
Intraocular pressure management: For elevated IOP due to bleeding, use topical medications such as beta-blockers and carbonic anhydrase inhibitors (CAIs).
It can develop several years to decades after injury. The risk is higher with a wider extent of angle recession (especially ≥180°). After the initial post-injury hypotony resolves, elevated intraocular pressure may occur years later. Regular measurement of intraocular pressure, visual field testing, and fundus examination are important for early detection.
When blunt external force is applied to the eye, intraocular pressure rises rapidly. This pressure causes the corneal limbus to stretch, and the aqueous humor moves posteriorly and into the angle, stretching the iris. This series of physical changes causes damage to the iris root.
The ciliary muscle consists of three layers: the circular muscle (Müller’s muscle), the longitudinal muscle (Brücke’s muscle), and the radial muscle. The rapid pressure change from blunt force causes a tear between the anatomically vulnerable circular and longitudinal muscles. This tear is the essence of angle recession.
At the moment of trauma, the trabecular meshwork sustains physical damage. This damage impairs aqueous humor outflow, leading to elevated intraocular pressure. It often does not manifest immediately after injury, but develops after a latent period of several years to decades as the functional reserve of the trabecular meshwork declines.
The following specific mechanisms are considered:
Direct trabecular meshwork damage at the time of trauma: The pressure change at injury physically damages the trabecular meshwork.
Post-inflammatory fibrosis: Inflammation following hyphema or traumatic uveitis promotes fibrosis and scarring of the trabecular meshwork.
Age-related changes: Normal aging combined with reduced trabecular reserve due to trauma leads to decompensation.
When cyclodialysis is present, the pathophysiology differs. If the ciliary body detaches from the sclera, the angle communicates with the suprachoroidal space, and aqueous humor flows massively into the suprachoroidal space. This results in marked hypotony and hypotony maculopathy. If the cyclodialysis closes spontaneously or with treatment, a sudden rise in intraocular pressure may occur.
QWhat is the difference between angle recession and cyclodialysis?
A
Angle recession is a tear between the circular and longitudinal muscles of the ciliary body, resulting only in a change in the position of the ciliary body. Cyclodialysis is a detachment of the ciliary body from the sclera, creating a communication between the angle and the suprachoroidal space. Cyclodialysis causes more pronounced hypotony and greater impact on vision. In cases of severe trauma, both conditions may coexist.
Quantitative evaluation methods for angle recession using anterior segment OCT and UBM are advancing. Research is underway to objectively quantify the extent and depth of angle recession and use them as predictive factors for glaucoma development risk. 2)
Long-term risk of developing angle recession glaucoma and predictive factors
Studies tracking the long-term incidence of glaucoma in cases with angle recession of 180° or more have shown that the risk of developing glaucoma 5 to 10 years after injury is significantly higher compared to normal eyes. The extent of angle recession and the degree of trabecular meshwork damage are being investigated as potential independent predictors of glaucoma development. 1)
Indications for MIGS (Minimally Invasive Glaucoma Surgery)
The application of minimally invasive glaucoma surgery (MIGS) to angle recession glaucoma is being studied. In angle recession glaucoma where the trabecular meshwork is damaged, the effectiveness of MIGS targeting the trabecular meshwork may be limited, and approaches that create bypass pathways to the suprachoroidal space or subconjunctival space are being evaluated.
Girkin CA, McGwin G Jr, Long C, Morris R, Kuhn F. Glaucoma after ocular contusion: a cohort study of the United States Eye Injury Registry. Journal of glaucoma. 2005;14(6):470-3. doi:10.1097/01.ijg.0000185437.92803.d7. PMID:16276279.
Sihota R, Kumar S, Gupta V, Dada T, Kashyap S, Insan R, Srinivasan G.. Early predictors of traumatic glaucoma after closed globe injury: trabecular pigmentation, widened angle recess, and higher baseline intraocular pressure. Arch Ophthalmol. 2008;126(7):921-926. doi:10.1001/archopht.126.7.921. PMID:18625937.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.