Primary angle closure glaucoma (PACG) is a disease in which intraocular pressure rises due to primary angle closure caused by genetic background or age-related changes in anterior segment morphology without other factors, and glaucomatous optic neuropathy has already developed1). Primary angle closure (PAC) is a condition in which intraocular pressure is elevated due to primary angle closure, or peripheral anterior synechia (PAS) has formed, but glaucomatous optic neuropathy has not occurred1). Primary angle closure suspect (PACS) refers to a condition in which primary angle closure is present, but there is no elevated intraocular pressure, no organic PAS, and no glaucomatous optic neuropathy1).
The term primary angle closure disease (PACD) is used as a collective term encompassing these three stages and acute primary angle closure glaucoma (acute PACG) and acute primary angle closure (acute PAC) 1)2). The significance of using the umbrella term PACD is to emphasize that the condition in an individual is a continuous spectrum that can progress from PACS to PAC and further to PACG depending on the stage of progression, and to encourage seamless follow-up and early intervention 1)2).
In the 2002 Foster classification, PACS was defined as ITC of 3 quadrants (270 degrees) or more, but currently, following the US Preferred Practice Pattern classification from 2021 onward, ITC of 180 degrees or more is used as the criterion2)12).
PACG and PAC have acute-onset and chronic types. In acute primary angle closure glaucoma and acute primary angle closure, intraocular pressure often rises markedly to 40–80 mmHg, presenting with symptoms such as decreased vision, blurred vision, halos, eye pain, headache, nausea, vomiting, and reduced or absent pupillary light reflex1)2). In contrast, chronic primary angle closure glaucoma (CACG) has no history of acute intraocular pressure elevation, and moderate intraocular pressure elevation of 20–30 mmHg progresses slowly1).
The Tajimi Study reported PACS in 0.2%, PAC in 0.5%, and PACG in 0.6% of individuals aged 40 years or older13). Another Japanese population study reported the prevalence of PACG in those aged 40 years or older as 0.34–0.6%2). Worldwide, approximately 0.7% of people aged 40 years or older have angle closure glaucoma, estimated at 20.2 million in 2013, with 15.5 million concentrated in Asia2)11). It is projected that by 2040, the number of affected individuals will increase by about 50% to 32 million, and more than 5 million may become blind2).
Ethnic differences are notable: reported rates are 2.5–3.8% in Inuit populations, 3.0% in Taiwan, 1.5% in Guangzhou (China), 1.2% in Beijing, 1.1% in Singapore, 1.4% in Mongolia, 0.9% in Thailand, 0.5–0.87% in South India, and 0.4% in Bangladesh2). In European populations, the rate is low at 0–0.6%2). In some Asian populations, PACG accounts for a similar frequency as primary open-angle glaucoma (POAG)2)11). Compared to POAG, PACG has a higher rate of unilateral blindness at initial examination, and the risk of bilateral severe visual impairment is about three times higher2).
Additionally, the age of onset of PACG tends to be higher than that of POAG, with a marked increase in risk in women aged 50 and older2). Regarding the sex ratio of PACG and POAG, while POAG shows minimal gender difference, PACG is 2 to 4 times more common in women than in men2). Women tend to have shallower anterior chamber depth and shorter axial length compared to men, which contributes as an anatomical predisposition2). In Japan, the absolute number of PACG patients is expected to increase with the aging population, posing challenges for the development of medical care systems and the strengthening of narrow-angle screening in primary care2)11).
QIf diagnosed with PACS, should I definitely undergo surgery?
A
Not all PACS eyes require laser treatment uniformly. In the Zhongshan Angle Closure Prevention Trial (ZAP trial) in China, the progression from untreated PACS to PAC or acute attack was about 4% at 6 years and about 12% at 14 years, and prophylactic laser iridotomy reduced the relative risk by 47% at 6 years and 70% at 14 years, but the absolute benefit was small3). The ANA-LIS trial in Singapore also showed a similar trend, with a 5-year progression rate of 9.4% and a risk reduction of 45% with LPI4). Based on these results, the 6th edition of the European Glaucoma Society Guidelines does not recommend routine LPI for healthy PACS eyes, and suggests considering LPI only for high-risk cases such as those with high hyperopia, need for frequent pupil dilation, or difficult access to medical care5). The 5th edition of the Japanese Glaucoma Treatment Guidelines also indicates surgery for cases with positive dark room or prone test results, difficulty in regular examinations, inability to promptly visit a doctor during an acute attack, positive family history, or need for frequent pupil dilation due to diabetic retinopathy, etc.1).
Ni W, et al. A novel histopathologic finding in the Descemet’s membrane of a patient with Peters Anomaly: a case-report and literature review. BMC Ophthalmol. 2015. Figure 2. PMCID: PMC4619091. License: CC BY.
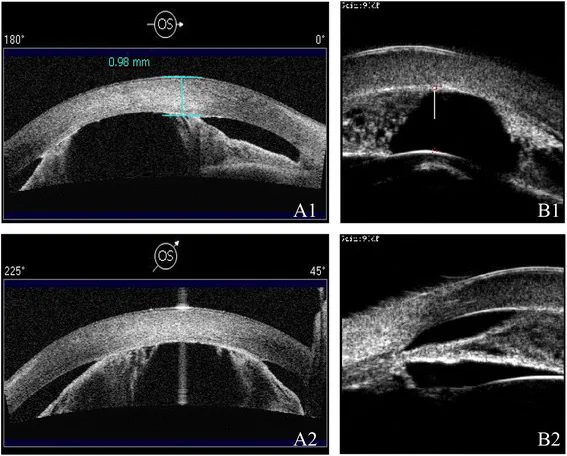
Tomographic images from anterior segment OCT and UBM show a shallow anterior chamber and markedly narrowed angle. Findings suggestive of peripheral anterior synechiae are also observed, indicating anatomical features of PACS/PACG.
PACS and chronic PACG often have few subjective symptoms, and patients frequently notice visual impairment or visual field defects only in the advanced stages1)2). In the chronic phase, intraocular pressure elevation is gradual, so optic nerve damage may progress unnoticed by the patient1). Additionally, in cases of brief intraocular pressure elevation due to mild pupillary block (intermittent angle closure), vague symptoms such as blurred vision in dark places or mild head heaviness may recur, making it important to identify these through history taking2).
In contrast, acute attacks present with dramatic symptoms. These include decreased vision, blurred vision, colored halos around lights (iridescent vision), severe eye pain with ipsilateral headache, and vagal symptoms such as nausea and vomiting 1)2). Iridescent vision is caused by abnormal light refraction due to corneal edema, resulting in seeing colored rings around light bulbs or streetlights. Because headache and nausea may dominate the clinical picture, patients may be misdirected to neurology or gastroenterology departments; therefore, any patient with unexplained severe headache accompanied by ocular symptoms requires an ophthalmological evaluation 2)7). Additionally, subacute attacks with few symptoms exist, where persistently elevated intraocular pressure without clear pain can lead to progressive optic nerve damage; thus, fundus and angle assessments should not be omitted 1)2).
Indentation gonioscopy: Double hump sign (iris indents in a bimodal pattern)
UBM: Anterior positioning of the ciliary body, disappearance of the ciliary sulcus, thickening of the iris root14)
Definitive diagnosis: When angle closure and intraocular pressure elevation are reproduced by mydriasis even after LPI
QWhat symptoms occur in an acute glaucoma attack?
A
In an acute primary angle closure glaucoma attack, intraocular pressure rises rapidly to 40–80 mmHg within a short time, causing severe eye pain and ipsilateral headache, decreased vision, blurred vision, seeing rainbow-colored rings around lights (halos), and nausea/vomiting1)2). Typical signs include conjunctival injection, corneal edema, and a moderately dilated, fixed pupil1)2). Systemic symptoms may predominate, leading to misdiagnosis as gastrointestinal disorders or migraine2)7). If left untreated for several hours, irreversible optic nerve damage occurs, so prompt ophthalmologic evaluation is necessary when suspected2)7).
The pathogenesis of primary angle closure glaucoma and primary angle closure disease often involves multiple mechanisms rather than a single mechanism 1)2)10).
Relative pupillary block: The contact between the posterior iris surface and the anterior lens surface impedes aqueous humor outflow from the posterior chamber to the anterior chamber, increasing posterior chamber pressure, causing the iris to bulge forward and cover the trabecular meshwork. This is the most common mechanism of PACD 1)2).
Plateau iris: An anatomical abnormality in which the ciliary body is positioned anteriorly, pushing the iris root forward, directly occluding the angle upon pupil dilation 1)14).
Lens-related factors: Age-related increase in lens thickness and anterior displacement of the lens. Prominent in advanced cataracts 1)10).
Post-lens factors: Anterior movement of the iris-lens diaphragm due to morphological abnormalities of the ciliary body, choroid, or vitreous body1).
Known lifestyle triggers for acute attacks include reading or watching movies in the dark, prolonged head-down posture (gardening, surgery, long-distance driving), natural mydriasis at night, oral/inhaled/nasal medications with anticholinergic effects, effects of mydriatic examinations, and severe stress 2)7). In particular, premedication for gastroscopy in elderly women, psychiatric medications, Parkinson’s disease treatments, and anticholinergic inhalers for asthma/COPD are easily overlooked, and collaboration with the prescribing physician is important 2)7). Patients with PAC predisposition should be advised to consult an ophthalmologist before using over-the-counter cold medications, nasal sprays, motion sickness remedies, or antihistamines 2). Additionally, if a patient aged 50 or older with hyperopia postpones cataract surgery, the risk of an attack increases with age-related lens thickening; therefore, the decision for cataract surgery itself can be a preventive intervention 6)10).
Gonioscopy is the most important examination for diagnosing primary angle closure disease and is the gold standard 1)2)5). After topical anesthesia, static gonioscopy is performed in the primary position without compression, using a short, narrow slit beam. Care is taken to avoid pupil constriction from the slit light, and the anatomical structures of the angle recess (Schwalbe’s line, trabecular meshwork, scleral spur, ciliary body band), micro-PAS, and angle pigmentation are evaluated 2). Then, dynamic/compression gonioscopy is used to differentiate functional closure from organic closure (PAS). According to the Shaffer-Kanski classification, grade 2 or less (angle ≤20 degrees) indicates possible angle closure, and grade 1 or less indicates high risk of closure.
This is a simple screening method that can be performed with only a slit-lamp microscope. A slit light is directed at the temporal limbus at a 60-degree angle, and the ratio of peripheral anterior chamber depth to corneal thickness is evaluated. If the anterior chamber depth is 1/4 or less of the corneal thickness (Grade 1–2), angle closure is likely, and gonioscopy must always be performed 2).
Assessment of endothelial cell loss in the affected eye, safety evaluation for LPI
Anterior segment OCT allows rapid, non-contact quantitative assessment and is also used for longitudinal progression prediction. The STAR Analysis in CASIA2 can automatically analyze AOD500 in 360 degrees, which is useful for narrow-angle screening 2). However, since it is difficult to distinguish color information or organic closure, it is not a replacement for gonioscopy but rather a complementary tool 2)5). UBM is contact-based and time-consuming, but it surpasses anterior segment OCT in analyzing the ciliary body and posterior iris surface, and is essential for definitive diagnosis of plateau iris2)14).
Provocative tests such as the dark room test, prone test, and mydriatic test have limited diagnostic power. The ZAP test was reported to be unable to identify high-risk groups for progression using the dark room prone test 3). Therefore, diagnosis is made by comprehensive evaluation of clinical findings, gonioscopic findings, and imaging findings.
The following differential diagnoses should always be considered 1)2):
In principle, PACD is bilateral. If the other eye shows a deep anterior chamber and wide angle, secondary causes should be strongly suspected 2)7). In particular, for unilateral acute attacks with lens subluxation or trauma history, consider traumatic lens dislocation; for bilateral acute attacks in young patients, consider sulfonamide-induced (e.g., topiramate) 2). In neovascular glaucoma, check for iris rubeosis and history of posterior segment diseases (diabetic retinopathy, central retinal vein occlusion, etc.) 1).
For the diagnosis of PACG, evidence of glaucomatous optic neuropathy is essential 1)2). In the acute phase, detailed fundus examination is difficult due to corneal edema, but using retinal/optic nerveOCT instead of indirect ophthalmoscopy or anterior segment OCT allows evaluation of the optic disc, retinal nerve fiber layer (RNFL), and macular ganglion cell complex (GCC) without pupil dilation 2). During an attack, the RNFL is temporarily thickened due to axonal swelling, then returns to normal after 1 month, and becomes thinner after 3 months; therefore, longitudinal evaluation is necessary 2). Visual field testing should be performed after the attack subsides using Humphrey 24-2 SITA or equivalent automated static perimetry, and progression is monitored in the same manner as for POAG1)5).
QHow do you choose between anterior segment OCT and ultrasound biomicroscopy (UBM)?
A
Anterior segment OCT is non-contact, allows quantitative evaluation of the angle in 360 degrees in a short time, and is suitable for outpatient screening and longitudinal comparison. The CASIA2 STAR Analysis automatically analyzes AOD500 from 16 cross-sections and can display the ITC area as a color map 2). On the other hand, UBM is contact-based and time-consuming, but because it uses ultrasound, it can visualize the ciliary body and posterior iris structures, and is indispensable for diagnosing plateau iris, characterized by anterior positioning of the ciliary body and disappearance of the ciliary sulcus 2)14). UBM is also the first choice when malignant glaucoma, ciliary body tumors, or organic lesions behind the lens are suspected. In clinical practice, anterior segment OCT is generally used for screening and longitudinal evaluation, while UBM is used for ciliary body evaluation, confirmation of plateau iris, and differential diagnosis 2)5).
The treatment goals are to relieve angle closure, achieve long-term intraocular pressure control, and prevent optic nerve damage 1)2)5). Treatment strategies differ depending on the stage (PACS/PAC/PACG) and whether it is acute or chronic.
Most PACS do not progress to PAC or PACG, but a certain proportion do, so risk-based management is recommended 1)2)3).
Risk
Recommended Management
Low risk (other than elderly women, no family history, good access to healthcare)
Observation 2)3)5)
Moderate to high risk (high hyperopia, family history of PACG, frequent need for pupil dilation, poor access to healthcare, regular use of anticholinergic drugs)
In at-risk individuals, acute attacks can be triggered by over-the-counter medications with anticholinergic effects, such as cold remedies, sleep aids, and motion sickness drugs. Therefore, patient education and instructions for emergency consultation when symptoms occur are important2)7).
PAC / PACG (cases due to relative pupillary block)
The 5th edition of the Glaucoma Clinical Practice Guidelines recommends laser iridotomy or lens extraction to relieve pupillary block as the first-line treatment (recommendation level 1A)1). Since most cases are bilateral, if PACG or PAC is found in one eye, prophylactic LPI (1A) or lens extraction (1A) should also be performed for the narrow angle of the fellow eye1).
Laser iridotomy (LPI): Performed with Nd:YAG alone or in combination with argon laser. Argon-only irradiation is not recommended due to a high risk of endothelial damage1). Complications include transient intraocular pressure elevation, anterior chamber hemorrhage, localized cataract, corneal endothelial damage, secondary bullous keratopathy, and visual symptoms such as glare and halo2).
Lens extraction (phacoemulsification + intraocular lens implantation): Fundamentally resolves pupillary block, increases anterior chamber depth, and widens the angle1)10). The EAGLE trial compared early clear lens extraction with LPI in patients aged 50 years or older with symptomatic PAC (IOP ≥30 mmHg) or PACG, and found that at 3 years, the lens extraction group was superior in QoL (EQ-5D) and IOP control, with approximately 10 times higher probability of maintaining IOP control without eye drops6). A UK cost analysis estimated favorable cost-effectiveness at 3 years and cost savings at 10 years2)6). The 6th edition of the European Glaucoma Society Guidelines strongly recommends either lens extraction or LPI for PAC/PACG in patients aged 50 years or older5).
Peripheral iridectomy: An option for cases where LPI is difficult due to corneal opacity, etc.1). Although it is an invasive intraocular surgery with associated risks, it can reliably restore aqueous humor flow1).
Site selection for LPI: Although the 12 o’clock position was previously recommended, reports of visual symptoms (dysphotopsia) have led to comparisons of superotemporal or horizontal (3 or 9 o’clock) placements. Results of randomized trials are inconsistent, but the choice between a position well covered by the upper eyelid in the superior quadrant or a horizontal position is determined by each institution’s policy2). Most postoperative dysphotopsia (glare, diplopia, linear photopsia) resolves spontaneously within 6 months2).
QWhy is lens extraction highlighted in the EAGLE trial?
A
The EAGLE (Effectiveness in Angle-Closure Glaucoma of Lens Extraction) trial was a multicenter randomized controlled trial primarily conducted in the UK, which assigned 419 patients aged 50 years or older with symptomatic PAC (intraocular pressure ≥30 mmHg) or PACG to early clear lens extraction (CLE) or LPI6). At 3 years, the CLE group was superior in terms of QoL indicators (EQ-5D), intraocular pressure control, and need for additional treatment; the probability of maintaining target intraocular pressure without medication was approximately 10 times higher in the CLE group than in the LPI group 6). A cost analysis in the UK estimated that CLE was cost-effective at 3 years and cost-saving at 10 years 2)6). In response, the American Academy of Ophthalmology’s Primary Angle-Closure Disease Preferred Practice Pattern also presents early lens extraction as an initial treatment option for PAC and PACG with high intraocular pressure, even in cases without visually significant cataract2). The 6th edition of the European Glaucoma Society guidelines also strongly recommends lens extraction and LPI equally for PAC and PACG in patients aged 50 years or older 5). The 5th edition of the Japanese Glaucoma Treatment Guidelines also lists it as a first-line option alongside LPI with a recommendation level of 1A 1).
Treatment of Acute Primary Angle Closure Glaucoma (APAC)
Acute attack is an ophthalmic emergency, and early reduction of intraocular pressure and release of pupillary block determine visual prognosis 1)2)7). The 5th edition of the Japanese Glaucoma Treatment Guidelines recommends the following stepwise treatment 1).
Initial pharmacotherapy:
Hyperosmotic agents: Intravenous infusion of 20% D-mannitol 1.0–2.0 g/kg over 30–60 minutes. Intraocular pressure reaches its lowest point 60–90 minutes after starting infusion, and the effect lasts 4–6 hours. Use with caution in patients with renal impairment or heart failure 1). Glycerol is infused intravenously at 300–500 mL over 45–90 minutes; monitor blood glucose in diabetic patients 1).
Miotics: Instill 1% or 2% pilocarpine hydrochloride eye drops 2–3 times per hour 1). However, if intraocular pressure is extremely high and the pupillary sphincter is ischemic with loss of light reflex, miotic effect may not be expected, and frequent instillation should be avoided because forward movement of the ciliary muscle may worsen pupillary block1).
Anti-inflammatory: Topical steroids such as betamethasone are used to calm anterior chamber inflammation1).
Surgical treatment:
The 5th edition of the Glaucoma Practice Guidelines recommends lens reconstruction as the first choice for acute primary angle closure glaucoma and acute primary angle closure1). If emergency surgery cannot be performed on the same day, first lower intraocular pressure with the above medications, then perform LPI after corneal clearing1). An example of LPI laser settings: first, use an argon laser with 200–400 μm, 200 mW, 0.2 seconds to stretch the iris; then, use 50 μm, 800–1,000 mW, 0.02 seconds to thin it until just before perforation; finally, apply 1–2 shots of Nd:YAG laser at 2.0–4.0 mJ for perforation. The total number of shots should ideally be less than 100 to protect the corneal endothelium1). In cases of corneal opacity, consider switching to surgical peripheral iridectomy.
In a consensus on acute primary angle closure attack (APACA) published in 2025 by the Asia-Pacific Glaucoma Society (APGS) and the Academy of Asia-Pacific Professors of Ophthalmology, it is proposed that for cases with intraocular pressure exceeding 50 mmHg after onset, conventional drug therapy alone is slow to take effect and carries risks of systemic complications, so the following alternative treatments should be actively considered7).
Argon laser peripheral iridoplasty (ALPI): A procedure that uses low-power, long-duration, large-spot laser to contract the peripheral iris and mechanically widen the angle. A randomized controlled trial showed that mean intraocular pressure decreased to 30.8 mmHg at 15 minutes and 24.1 mmHg at 30 minutes after ALPI, reaching target pressure more quickly than conventional drug therapy7).
Laser pupilloplasty (LPP): Uses a 532 nm laser to contract and evert the pupillary margin, relieving pupillary block. It can be performed even with slightly reduced corneal clarity and is used in combination with ALPI7).
Anterior chamber paracentesis (ACP): A procedure that decompresses the anterior chamber using a 30 G needle or 15-degree knife, immediately lowering intraocular pressure. It can be performed even in facilities without an argon laser7).
These alternative treatments are recommended to avoid emergency trabeculectomy or emergency phacoemulsification in “hot and angry” eyes, which were previously avoided7). Early phacoemulsification after the acute attack subsides may be considered as an option to prevent additional damage to retinal ganglion cells7).
Management of the fellow eye:
Without prophylactic LPI, the contralateral eye after APAC can develop an acute attack in about half of cases within 5 years 2). In principle, prophylactic LPI should be performed promptly, and while waiting, miotic eye drops (pilocarpine) should be started 2)7). Long-term administration of pilocarpine is not appropriate as chronic therapy because it carries risks of poor pupillary dilation, posterior synechiae, cataract progression, and retinal detachment; it should only be used as a bridge until LPI is performed 2). Even after prophylactic LPI in the contralateral eye, cases of PACG developing within 5–6 years have been reported, so long-term follow-up is essential 2).
Treatment of Chronic Primary Angle-Closure Glaucoma
For residual elevated intraocular pressure (residual glaucoma) after resolution of pupillary block, medical therapy, laser treatment, and incisional surgery similar to that for primary open-angle glaucoma are performed 1).
Medical therapy: Prostaglandin/prostanoid-related drugs are the first-line choice 1)5). Beta-blockers, alpha-2 agonists, Rho kinase inhibitors, and carbonic anhydrase inhibitors are added as needed.
Lens extraction: Effective for both resolving pupillary block and opening the angle; it alone has an intraocular pressure-lowering effect (recommendation level 1A) 1). However, in cases with extensive PAS (≥50% of the angle), the IOP-lowering effect is limited 1)10).
Goniosynechialysis: Indicated in cases with extensive PAS; when combined with lens extraction, it can both prevent re-synechiae and lower IOP1).
Trabeculotomy: Applied to areas where the trabecular meshwork is open; also used in combination for PAS lysis 1).
Trabeculectomy: Indicated in cases with inadequate IOP control on medication, long-standing PAS, or poor angle visualization. In eyes with narrow angles, there is a risk of complications such as postoperative shallow anterior chamber, choroidal detachment, and malignant glaucoma, so careful management is required 1)9). The 6th edition of the European Glaucoma Society guidelines recommends trabeculectomy as the first-choice surgery for pseudophakic PACG5).
Minimally invasive glaucoma surgery (MIGS): MIGS for eyes with angle closure was traditionally contraindicated, but in recent years its indications have expanded because combined phacoemulsification provides access to the angle. A meta-analysis of 23 studies including 875 cases showed that MIGS (with or without phaco) reduced intraocular pressure by an average of 7.71 mmHg (95% CI 5.16–10.26) and the number of glaucoma medications by an average of 1.57 (95% CI 1.17–1.96) at one year 8). Ab interno trabeculotomy (AIT) was superior to endoscopic cyclophotocoagulation and iStent, and phaco-MIGS had a greater medication reduction effect than phaco alone 8). The complication rate was 16%, most being mild transient hyphema8). In mild to moderate PACG with cataract, phaco + MIGS can be considered as an option before transitioning to trabeculectomy8).
In plateau iris, intraocular pressure control may not be achieved by relieving pupillary block alone 1)14).
Pilocarpine eye drops: They stretch the peripheral iris and widen the angle, but the effect is uncertain, and long-term use can cause poor dilation, posterior synechiae, and cataract progression 1).
Laser gonioplasty (LGP): Using an Abraham lens, argon laser is applied with spot size 500 μm, duration 0.2–0.5 seconds, and power 200 mW as a standard, targeting approximately 15 shots per quadrant over half or the full circumference of the peripheral iris1). In cases with combined pupillary block mechanism, LPI is performed first, followed by LGP 1).
Lens extraction: When the crystalline lens is replaced with an intraocular lens, the anterior chamber depth increases, and in eyes with angle closure, the ciliary processes move further posteriorly postoperatively, further opening the angle. Therefore, it is selected as a reliable method for angle widening 1)6)14).
Follow-up observation: Data on long-term efficacy are limited; after surgery, continued use of pilocarpine eye drops and periodic angle evaluation with UBM are recommended 1)14).
Lens extraction combined with endoscopic cyclophotocoagulation (ECP): Small case series have reported that it acts on the morphology of the ciliary processes themselves and may improve intraocular pressure control 2). A prospective comparative trial showed no significant difference in postoperative intraocular pressure compared to phaco alone, but anterior segment OCT measurements showed greater angle widening 2).
Patient education: Explain to the patient in advance that LPI is not a definitive solution for plateau iris, and inform them that there is a risk of recurrent attacks due to mydriatic stimulation even after LPI1)14).
Most PACD cases are based on relative pupillary block as the fundamental mechanism1)2). The iris-lens contact in the pupillary area increases resistance to aqueous humor flow from the posterior chamber to the anterior chamber. When posterior chamber pressure becomes relatively high, the iris bulges forward and almost completely covers the trabecular meshwork in the periphery. This creates functional closure of the angle. In acute attacks, anterior movement of the lens and edema of the iris stroma are added to this condition, further exacerbating pupillary block and leading to a vicious cycle of rapid intraocular pressure elevation1)2).
Pupillary block is most likely to be maximal when the pupil is in a moderately dilated position. This is why reading in dim light, waking at night, drugs with anticholinergic effects, and a head-down posture can trigger attacks2)7).
In plateau iris, the ciliary body is positioned anteriorly, mechanically pushing the iris root forward. The central anterior chamber depth is relatively preserved, so it appears normal at first glance, but upon dilation, the peripheral iris rides over the ciliary processes and directly closes the angle1)14). UBM features include anterior positioning of the ciliary body, disappearance of the ciliary sulcus, a thick and anteriorly bowed iris root, and a narrow angle recess14).
Lens factors contribute through age-related increase in lens thickness and anterior displacement. As the lens thickens, the iris-lens contact area expands, strengthening pupillary block1)10). Also, a thicker lens results in shallower anterior chamber depth, further manifesting anatomical predisposition2)10). This is the rationale for the angle-opening effect of lens extraction6)10).
Secondary trabecular dysfunction and optic neuropathy
Prolonged or repeated iris-trabecular contact causes irreversible functional damage to the trabecular meshwork itself, leading to PAS formation1)2). Therefore, even after relieving pupillary block, chronic intraocular pressure elevation persists in a certain proportion of cases, which is called residual glaucoma1). According to the APGS consensus, even after successful LPI following an acute attack, up to 58% of cases may progress to chronic PACG7). Multiple mechanisms have been proposed, including mechanical damage to trabecular cells, involvement of inflammatory mediators, and collapse of Schlemm’s canal, but the complete pathogenesis has not been fully elucidated7)10).
The retinal nerve fiber layer (RNFL) after an acute attack transiently thickens due to axonal swelling immediately after the attack, returns to normal values in about one month, and then becomes thinner after three months 2). This indicates that axonal swelling and secondary degeneration occur separately over time, and can be tracked by longitudinal OCT evaluation. In a study following the long-term outcomes of untreated APAC cases for 4–10 years, 18% progressed to legal blindness and 58% had visual acuity worse than 20/40 2). Corneal endothelial cell density also decreases in proportion to the duration of the attack, resulting in pleomorphism (variation) and polymegethism (size variation) of cell morphology 2). The effects of high intraocular pressure and ischemia also extend to ciliary body blood flow, and aqueous humor production itself may temporarily decrease, sometimes worsening the response to drug therapy 7).
Ischemia-reperfusion injury and post-attack ganglion cell loss
The marked elevation of intraocular pressure during an acute attack causes impaired blood flow to the optic nerve head and retina, and upon resolution of the attack, reperfusion leads to oxidative stress and production of inflammatory cytokines 7). Animal experiments and human longitudinal studies suggest that this ischemia-reperfusion injury results in continued loss of retinal ganglion cells (RGCs) for some time even after intraocular pressure is lowered 7). This finding underscores the importance of rapidly lowering intraocular pressure during an attack and provides the theoretical basis for the APGS recommendation of prompt intraocular pressure reduction using alternative treatments (ALPI, LPP, ACP) 7).
The ZAP trial, as a large-scale randomized study in an Asian population, provided foundational data for PACS management and prompted reconsideration of routine prophylactic LPI3). The Singapore ANA-LIS trial also supports this 4). Meanwhile, the EAGLE trial demonstrated the superiority of early lens extraction for PAC and PACG, and this has been adopted in major guidelines in the United States, Europe, and Japan 1)2)5)6). Based on these results, the 2026 edition of the Primary Angle-Closure Disease Preferred Practice Pattern explicitly lists lens extraction as a strong initial treatment option for PAC and PACG2).
The 2025 consensus of APGS/AAPPO proposes a treatment flow that actively incorporates rapid intraocular pressure reduction using alternative procedures such as ALPI, LPP, and ACP, as well as early phacoemulsification after attack sedation, because conventional drug therapy alone has a slow onset of action and carries risks of systemic side effects in elderly patients and those with comorbidities 7). This is also important from the perspective of suppressing ischemia-reperfusion injury, which can cause progressive RGC loss after an attack 7).
Longitudinal analysis of anterior segment OCT has reported that increases in anterior lens vault and decreases in angle width are predictive factors for PACD progression over 3 to 6 years 2). In the future, it is expected that individual risk assessment based on these biometric indicators will guide decisions for LPI or lens extraction. A study using AI automatic diagnosis and Markov models in China showed that population screening combined with AI for individuals aged 65 and older can suppress PACG progression, but challenges remain in recovering screening costs 2).
MIGS was initially contraindicated in PACG, but with the advent of combined phacoemulsification that provides access to the angle, it is gaining attention as a minimally invasive option for mild to moderate PACG8). Meta-analyses have shown the superiority of AIT, but the number of studies and follow-up periods are limited, and further validation of long-term outcomes and cost-effectiveness is needed 8). Compared to trabeculectomy, MIGS has a lower risk of bleb-related complications and bleb infections, which may significantly influence surgical choices for PACG with cataract8).
In recent years, genome-wide association studies have identified genetic polymorphisms (e.g., PLEKHA7, COL11A1, PCMTD1-ST18) that increase the risk of PACD, advancing our understanding of anatomical predisposition and individualized risk assessment 2). In the future, screening strategies combining genetic information and biometric data may be established for individuals with a positive family history or high-risk ethnic groups 2).
From the perspective of patient education, it is important for long-term visual function preservation to educate individuals at risk for PACD about the symptoms of acute attacks and the need for prompt medical attention, to provide information on avoiding over-the-counter and prescription drugs that cause pupillary dilation, and to recommend ophthalmic examinations for family members (especially first-degree relatives) 2).
American Academy of Ophthalmology. Primary Angle-Closure Disease Preferred Practice Pattern®. San Francisco: American Academy of Ophthalmology; 2025.
He M, Jiang Y, Huang S, Chang DS, Munoz B, Aung T, Foster PJ, Friedman DS. Laser peripheral iridotomy for the prevention of angle closure: a single-centre, randomised controlled trial. Lancet (London, England). 2019;393(10181):1609-1618. doi:10.1016/S0140-6736(18)32607-2. PMID:30878226.
Baskaran M, Kumar RS, Friedman DS, Lu QS, Wong HT, Chew PTK, et al. The Singapore Asymptomatic Narrow Angles Laser Iridotomy Study: Five-Year Results of a Randomized Controlled Trial. Ophthalmology. 2022;129(2):147-158. doi:10.1016/j.ophtha.2021.08.017. PMID:34453952.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Augusto Azuara-Blanco, Jennifer Burr, Craig Ramsay, David Cooper, Paul J Foster, David S Friedman, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. The Lancet. 2016;388(10052):1389-1397. doi:10.1016/s0140-6736(16)30956-4.
Chan PP, Zhang X, Aung T, Chew PTK, Congdon N, Dada T, Fang SK, He M, Kim CY, Lai JSM, Lee JWY, Liang Y, Lingam V, Liu CY, Rojanapongpun P, Sun X, Tang X, Tham CCY. Controversies, consensuses, and guidelines for acute primary angle closure attack (APACA) by the Asia-Pacific Glaucoma Society (APGS) and the Academy of Asia-Pacific Professors of Ophthalmology (AAPPO). Asia Pac J Ophthalmol (Phila). 2025;14(6):100223. doi:10.1016/j.apjo.2025.100223. PMID:40615047.
Paik B, Chua CH, Yip LW, Yip VCH. Outcomes and Complications of Minimally Invasive Glaucoma Surgeries (MIGS) in Primary Angle Closure and Primary Angle Closure Glaucoma: A Systematic Review and Meta-Analysis. Clinical ophthalmology (Auckland, N.Z.). 2025;19:483-506. doi:10.2147/OPTH.S505856. PMID:39963523; PMCID:PMC11830760.
Song BJ, Ramanathan M, Morales E, Law SK, Giaconi JA, Coleman AL, et al. Trabeculectomy and Combined Phacoemulsification-Trabeculectomy: Outcomes and Risk Factors for Failure in Primary Angle Closure Glaucoma. Journal of glaucoma. 2016;25(9):763-9. doi:10.1097/IJG.0000000000000493. PMID:27513900; PMCID:PMC5001924.
Tarongoy P, Ho CL, Walton DS. Angle-closure glaucoma: the role of the lens in the pathogenesis, prevention, and treatment. Survey of ophthalmology. 2009;54(2):211-25. doi:10.1016/j.survophthal.2008.12.002. PMID:19298900.
Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262-267.
Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The definition and classification of glaucoma in prevalence surveys. The British journal of ophthalmology. 2002;86(2):238-42. doi:10.1136/bjo.86.2.238. PMID:11815354; PMCID:PMC1771026.
Yamamoto T, Iwase A, Araie M, Suzuki Y, Abe H, Shirato S, Kuwayama Y, Mishima HK, Shimizu H, Tomita G, Inoue Y, Kitazawa Y, Tajimi Study Group, Japan Glaucoma Society.. The Tajimi Study report 2: prevalence of primary angle closure and secondary glaucoma in a Japanese population. Ophthalmology. 2005;112(10):1661-1669. doi:10.1016/j.ophtha.2005.05.012. PMID:16111758.
Kumar RS, Baskaran M, Chew PT, Friedman DS, Handa S, Lavanya R, et al. Prevalence of plateau iris in primary angle closure suspects an ultrasound biomicroscopy study. Ophthalmology. 2008;115(3):430-4. doi:10.1016/j.ophtha.2007.07.026. PMID:17900691.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.