Primary open-angle glaucoma (POAG) is a chronic, progressive, irreversible optic nerve disease1). It causes visual field defects due to loss of the optic disc rim and retinal nerve fiber layer (RNFL)1)3). The anterior chamber angle is open and appears normal3). It is usually bilateral but often asymmetric3). Major risk factors are elevated intraocular pressure and aging1). With early diagnosis and treatment, visual impairment can often be prevented1)3).
In the 5th edition of the Japanese Glaucoma Guideline, primary open-angle glaucoma (broad definition) is defined as a disease concept that encompasses both primary open-angle glaucoma (narrow definition), in which conventional intraocular pressure is higher than the normal range, and normal-tension glaucoma (NTG)9). In clinical practice, it is conveniently divided into a high-tension group (narrow POAG) and a normal-tension group (NTG)9).
According to the Tajimi Study, when normal intraocular pressure in Japanese is defined as mean ± 2 standard deviations, the upper limit of normal is 19.9–20.0 mmHg, and it is considered reasonable to use 20 mmHg as the cutoff in daily practice 9)11). The European Glaucoma Society (EGS) guidelines refer to these as POAG/HTG (high-tension glaucoma) and POAG/NTG1)2). Both are part of a continuous disease spectrum, and the treatment strategy is essentially the same.
As of 2020, the number of POAG patients worldwide is estimated at approximately 53 million 3). The prevalence among people aged 40–80 is 3.0%. In Europe, 2.99% (12.3 million) of the population aged 40 and older have glaucoma, and more than half (56.4%) are estimated to be undiagnosed 2)3). There are significant differences in prevalence among races and ethnic groups. African Americans have a prevalence about three times that of Caucasians, making it a leading cause of irreversible blindness 3). Even higher prevalence has been reported in African-Caribbean populations 3). The prevalence in Hispanics is similar to that in African populations, and some reports indicate that the prevalence in Asian Americans is also higher than in Caucasians 3).
In the Tajimi Study, the total prevalence of glaucoma in individuals aged 40 years or older was 5.0%, with the majority being open-angle glaucoma11). The Kumejima Study showed regional differences, with a higher frequency of angle-closure glaucoma than the Tajimi Study12). Approximately 90% of POAG (broad sense) corresponds to NTG, and about 70% of all glaucoma is normal-tension glaucoma. In the Baltimore Eye Survey, the proportion of individuals with POAG at an intraocular pressure of 30 mmHg was about 7% in Caucasians and 25% in African Americans, demonstrating the limitations of using a specific intraocular pressure cutoff for screening3).
QWhat is the difference between primary open-angle glaucoma and normal-tension glaucoma?
A
Both belong to the same continuous disease group of primary open-angle glaucoma (broad sense). According to the 5th edition of the Glaucoma Clinical Practice Guidelines, an intraocular pressure of 20 mmHg is used as the cutoff; those exceeding this are classified as POAG (narrow sense), and those consistently within the normal range are classified as NTG. The European Glaucoma Society uses the terms POAG/HTG and POAG/NTG. Intraocular pressure has diurnal and seasonal variations, and repeated measurements or diurnal variation measurements are necessary for differentiation. In NTG, optic disc hemorrhages are more frequent, and paracentral scotomas are more common. The treatment strategy is the same, and the only evidence-based treatment is lowering intraocular pressure. In the Tajimi Study, 3.6% of the 3.9% with POAG (broad sense) were NTG, making Japan one of the countries with the highest prevalence of normal-tension glaucoma in the world.
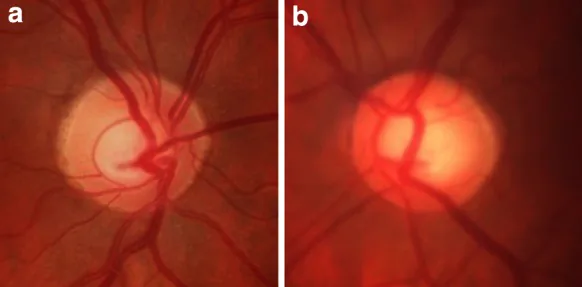
Seo JH, Kim TW, Weinreb RN. Relationship of intraocular pressure and frequency of spontaneous retinal venous pulsation in primary open-angle glaucoma. Ophthalmology. 2012. Figure 1. PMCID: PMC3890055. License: CC BY.
(a) Right eye and (b) left eye fundus photographs. The left optic disc shows an enlarged cup (C/D ratio approximately 0.6) and thinning of the neuroretinal rim. This corresponds to glaucomatous optic neuropathy with asymmetry, discussed in section “2. Main Symptoms and Clinical Findings.”
Most patients with primary open-angle glaucoma are asymptomatic in the early stages. Visual field defects are difficult to recognize, and it is challenging to detect early cases based on subjective symptoms. Many cases are discovered when high intraocular pressure or optic disc cupping is noted during an eye examination for other reasons, such as health checkups or prescription of glasses or contact lenses.
As the disease progresses, subjective symptoms such as “partial blurring” or “areas where objects cannot be recognized” appear. In more advanced cases, patients experience whitish vision, night blindness, glare, and difficulties in daily life such as tripping or bumping into objects. Among glaucoma patients visiting low-vision clinics, common needs include difficulty with reading, walking, writing, and photophobia.
Increased cup-to-disc ratio: Characteristic vertical enlargement of the cup 3)
Asymmetry between eyes: A difference in cup-to-disc ratio greater than 0.2 is considered significant 3)
Thinning or notching of the neuroretinal rim: Commonly occurs at the superior and inferior poles. Disruption of the ISNT rule is a diagnostic clue 3)
Retinal nerve fiber layer defect (NFLD): Wedge-shaped nerve fiber layer defects appear before visual field loss
Disc hemorrhage (DH): Important as a biomarker of progression 3)7). Cup-shaped (proximal) DH is reported to have a higher risk of progression than peripapillary (distal) DH 7)
Beta peripapillary atrophy and lamina dot sign: Appear with glaucomatous changes
Visual Field Findings
Arcuate scotoma: The most characteristic glaucomatous visual field defect3)
Nasal step: Appears as a localized defect bounded by the horizontal meridian
Generalized sensitivity reduction: May be accompanied by diffuse sensitivity loss
Glaucoma hemifield test abnormality: Detects asymmetry between the upper and lower hemifields
Central 10-degree visual field defect: With the widespread use of OCT, macular damage in early stages is recognized, and the importance of 10-degree visual field testing is being re-emphasized
The most characteristic clinical finding is the optic disc appearance, which requires accurate stereoscopic assessment. Visual field defects are detected corresponding to the area of optic nerve damage. Typical visual field patterns include arcuate scotoma, nasal step, paracentral scotoma, and generalized sensitivity reduction 3).
Two theories have been proposed for the pathogenesis of disc hemorrhage: the vascular theory and the mechanical theory 7). The vascular theory suggests impaired autoregulation due to nitric oxide signaling dysfunction and rupture of optic nerve arteries under high shear stress 7). Densitometric analysis of hemorrhages supports an arterial origin 7). Local compression of retinal nerve fibers by disc hemorrhage may cause structural and functional damage 7).
Intraocular pressure (IOP) is the most important risk factor for the development of POAG1)3). Epidemiological studies have shown that the prevalence of POAG increases with rising IOP3). Clinical trials have demonstrated that lowering IOP reduces the risk of developing POAG and its progression; the Early Manifest Glaucoma Trial (EMGT) showed that a 25% reduction in IOP decreased the relative risk of progression by 50%2)3). However, there is considerable individual variation in the susceptibility of the optic nerve to IOP, and as evidenced by normal-tension glaucoma, optic neuropathy can occur even within the normal IOP range3).
Type 2 diabetes has been reported to increase the risk of POAG by 40–100%3)4). Microvascular changes in the optic nerve may contribute to increased susceptibility3). In patients with systemic arterial hypertension, the risk of developing open-angle glaucoma is increased by 17%, and when diabetes is also present, the risk increases by 48%3). In patients on antihypertensive medication, low diastolic perfusion pressure is associated with an increased risk of glaucoma3). Migraine, sleep apnea, peripheral vasospasm (Raynaud’s syndrome), and cardiovascular disease have also been reported as associated factors, but consistent results have not been obtained2)3).
Family history is a strong risk factor, and many genetic loci including polymorphisms have been identified. Among Mendelian mutations, MYOC (myocilin) mutations are the most frequent, accounting for 2–4% of POAG, followed by OPTN (optineurin) 2). The 6th edition of EGS does not recommend genotyping for all POAG patients, but recommends considering genetic testing for families with young-onset disease 2).
QWhy is thin cornea a risk factor for glaucoma?
A
The OHTS showed that thin central corneal thickness (CCT) is an independent risk factor for the development of POAG3)4). Thin corneas tend to yield lower intraocular pressure measurements than actual, leading to underestimation of pressure, which contributes to risk. Another theory suggests that thin CCT reflects reduced rigidity of supporting structures around the optic nerve, such as the lamina cribrosa and sclera, indicating vulnerability to intraocular pressure. In eyes with CCT <555 μm and intraocular pressure >25 mmHg, the 5-year risk of conversion to glaucoma is reported to reach 36%.
Diagnosis of primary open-angle glaucoma requires assessment of intraocular pressure, confirmation of optic disc damage, confirmation of open angle, and evaluation of visual field defects 3)9). In narrow-sense POAG, a definitive diagnosis is made based on four elements: (1) elevated intraocular pressure, (2) glaucomatous changes of the optic disc, (3) visual field defects consistent with disc findings, and (4) exclusion of other causes of elevated intraocular pressure.
Goldmann applanation tonometry (GAT) is the gold standard and is chosen for cases requiring precise intraocular pressure measurement3). It measures based on the Imbert-Fick law with an applanation area of 15.09 mm² (diameter 3.06 mm), and provides the most accurate value when central corneal thickness is 520 μm. Central corneal thickness (CCT) should be measured concurrently, noting that thin corneas lead to underestimation and thick corneas to overestimation 3).
Non-contact tonometers, rebound tonometers (iCare), and Tono-Pen are used as supplementary devices. iCare correlates well with Goldmann applanation tonometry and is easy to use in patients with narrow palpebral fissures and infants. iCare HOME2 allows patients to self-measure at home, which is useful for understanding intraocular pressure fluctuations outside office hours. Phasing (diurnal variation measurement) may be performed to assess diurnal and seasonal variations in intraocular pressure.
It is essential for confirming open angle and excluding secondary glaucoma3). Check for pigment dispersion, exfoliation material, neovascularization, and peripheral anterior synechiae3). It should be performed at the initial visit.
Three-dimensional clinical evaluation of the optic disc is the gold standard 3). Quantitative assessment of RNFL thickness and ganglion cell layer using optical coherence tomography (OCT) is widely used as an objective adjunct 3)9). With the widespread use of OCT, it has become clear that many cases of POAG involve macular damage even at early stages, reaffirming the need for visual field testing within 10 degrees at an earlier stage. For progression monitoring, evaluation of changes over time using fundus photography and OCT is useful, but in advanced glaucoma, OCT has limitations in detecting thinning (floor effect), so visual field testing becomes the main method for determining progression 9). OCT angiography (OCTA) is less affected by the floor effect and may be advantageous for evaluating advanced stages, but standardized methods for its use in clinical practice have not been established 9).
Automated static threshold perimetry using the Humphrey Field Analyzer is the gold standard 3). The SITA (Swedish Interactive Threshold Algorithm) reduces examination time. The Glaucoma Hemifield Test (GHT) detects asymmetry between the upper and lower hemifields. Frequency Doubling Technology (FDT) and SITA-SWAP (Blue-on-Yellow perimetry) are also used for detecting early visual field defects. For progression assessment, event analysis and trend analysis are used together; trend analysis is useful for quantitative evaluation of progression rate 9).
Diseases to be differentiated include ocular hypertension, NTG, primary angle-closure glaucoma, pigmentary glaucoma, exfoliation glaucoma, steroid-induced glaucoma, developmental glaucoma, uveitic secondary glaucoma, plateau iris syndrome, burned-out primary open-angle glaucoma, spontaneously resolved steroid-induced glaucoma, and remission phase of Posner-Schlossman syndrome3). Neuro-ophthalmic diseases (optic neuropathy due to intracranial tumors, superior segmental optic nerve hypoplasia SSOH, etc.) are also differential diagnoses and may require imaging to rule out. Secondary open-angle glaucoma after YAG laser vitreolysis is also included in the differential diagnosis; cases with chronic intraocular pressure elevation due to accumulation of protein particles in the trabecular meshwork have been reported, and postoperative intraocular pressure monitoring is important 8).
QWhat should be done if glaucoma is suspected?
A
Glaucoma suspect is defined as a condition with sustained intraocular pressure elevation, or any of the optic disc, RNFL, or visual field findings suggestive of glaucoma4). In the OHTS, over 90% of untreated OHT patients did not progress to POAG within 5 years 4). The decision to initiate treatment is based on the number and severity of risk factors, or evidence of progressive optic nerve or visual field changes 4). Regular examinations (every 6–12 months) monitor structural and functional changes, and treatment is started when progression is observed. A state with glaucomatous optic nerve abnormalities but no abnormalities on standard static perimetry is called preperimetric glaucoma, and treatment may be considered if risk factors are present 9).
The treatment goals for primary open-angle glaucoma are: (1) control to target intraocular pressure, (2) preservation of the optic nerve and retina, and (3) preservation of the visual field 9). Intraocular pressure reduction is the only evidence-based treatment 1)3)9).
Target intraocular pressure is set individually based on glaucoma stage, untreated intraocular pressure, life expectancy, age, progression of visual field damage, family history, status of the fellow eye, and risk factors 9). Examples of target intraocular pressure by stage: early stage ≤19 mmHg, moderate stage ≤16 mmHg, advanced stage ≤14 mmHg 9). Additionally, based on evidence from various RCTs (EMGT, OHTS, CIGTS, AGIS, etc.), a target of 20–30% reduction from untreated intraocular pressure is recommended 9).
In advanced stages, progression has a greater impact on quality of life, so target intraocular pressure is set lower; if life expectancy is long, more aggressive slowing of progression is aimed for 9). Target intraocular pressure is not absolute and is adjusted as needed during follow-up based on progression 9). For moderate or later stages, achieving sufficient slowing of progression often requires a target in the low teen to sub-teen range, and surgical treatment is frequently needed to achieve this level of intraocular pressure reduction.
Prostanoid FP receptor agonists: Most widely used as first-line therapy. Includes latanoprost, travoprost, tafluprost, and bimatoprost. They enhance uveoscleral outflow, reducing intraocular pressure by approximately 25–35%, administered once daily 9).
EP2 receptor agonist (omidenepag isopropyl): A first-line candidate with a novel mechanism of action, approved in 2018. It is non-inferior to latanoprost. Contraindicated in eyes with intraocular lenses, and combination with FP receptor agonists is not recommended 9).
Beta-blockers: Suppress aqueous humor production. Examples include timolol, carteolol, and betaxolol. Systemic side effects (bradycardia, bronchospasm) require caution 9)
Carbonic anhydrase inhibitors: Suppress aqueous humor production. Includes dorzolamide and brinzolamide eye drops, as well as oral acetazolamide9)
Alpha-2 agonists (brimonidine): Have dual action of suppressing aqueous humor production and enhancing uveoscleral outflow9)
Rho kinase inhibitors (ripasudil): A new drug class that directly promotes trabecular outflow, first approved worldwide in Japan. Conjunctival hyperemia is the main side effect 9)
Laser and Surgical Treatment
SLT (Selective Laser Trabeculoplasty): Uses a 532 nm Q-switched frequency-doubled YAG laser with a spot size of 400 μm, 0.4–1.2 mJ, and 3 nanoseconds, applied to half to the full circumference of the trabecular meshwork9). The LiGHT Trial demonstrated long-term efficacy equal to or better than eye drops, and it is recommended as first-line treatment by EGS 6th edition, AAO PPP, and UK NICE 1)2)10)
Trabeculectomy (with MMC): The most established glaucoma filtering surgery. It is the most common incisional surgery for most types of glaucoma including POAG. The 5-year late infection rate in Japanese patients is reported as 2.2% 9)
Tube shunt surgery: Devices such as Baerveldt glaucoma implant (BG101-350, BG102-350, BG103-250), Ahmed glaucoma valve (FP7, FP8), and Ex-PRESS® microtube shunt are used 6)9)
MIGS (Minimally Invasive Glaucoma Surgery): Various devices including iStent/iStent inject, Hydrus, Kahook Dual Blade, GATT, Trabectome, Xen, PreserFlo, and OMNI are used, targeting reconstruction of the trabecular outflow pathway 6)13)14)
Cyclophotocoagulation: Includes continuous-wave transscleral diode laser (2,000 mW, 2 seconds) and transscleral micropulse (2,000 mW, 80 seconds × 2). It is an option for refractory cases 9)
Treatment policy: The basic principle is to start with monotherapy and limit combination therapy to a maximum of two drugs whenever possible9). Drug selection should consider target intraocular pressure, side effects, frequency of instillation, and patient comfort. At initiation, a unilateral trial (efficacy evaluation by administering to one eye) is desirable9). When multiple drugs are needed, fixed-combination eye drops are useful for maintaining adherence; in Japan, several fixed-combination eye drops containing two ingredients are approved9). If monotherapy is insufficient, consider switching drugs or adding another agent (including fixed combinations). If target intraocular pressure is still not achieved or visual field progression is observed, consider laser therapy or incisional surgery9).
In elderly patients or those at risk of systemic side effects, avoid beta-blockers and choose prostaglandin analogs first, followed by carbonic anhydrase inhibitors, alpha-2 agonists, and Rho kinase inhibitors. Poor adherence is a major factor in disease progression; in Japan, approximately 40% of patients newly prescribed glaucoma eye drops discontinue treatment within about one year9). Providing written instructions, appointment management, and reminder notifications are recommended for continuous long-term care9).
Lower IOP and fewer eye drops at 2 years compared to cataract surgery alone 14)
Long-term follow-up data from EMGT showed that the natural rate of progression without treatment varies greatly by disease type. High-tension glaucoma (HTG) 1.31 dB/year, normal-tension glaucoma (NTG) 0.36 dB/year, and exfoliative glaucoma (PXFG) 3.13 dB/year, with exfoliative glaucoma progressing most rapidly 3).
In the 6-year results of the LiGHT Trial, 69.8% of the SLT first-line treatment group maintained target IOP without additional treatment, and the progression rate was significantly lower at 19.6% vs 26.8% (eye drop group, P=0.006) 10). The number of trabeculectomies was significantly lower in the SLT group (13 eyes) compared to the eye drop group (32 eyes, P<0.001), and the number of cataract surgeries was also significantly lower in the SLT group (57 eyes) compared to the eye drop group (95 eyes, P=0.03). No serious laser-related adverse events were observed 10). Based on these results, the European Glaucoma Society, American Academy of Ophthalmology, and UK NICE recommend SLT as a first-line treatment option for OAG/OHT 1)2)3)10).
In the Scottish Glaucoma Trial, trabeculectomy achieved a 58% reduction in IOP and resulted in less visual field progression than medical therapy (42%) 3). The Moorfields Primary Treatment Trial showed that trabeculectomy had the greatest IOP-lowering effect (60%) 3).
Management of inadequate IOP control after MIGS is a clinical challenge 6). In a panel discussion by multiple experts, options such as trabeculectomy, tube shunt, and suprachoroidal shunt were discussed for advanced POAG cases where MIGS had failed in the fellow eye 6). Failure of Schlemm’s canal surgery suggests restriction of outflow pathways beyond Schlemm’s canal, while limited efficacy of trabeculectomy suggests an exuberant wound healing response 6). Individualized surgical strategies tailored to the characteristics of each case are important 6).
QHow is the type of surgery selected?
A
Surgery selection is determined by comprehensively considering the stage, intraocular pressure level, previous surgical history, patient age and life expectancy, and wound healing tendency 6). For mild to moderate cases, MIGS (trabecular outflow enhancement) is considered 6)13)14). For advanced cases or when the target intraocular pressure is low, trabeculectomy or tube shunt is indicated 6)9). In the Primary Tube Versus Trabeculectomy Study (PTVT), the success rate of Baerveldt 350 was higher in cases with high preoperative intraocular pressure6). It is recommended to learn from the surgical results of the fellow eye and adjust the next intervention 6). SLT as primary treatment has shown long-term outcomes equivalent to or better than eye drops; in the LiGHT Trial, about 70% maintained target intraocular pressure without additional treatment at 6 years 10).
The final common pathway of primary open-angle glaucoma is the loss of retinal ganglion cells (RGCs) at the optic nerve head 5). RGC death is the main pathological process, and the pattern and rate of loss are defined structurally and functionally 5). The mechanisms of damage are broadly divided into intraocular pressure-dependent and intraocular pressure-independent factors.
Elevated intraocular pressure in POAG is thought to result from functional impairment of aqueous humor outflow in the angle and trabecular meshwork. Pathologically, deposition of extracellular matrix on trabecular beams and endothelial meshwork, narrowing of trabecular spaces, and occlusion of Schlemm’s canal are observed. Primary damage to RGC axons occurs at the optic nerve head (ONH), blocking anterograde and retrograde axonal transport 5). Physical remodeling of the lamina cribrosa (LC) at the ONH explains the selective loss of RGC axons in the superior and inferior poles 5).
POAG is not a pathologically diagnosed disease but one of the clinical syndromes. Family history is often observed, and genetics is an important factor in pathogenesis. Many genetic loci including MYOC and OPTN have been identified, but only a few cases can be explained by single gene mutations, suggesting a multifactorial genetic background 2).
Vascular dysregulation is an important intraocular pressure-independent factor 7). In primary open-angle glaucoma, impaired nitric oxide signaling reduces autoregulation, making the optic nerve arteries more susceptible to failure under high shear stress 7). Optic disc hemorrhage is a biomarker of vascular dysregulation, and local compression of RGC axons by the hemorrhage may cause structural and functional damage 7).
Prelaminar wedge defects (PLWDs), wedge-shaped defects in the prelaminar layer, are more frequently observed in POAG than in healthy eyes and are significantly associated with a history of optic disc hemorrhage7). PLWDs are thought to reflect optic nerve vulnerability due to intraocular pressure-independent factors (such as vascular dysfunction) 7).
Other non-intraocular pressure factors include excitotoxic damage (excessive glutamate), autoimmune-mediated neuropathy, loss of neurotrophic factors, and autoregulatory dysfunction of retinal and choroidal vessels. Decreased cerebrospinal fluid pressure may increase the translaminar pressure gradient at the optic nerve head, attracting attention as a factor that can cause optic neuropathy even at normal intraocular pressure. The frequent comorbidity of peripheral circulatory disorders such as cold sensitivity and migraine, as well as cardiovascular diseases in NTG, also suggests the involvement of circulatory disturbance factors.
The 6-year results of the LiGHT Trial have established SLT as a first-line treatment 10). The SLT first-line group showed a significantly lower disease progression rate compared to the eye drop first-line group, with approximately 70% of eyes maintaining target intraocular pressure without additional treatment, and significantly fewer required trabeculectomies and cataract surgeries 10). The EGS 6th edition, AAO PPP, and UK NICE guidelines recommend SLT as a first-line treatment option alongside eye drops 1)2)3).
Evolution of Surgical Strategies for Refractory POAG
Management of advanced POAG after failed MIGS is actively debated 6). Suprachoroidal shunts (e.g., MINIject) may bypass outflow barriers beyond Schlemm’s canal and eliminate bleb-related complications 6). The Paul glaucoma implant (PGI) is expected to provide more predictable early postoperative intraocular pressure and corneal endothelial protection due to its smaller tube diameter compared to conventional tube shunts 6). Combinations of multiple MIGS procedures and different mechanisms targeting trabecular outflow, uveoscleral outflow, and suprachoroidal outflow are also being explored 6). The HORIZON study showed that Hydrus Microstent combined with cataract surgery significantly reduced IOP and the number of eye drops at 5 years 13).
The association between the location of optic disc hemorrhage (proximal vs. distal) and the risk of progression has been reported7). Cup-shaped (proximal) DH has a higher risk of progression than peripapillary (distal) DH, suggesting the involvement of compressive optic neuropathy at the level of the lamina cribrosa on RGC axons7). Densitometry studies have provided findings supporting that optic disc hemorrhages are of arterial origin7).
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Gedde SJ, Lind JT, Wright MM, Chen PP, Muir KW, Vinod K, Li T, Mansberger SL; American Academy of Ophthalmology Preferred Practice Pattern Glaucoma Panel. Primary Open-Angle Glaucoma Suspect Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P151-P192. doi:10.1016/j.ophtha.2020.10.023. PMID:33189698.
Asrani SG, McGlumphy EJ, Al-Aswad LA, Chaya CJ, Lin S, Musch DC, Pitha I, Robin AL, Wirostko B, Johnson TV. The relationship between intraocular pressure and glaucoma: An evolving concept. Prog Retin Eye Res. 2024;103:101303. doi:10.1016/j.preteyeres.2024.101303.
Huang MJ, Samuelson TW, De Francesco T, et al. Managing primary open-angle glaucoma in the setting of suboptimal surgical outcomes in the fellow eye. J Cataract Refract Surg. 2023;49(7):764. doi:10.1097/j.jcrs.0000000000001221.
Verticchio Vercellin A, Pasquale LR, Harris A. Disc hemorrhages in open-angle glaucoma—between a rock and a hard place? JAMA Ophthalmol. 2024;142(10):950-951.
de Vries E, Faraj C, Gerbrandy F, Hulsman C. Secondary open-angle glaucoma following YAG-laser vitreolysis. BMJ Case Rep. 2022;15(4):e248937. doi:10.1136/bcr-2022-248937.
Gazzard G, Konstantakopoulou E, Garway-Heath D, Adeleke M, Vickerstaff V, Ambler G, et al. Laser in Glaucoma and Ocular Hypertension (LiGHT) Trial: Six-Year Results of Primary Selective Laser Trabeculoplasty versus Eye Drops for the Treatment of Glaucoma and Ocular Hypertension. Ophthalmology. 2023;130(2):139-151. doi:10.1016/j.ophtha.2022.09.009. PMID:36122660.
Iwase A, Suzuki Y, Araie M, Yamamoto T, Abe H, Shirato S, et al. The prevalence of primary open-angle glaucoma in Japanese: the Tajimi Study. Ophthalmology. 2004;111(9):1641-8. doi:10.1016/j.ophtha.2004.03.029. PMID:15350316.
Sawaguchi S, Sakai H, Iwase A, Yamamoto T, Abe H, Tomita G, Tomidokoro A, Araie M.. Prevalence of primary angle closure and primary angle-closure glaucoma in a southwestern rural population of Japan: the Kumejima Study. Ophthalmology. 2012;119(6):1134-1142. doi:10.1016/j.ophtha.2011.12.038. PMID:22361313.
Ahmed IIK, De Francesco T, Rhee D, McCabe C, Flowers B, Gazzard G, et al. Long-term Outcomes from the HORIZON Randomized Trial for a Schlemm’s Canal Microstent in Combination Cataract and Glaucoma Surgery. Ophthalmology. 2022;129(7):742-751. doi:10.1016/j.ophtha.2022.02.021. PMID:35218867.
Samuelson TW, Sarkisian SR Jr, Lubeck DM, Stiles MC, Duh YJ, Romo EA, et al. Prospective, Randomized, Controlled Pivotal Trial of an Ab Interno Implanted Trabecular Micro-Bypass in Primary Open-Angle Glaucoma and Cataract: Two-Year Results. Ophthalmology. 2019;126(6):811-821. doi:10.1016/j.ophtha.2019.03.006. PMID:30880108.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.