Trabeculotomy is a surgery that incises the juxtacanalicular trabecular meshwork, where aqueous outflow resistance is highest, to improve aqueous outflow obstruction and lower intraocular pressure. Compared to filtering surgery (trabeculectomy), it has fewer intraoperative and postoperative complications, but its intraocular pressure lowering effect is inferior to filtering surgery.
Conventional trabeculotomy was an ab externo procedure requiring conjunctival incision and scleral flap creation. In recent years, minimally invasive procedures called minimally invasive glaucoma surgery (MIGS) have been introduced clinically and are performed at an earlier stage than the indication for trabeculectomy1). MIGS are non-bleb-forming procedures performed ab interno (from inside the eye), minimizing disruption to normal anatomy and physiology3).
The defining features of MIGS are summarized in the following five points3).
High safety: Low risk of serious complications such as hypotony and choroidal detachment
Minimal disruption to normal anatomy: Enhances physiological outflow mechanisms
Ab interno approach: Performed from inside the eye through a corneal incision
Efficacy: Achieves at least 20% intraocular pressure reduction or reduction of one medication
Rapid recovery: Minimal additional downtime
In the context of glaucoma surgery, outflow reconstruction surgery (trabeculotomy/MIGS) is indicated for cases where adequate intraocular pressure reduction cannot be achieved with medication or laser therapy 1). The main target disease types are primary open-angle glaucoma, normal-tension glaucoma, exfoliation glaucoma, steroidglaucoma, and developmental glaucoma (childhood glaucoma). Exfoliation glaucoma and steroidglaucoma show greater intraocular pressure reduction than primary open-angle glaucoma.
Glaucoma treatment is performed stepwise: medication (first choice) → laser therapy (SLT, etc.) → incisional surgery 1). Among incisional surgeries, trabeculectomy is the most widely performed filtering surgery, but outflow reconstruction surgery (trabeculotomy/MIGS) has the major advantage of allowing earlier intervention than trabeculectomy1). For advanced glaucoma or cases requiring low target intraocular pressure, trabeculectomy or tube shunt surgery is still necessary.
Devices that form a bleb under the conjunctiva (XEN Gel Stent, PreserFlo MicroShunt, etc.) have different safety and efficacy profiles and are classified as MIBS (minimally invasive bleb surgery) rather than MIGS3).
The approval history of intraocular drainage devices combined with cataract surgery is as follows 2).
iStent (titanium, heparin-coated): Approved in 2016. Available for right and left eyes. Set in a disposable inserter.
iStent inject W (titanium): Approved on October 31, 2019. Two bullet-shaped stents placed in one eye. No distinction between left and right eyes. Approved for standalone surgery from July 11, 2024.
Hydrus (nitinol, crescent-shaped): Approved on June 6, 2024. One stent loaded in a delivery system. No distinction between left and right eyes.
Traditionally, for early to moderate open-angle glaucoma, combined surgery with cataract surgery was performed using an external approach with a trabeculotome (metal probe) 2). However, the external approach required conjunctival incision, and if additional filtering surgery such as trabeculectomy was needed later, conjunctival scarring often hindered the surgery 2). To solve this problem, outflow reconstruction surgery performed from the anterior chamber side under gonioscopic guidance (using nylon thread, handpiece, hook, blade, etc.) was developed, allowing surgery without creating conjunctival scarring 2).
In the European Union, iStent was approved in 2004, iStent inject W in 2010, and Hydrus in 2011. In the US FDA, iStent was approved in 2012, and iStent inject W and Hydrus in 20182).
QHow is MIGS different from traditional glaucoma surgery?
A
MIGS is performed through small incisions from inside the eye (ab interno), resulting in faster recovery and lower risk of complications. On the other hand, traditional surgeries such as trabeculectomy can lower intraocular pressure more significantly but carry risks of serious complications like hypotony and infection. MIGS is suitable for mild to moderate glaucoma and preserves the conjunctiva, so it does not compromise the success rate of future filtering surgery. For advanced glaucoma requiring low target intraocular pressure, traditional surgery is chosen. Please consult your doctor.
2. Classification and Techniques of Surgical Procedures
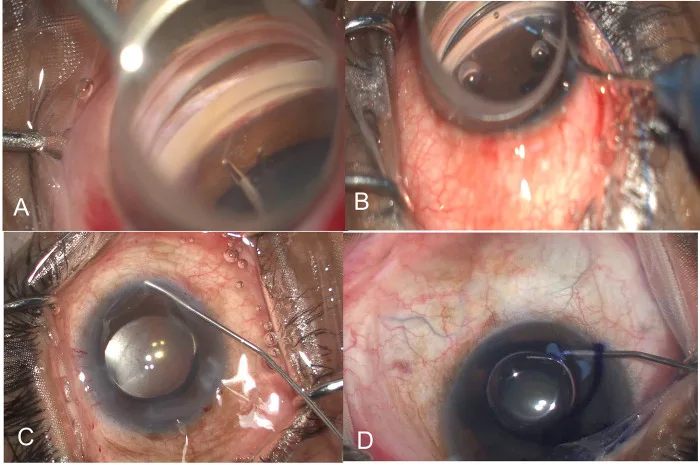
Rao A, Mukherjee S. Intraoperative predictors for clinical outcomes after microinvasive glaucoma surgery. PLoS One. 2023;18(11):e0293212. Figure 1. PMCID: PMC10635545. License: CC BY 4.0.
A shows micro-MIGS (trabecular band excision) with microforceps peeling the trabecular meshwork, B shows GATT (gonioscopy-assisted transluminal trabeculotomy) with Prolene suture passing through Schlemm’s canal, C shows blanching effect of collector channels after opening Schlemm’s canal, D shows trabecular meshwork staining with trypan blue. These correspond to individual steps of angle manipulation in GATT and intraocular methods discussed in the section “Classification and Techniques of Surgical Procedures.”
Glaucoma surgery is broadly classified into four categories: filtering surgery, aqueous outflow reconstruction, pupillary block relief surgery, and cyclodestructive surgery1). The procedures included in aqueous outflow reconstruction are further divided into three groups based on approach and instruments used.
Trabeculotomy (external approach): Conventional method where a trabeculotome is inserted into Schlemm’s canal and rotated into the anterior chamber.
Trabeculotomy (internal approach): MIGS that incises the trabecular meshwork under direct gonioscopic view using microhooks, KDB, Trabectome, suture, etc.
Intraocular drainage device combined with cataract surgery: Stent-type MIGS where iStent inject W or Hydrus is placed in Schlemm’s canal.
External approach (trabeculotome)
Approach: ab externo (conjunctival incision, scleral flap creation)
Technique: After miosis with pilocarpine eye drops, the limbal conjunctiva is incised to expose the sclera. A 4 mm scleral flap is created, and Schlemm’s canal is identified and its outer wall incised. A U-shaped metal probe (trabeculotome, curvature diameter 13-17 mm) is inserted into Schlemm’s canal and rotated to incise the inner wall of Schlemm’s canal and the trabecular meshwork. The scleral flap and conjunctiva are sutured with 10-0 nylon.
Features: Some facilities use a double scleral flap technique. Simultaneous performance with cataract surgery improves outcomes. Because conjunctival incision is required, it may affect future filtering surgery.
Intraocular method (MIGS outflow reconstruction)
Approach: ab interno (clear corneal incision, conjunctival sparing)
Procedure: After cataract surgery, inject ophthalmic viscosurgical device. Tilt the patient’s face 35° away from the surgeon and tilt the microscope 35°. Under gonioscopy, identify the trabecular meshwork and insert a microhook (μ-hook) or KDB into the anterior chamber. Incise the trabecular meshwork approximately 120° using the scleral spur as a guide. Remove reflux bleeding from Schlemm’s canal with I/A, then reform the anterior chamber and finish.
Features: No surgical scar on the conjunctiva, preserving filtration surgery. High reliability and safety due to direct visualization1).
Intraocular drainage (stent-type MIGS)
Approach: ab interno (corneal incision, conjunctival sparing)
Procedure (iStent inject W): Insert the inserter through the corneal incision, press the trocar against the trabecular meshwork, and release two bullet-shaped titanium stents using the release button. Confirm reflux bleeding2).
Procedure (Hydrus): Place an 8 mm crescent-shaped nitinol device into Schlemm’s canal over approximately 90° using a delivery system. It acts as a scaffold that dilates Schlemm’s canal 4 to 5 times9).
Features: Combined with cataract surgery is the principle, but iStent inject W has been approved for standalone surgery since July 20242).
This procedure uses a high-frequency electrode to electrocoagulate and incise the inner wall of Schlemm’s canal and the trabecular meshwork (FDA approved in 2004). A handpiece with built-in irrigation and aspiration is inserted through a 1.6 mm corneal incision. While protecting adjacent tissue with a footplate, output starts at 0.8 mW and treats up to 180° of the trabecular meshwork. Thermal conduction to the outer wall is minimized to about 1.2°C. No viscoelastic material is used. Postoperative outcomes are comparable to trabeculotomy, and concurrent cataract surgery improves results. A meta-analysis (5,091 patients) reported 2-year success rates of 46% for standalone and 85% for combined CE-IOL4). Hyphema occurs in up to 100% of cases but resolves within a few days in most 5).
This procedure involves inserting a microcatheter or Prolene suture into Schlemm’s canal and incising the trabecular meshwork circumferentially (360°). It was reported by Fellman and Grover in 2014. Using a suture allows for a low-cost implementation.
The technique first opens Schlemm’s canal via goniotomy, then inserts a catheter or suture into the canal and passes it around the full circumference. The trabecular meshwork is then incised by pulling the device centripetally. Postoperative management requires maintaining intraocular pressure at 30 mmHg or higher.
A meta-analysis (537 eyes) showed a mean IOP reduction of 9.81 mmHg and a decrease of 1.67 medications 4). Complications included hyphema (12.5–80.6%), IOP spike (1.9–32.3%), and transient hypotony (4.5–6.5%) 4). Ciliochoroidal detachment was detected by anterior segment OCT in 47.7% of cases, but most were asymptomatic and resolved spontaneously 4).
Comparison between 180° (hemi-GATT) and 360° procedures suggests that the dose-response threshold is reached at 120–180°, with the advantage of preserving the remaining area for future re-intervention. The inferior segment tends to have higher outflow pathway activity.
A flexible microcatheter is inserted twice at 180° each, performing viscodilation of Schlemm’s canal and trabeculotomy with a single device. In the GEMINI Study, 84.2% achieved ≥20% IOP reduction at 1 year 4).
This technique uses an iTrack microcatheter to dilate Schlemm’s canal and collector channels circumferentially (360°) with viscoelastic material. It does not incise the trabecular meshwork but improves pathological changes (collapse) of the lumen 4).
QWhich procedure should I choose?
A
The choice of surgical procedure depends on the type and severity of glaucoma, whether cataract surgery is performed simultaneously, and the surgeon’s experience. Meta-analyses indicate that trabeculotomy/trabeculectomy procedures (such as KDB, GATT) are superior to stent-type procedures (such as iStent) in lowering intraocular pressure and reducing medication 5), but the safety profile also differs by procedure. Outflow reconstruction surgery yields particularly good results in exfoliation glaucoma and steroid-induced glaucoma. Please consult with your ophthalmologist to select the optimal procedure.
3. Indications, Selection Criteria, and Contraindications
Surgical treatment for glaucoma is performed to lower intraocular pressure1). Indications include cases where sufficient intraocular pressure reduction cannot be achieved with medication or laser therapy, or cases where adequate pressure reduction is not expected due to side effects or poor adherence to medication 1).
Outflow reconstruction surgery (trabeculotomy/MIGS) is now performed at an earlier stage than trabeculectomy1).
Secondary childhood glaucoma: Trabeculotomy is indicated as in primary childhood glaucoma
Developmental glaucoma (primary childhood glaucoma): Trabeculotomy is the first choice in children where postoperative management of filtering blebs is difficult. Onset after 2 months of age shows a success rate of 96%, indicating good outcomes
Neovascular glaucoma / glaucoma secondary to uveitis: Pathological changes in the trabecular meshwork are significant, and the response rate to outflow reconstruction surgery is low, so it is generally not indicated
Selection Criteria for Intraocular Drainage Devices Combined with Cataract Surgery 2)
Need for conjunctival preservation: When future filtration surgery needs to be preserved, ab interno or stent-type procedures that do not incise the conjunctiva are advantageous.
Presence of cataract: In cases with cataract, combined surgery is standard, and the use of an intraocular drainage device is possible.
Surgeon experience: Sufficient experience in angle surgery is required, and it should be strictly avoided to perform it casually 1).
Tolerance for hyphema: iStent has been reported to cause less hyphema than blade-based procedures, and intraocular drainage devices may be an option in cases where postoperative hyphema should be avoided 2).
Angle-closure glaucoma: The angle is closed and not suitable for outflow reconstruction (however, there has been a recent trend toward expanding indications 3)).
Diseases with elevated episcleral venous pressure (e.g., Sturge-Weber syndrome): Trabecular MIGS is contraindicated because the effect is limited by episcleral venous pressure.
Glaucoma with congenital angle abnormalities: The angle structure is unclear, and the safety of stent placement cannot be guaranteed.
Neovascular glaucoma: Neovascularization of the trabecular meshwork impairs the effect of outflow reconstruction, resulting in a low response rate.
This procedure is performed by physicians who have performed at least 100 cataract surgeries and at least 10 incisional glaucoma surgeries, and who have completed training courses provided by each company 2).
QCan it be performed at the same time as cataract surgery?
A
Many MIGS procedures can be performed simultaneously with cataract surgery (lens reconstruction), and combined surgery results in better intraocular pressure reduction and lower reoperation rates than MIGS alone 6). iStent inject W and Hydrus are generally used in combination with cataract surgery, but iStent inject W has been approved for standalone surgery since July 2024 2). Microhook, KDB, GATT, and Trabectome can be performed alone, but simultaneous surgery is standard in cases with cataract. Please consult your ophthalmologist.
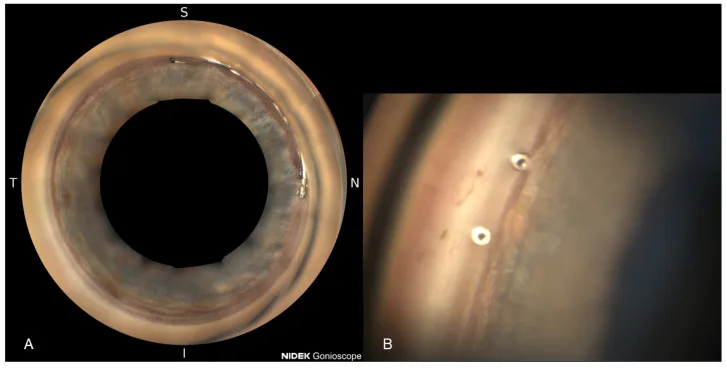
Weich C, Zimmermann JA, Storp JJ, Merté R-L, Eter N, Brücher VC. Comparison of the Intraocular Pressure-Lowering Effect of Minimally Invasive Glaucoma Surgery (MIGS) iStent Inject W and Hydrus—The 12-Month Real-Life Data. Diagnostics. 2025;15(4):493. Figure 1. PMCID: PMC11854837. License: CC BY 4.0.
A is a full-circle gonioscopic image (NIDEK GS-1) after Hydrus placement, showing the proximal end of the stent on the nasal side. B is a close-up gonioscopic image confirming the two-port openings of iStent inject W within the trabecular meshwork. This corresponds to the device position evaluation and postoperative gonioscopy discussed in the section “Treatment Outcomes and Complications.”
Postoperative intraocular pressure often ranges between 16 and 20 mmHg. For primary open-angle glaucoma, the expected intraocular pressure after trabeculotomy alone is 18 mmHg at 5 years postoperatively, and the rate of control to 20 mmHg or lower is about 50% at 5 years. Compared to trabeculectomy, intensive postoperative management that affects outcomes is not required, and advantages include faster visual recovery, less induced astigmatism, and fewer higher-order aberrations.
Simultaneous surgery with cataract surgery (lens reconstruction) improves the outcomes of trabeculotomy, so combined surgery is often chosen in cases with concurrent cataract.
Primary congenital glaucoma: Expected intraocular pressure is 17–18 mmHg at 18 years postoperatively. Success rate is 96% for onset after 2 months of age. However, prognosis is poor when associated with Axenfeld-Rieger syndrome or Sturge-Weber syndrome, or when corneal diameter exceeds 13 mm.
Developmental glaucoma overall: Goniotomy for early-onset type (1–2 years of age) has a success rate of 94%. For onset before 1 month or after 2 years of age, the success rate drops to 38%.
Overall, MIGS achieves a 15–50% reduction in intraocular pressure (IOP) and reduces the number of medications by 0.4–1.8 agents 6). When combined with cataract surgery, it provides an additional IOP reduction of 2–2.8 mmHg compared to cataract surgery alone, and the reoperation rate at 2 years is significantly lower (3% vs. 24%) 6). In some series, 22.6–80% of patients achieve medication freedom 6).
A meta-analysis (875 eyes, 23 studies) reported a weighted mean IOP reduction of 7.71 mmHg (95% CI: 5.16–10.26) and a medication reduction of 1.57 agents (95% CI: 1.17–1.96) at 1 year 5). Subgroup analysis showed that ab interno trabeculotomy (AIT) was significantly superior to iStent and endoscopic cyclophotocoagulation in both IOP reduction (p<0.02) and medication reduction (p<0.01) 5).
Because cataract surgery itself also has an IOP-lowering effect, it is difficult to completely separate the pure effect of MIGS from that of cataract surgery 3)7). Based on RCT results, approximately two-thirds of the IOP reduction and medication reduction in the CE-IOL+MIGS group are attributed to CE-IOL alone, and the additional effect of MIGS is estimated to be about one-third 4).
Outcomes of Stent-Type Devices
iStent inject W + CE-IOL: At 24 months, 75.8% achieved ≥20% IOP reduction (CE-IOL alone: 61.9%, p=0.005) 8)
Hydrus vs. iStent (COMPARE trial, standalone surgery): Cumulative success rate for IOP ≤18 mmHg was 35.6% for Hydrus vs. 10.5% for iStent (p=0.001). Medication-free rate: 46.6% vs. 24.0% 10)
Outcomes of Trabeculotomy/Trabeculectomy
KDB + CE-IOL vs. iStent + CE-IOL: 1-year success rate 93.7% vs. 83.3% (p=0.04). Mean IOP 15.4 vs. 16.1 mmHg 11)
Microhook + CE-IOL vs. CE-IOL alone: IOP reduction rate 51.5% vs. 20.1% (p<0.001). Complete success rate 90.3% vs. 0% 12)
Trabectome (meta-analysis, 5,091 patients): Success rate 46% for standalone, 85% for combined with CE-IOL (2 years) 4)
MIGS overall has a better complication profile than conventional filtration surgery5). Meta-analyses report no hypotony, diplopia, or infection, and all types of MIGS are safe5).
Incorrect insertion of the trabeculotome: Early perforation that occurs when accurate insertion into Schlemm’s canal is difficult
Ciliary body detachment: The probe enters the suprachoroidal space
Descemet’s membrane detachment/hematoma
Hyphema: Inevitable with perforation of the inner wall of Schlemm’s canal, but usually resolves spontaneously within 2-3 days. If high intraocular pressure persists, anterior chamber washout is performed due to the risk of corneal blood staining.
For Hydrus, UGH (uveitis-glaucoma-hyphema) syndrome presenting with iritis, cystoid macular edema, hyphema, and high intraocular pressure due to malposition has been reported 13). Since removal becomes difficult due to adhesion of iris tissue after 6 months or more post-placement, early recognition of abnormalities is important 13).
Two cases of ciliochoroidal detachment and persistent hypotony (1-4 mmHg, lasting more than 2 months) after microhook trabeculotomy have been reported. Both cases resolved with vitrectomy and gas tamponade14). Additionally, a case has been reported where ciliary body detachment after microhook closed spontaneously after 5 months, and at the time of closure, acute intraocular pressure elevation (42 mmHg) was observed, followed by normalization. Anterior segment OCT (AS-OCT) was superior to gonioscopy in detecting ciliary body detachment, demonstrating the usefulness of AS-OCT for postoperative angle evaluation.
QAre MIGS complications serious?
A
Complications of MIGS are generally mild and transient. Hyphema is the most common, but it usually resolves spontaneously within a few days. Serious complications such as hypotony, infection, and diplopia, which are concerns in conventional surgery, are rarely reported with MIGS5). However, additional surgery may be required due to device malposition. After surgery, follow your doctor’s instructions and attend regular check-ups.
5. Preoperative examination and postoperative management
Hyphema: Inevitable due to perforation of the inner wall of Schlemm’s canal. Causes visual disturbance immediately after surgery, but most resolve in 2–3 days and are absorbed spontaneously within 2 weeks. If high IOP persists due to bleeding, anterior chamber washout is performed because of the risk of corneal blood staining (irreversible hemoglobin deposition in the corneal stroma)
IOP spike: High IOP ≥30 mmHg may persist up to 3 months postoperatively. This phenomenon is called an “IOP spike.” The following medications are used:
Pilocarpine 1–2% eye drops (opens the angle by miosis)
Induced astigmatism: Astigmatism may occur due to creation of the scleral flap. Intraocular methods (MIGS) have the advantage of less induced astigmatism and fewer higher-order aberrations
Postoperative eye drops: Antibiotic and steroid eye drops are used for about 1–2 months
Postoperative management of intraocular procedures (MIGS)
Postoperative management is similar to that for cataract surgery 1). Intensive postoperative care that determines surgical outcomes, such as after trabeculectomy, is not required, and visual recovery is rapid.
Antibiotic eye drops such as levofloxacin: 3 times daily
Nonsteroidal anti-inflammatory drug (NSAID) eye drops such as diclofenac: 3 times daily
Steroid eye drops such as 0.1% betamethasone: 3 times daily
Anterior chamber hemorrhage is almost inevitable, but in many cases it improves within a few days to several days.
Regular examinations are performed at 1 day, 1 week, 1 month, 3 months, 6 months, and 1 year postoperatively.
Postoperative management of intraocular drainage devices
Long-term safety of the device is evaluated by corneal endothelial cell count (based on the precedent of CyPass Micro-Stent withdrawal from the market, special attention should be paid to changes in the corneal endothelium over time).
The position of the stent is confirmed by gonioscopy (early detection of malposition is important).
A patient card is issued, and the importance of postoperative follow-up is explained.
The presence of device obstruction or peripheral anterior synechiae (PAS) is regularly evaluated.
6. Pathophysiology: Mechanism of aqueous humor outflow and principle of action
Aqueous humor is produced by the ciliary body, flows from the posterior chamber through the pupil into the anterior chamber. There are two main outflow pathways from the anterior chamber.
Trabecular outflow pathway (conventional pathway) is the main route, accounting for approximately 80-90% of total aqueous outflow, and passes through the following structures in order.
Trabecular meshwork: three-layer structure consisting of uveal meshwork, corneoscleral meshwork, and juxtacanalicular tissue. In open-angle glaucoma, the extracellular matrix in the juxtacanalicular tissue increases, leading to elevated outflow resistance.
Schlemm’s canal: a ring-shaped lymphatic-like structure with an inner diameter of approximately 200-400 μm. Elevated intraocular pressure causes the canal lumen to collapse, further increasing outflow resistance.
Collector channels: approximately 25-35 channels branch from Schlemm’s canal and lead outward. The distribution of collector channel openings is uneven, and outflow capacity varies by location.
Episcleral veins: ultimately merge into the venous system. Episcleral venous pressure is approximately 8-10 mmHg, which defines the theoretical lower limit of intraocular pressure reduction by MIGS.
Uveoscleral outflow pathway (unconventional pathway) is a route that passes through the ciliary muscle interstices into the suprachoroidal space, accounting for approximately 10-20% of total aqueous outflow.
The majority of aqueous outflow resistance resides in the juxtacanalicular tissue and the inner wall of Schlemm’s canal. In open-angle glaucoma, resistance at this site is pathologically increased, and all MIGS procedures lower intraocular pressure by directly or indirectly reducing this resistance.
Ab externo approach (trabeculotome): The outer wall of Schlemm’s canal is exposed, and a probe is rotated to break through the inner wall into the anterior chamber, incising the trabecular meshwork. This method physically accesses Schlemm’s canal from the scleral side.
Ab interno approach (microhook, KDB): The trabecular meshwork and inner wall of Schlemm’s canal are incised or excised in a strip under direct gonioscopic visualization from the anterior chamber. This directly removes the main site of outflow resistance.
Trabectome: A high-frequency electrode ablates and removes the trabecular meshwork, exposing Schlemm’s canal.
GATT: Schlemm’s canal is incised over 240-360 degrees using a suture or catheter. This allows extensive opening of the outflow pathway.
Stent (iStent inject W): A titanium stent is placed within the trabecular meshwork, creating a bypass pathway from the anterior chamber to Schlemm’s canal.
Hydrus: An 8-mm nitinol scaffold dilates Schlemm’s canal approximately 4-5 times over about 90 degrees, maintaining patency of the canal lumen.
ABiC: A viscoelastic substance dilates Schlemm’s canal and collector channels 360°, improving luminal collapse. Trabecular meshwork is not incised.
The IOP-lowering effect of MIGS targeting the trabecular meshwork is limited by distal outflow resistance beyond Schlemm’s canal and episcleral venous pressure (approximately 8–10 mmHg) 3). Therefore, postoperative IOP rarely drops below the mid-teens (around 15 mmHg) 3). According to the Hagen-Poiseuille law, flow within the lumen is proportional to the fourth power of the inner diameter and inversely proportional to length, so the stent lumen diameter and the extent of trabecular incision are key factors determining flow.
In contrast, filtering surgeries (trabeculectomy and tube shunt) drain aqueous humor to the subconjunctival space, bypassing the limitation of episcleral venous pressure, and can achieve lower target IOP (≤10 mmHg). This is the theoretical basis for why MIGS may be insufficient for advanced glaucoma requiring low target IOP.
The effect of trabeculotomy depends on the extent of incision, but beyond 120–180°, a dose-response plateau is reached. Aqueous outflow is not uniform around the entire angle; outflow pathway activity is particularly high in the nasal and inferior segments. The distribution density of collector channels also varies by location, and selective incision of segments rich in outflow pathways can achieve efficient IOP reduction. Therefore, a 180° procedure (e.g., hemi-GATT) may provide sufficient effect.
In all glaucoma surgeries including MIGS, the IOP-lowering effect tends to diminish over time 3). Stent-type devices may develop peripheral anterior synechiae or device obstruction. In trabeculotomy, fibrovascular membrane formation or scarring due to inflammatory response may cause restenosis at the incision site. Therefore, glaucoma is a lifelong disease and cannot be cured by a single surgery 3). An important advantage of MIGS is that it does not involve conjunctival incision, thus preserving the success rate of future filtering surgeries (trabeculectomy or tube shunt) 3).
Pilocarpine is one of the oldest IOP-lowering medications, but it is sometimes used after MIGS to maintain outflow effect, and it plays an important role in the management after minimally invasive glaucoma surgery. 1–2% pilocarpine eye drops are thought to maintain angle opening in the early postoperative period and contribute to early resolution of hyphema.
The reporting methods for clinical endpoints in MIGS studies have not been standardized, making comparisons between different studies difficult 4). The AAO Glaucoma PPP Committee recommends using the cumulative success rate from Kaplan-Meier survival analysis at 2 years as the primary endpoint 4).
Success criteria for standalone MIGS: Intraocular pressure ≤21 mmHg and ≥20% reduction from baseline, no increase in glaucoma medications, no additional surgery, no loss of light perception, no hypotony 4)
Success criteria for CE-IOL combined MIGS: Reduction of at least one medication (without intraocular pressure increase), or intraocular pressure ≤21 mmHg and ≥20% reduction 4)
The minimal clinically important difference (MCID) for the 2-year cumulative success rate has been proposed as ≥50% for standalone MIGS and ≥65% for CE-IOL combined MIGS4).
Traditionally, angle-closure glaucoma was considered a contraindication for MIGS, but this view is changing in recent years based on the idea that more patients could benefit from MIGS3).
Research on patient-reported outcomes after MIGS is limited, but preliminary findings suggest improvements in visual function, quality of life, and ocular surface health 6). Reducing medication burden may contribute to improved ocular surface and treatment adherence6).
A review of 40 studies found that 22.6–80% of patients became medication-free after combined MIGS-phacoemulsification, and reduction of ocular surface damage from eye drops (such as corneal epithelial damage, conjunctival hyperemia, and meibomian gland dysfunction) is thought to contribute to improved quality of life 6). Patients on multiple medications (≥3) particularly benefit from medication reduction after MIGS. Development of standardized patient-reported outcome measures and research in diverse racial populations are future challenges 6).
The CyPass Micro-Stent (suprachoroidal MIGS) was found to cause corneal endothelial cell loss after 5 years, leading to its voluntary withdrawal from the market in 2018 3). For MIGS in general, accumulation of data on long-term safety, cost-effectiveness, and medication-free rates remains a future challenge 3)7).
There is a report of KDB performed for juvenile open-angle glaucoma associated with Freeman-Sheldon syndrome, where intraocular pressure decreased from 40 mmHg to 10 mmHg and remained stable below 15 mmHg for 27 months. Expansion of MIGS beyond conventional indications to special disease types is being considered.
In combined KDB trabeculotomy and deep sclerectomy, cases have been reported where postoperative intraocular pressure dropped below the episcleral venous pressure, leading to massive hyphema and fibrin clots, resulting in peripheral anterior synechiae and collector channel obstruction. Caution is needed when combining procedures that significantly lower intraocular pressure; while KDB alone achieves a pressure reduction of approximately 28.4%, the combination group did not show a significant additional effect.
ELIOS: A new technology that uses a highly precise non-thermal laser to create 10 microchannels in the trabecular meshwork. The cold laser minimizes tissue fibrosis, and sustained intraocular pressure reduction over 8 years has been reported. At 1 year postoperatively, 80% of patients were able to discontinue medication.
MIMS (Minimally Invasive Mini-Sclerostomy): An ab externo filtering surgery without a stent, which permanently creates a scleral-corneal drainage channel using a 600 μm needle with a 300 μm triangular blade. Results are promising but still under investigation.
QIs reoperation necessary after MIGS?
A
The effect of MIGS may diminish over time, as with all glaucoma surgeries. Reports indicate that up to 24% of patients undergoing standalone MIGS required reoperation at 2 years 6). When combined with cataract surgery, the reoperation rate drops significantly to 3% 6). MIGS preserves the conjunctiva, so if additional surgeries such as trabeculectomy or tube shunt are needed in the future, their success rate is not compromised.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Vinod K, Bowden EC, Kolomeyer NN, Chopra V, Challa P, Budenz DL, Repka MX, et al. Special Commentary: Reporting Clinical Endpoints in Studies of Minimally Invasive Glaucoma Surgery. Ophthalmology. 2025;132(2):141-153. doi:10.1016/j.ophtha.2024.07.030. PMID:39127407.
Paik JM, et al. Outcomes and Complications of Minimally Invasive Glaucoma Surgery: A Systematic Review and Meta-Analysis. Clin Ophthalmol. 2025;19:487-503.
Singh P, Sharma B, Sarma N, Nag DS, Patnaik A, Verma R. Clinical Outcomes and Patient-Reported Outcomes of Minimally Invasive Glaucoma Surgery Techniques Over the Past Decade. Cureus. 2025;17(7):e87872. doi:10.7759/cureus.87872. PMID:40809659; PMCID:PMC12344473.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Samuelson TW, Sarkisian SR Jr, Lubeck DM, Stiles MC, Duh YJ, Romo EA, et al. Prospective, Randomized, Controlled Pivotal Trial of an Ab Interno Implanted Trabecular Micro-Bypass in Primary Open-Angle Glaucoma and Cataract: Two-Year Results. Ophthalmology. 2019;126(6):811-821. doi:10.1016/j.ophtha.2019.03.006. PMID:30880108.
Samuelson TW, Chang DF, Marquis R, Flowers B, Lim KS, Ahmed IIK, et al. A Schlemm Canal Microstent for Intraocular Pressure Reduction in Primary Open-Angle Glaucoma and Cataract: The HORIZON Study. Ophthalmology. 2019;126(1):29-37. doi:10.1016/j.ophtha.2018.05.012. PMID:29945799.
Ahmed IIK, Fea A, Au L, Ang RE, Harasymowycz P, Jampel HD, et al. A Prospective Randomized Trial Comparing Hydrus and iStent Microinvasive Glaucoma Surgery Implants for Standalone Treatment of Open-Angle Glaucoma: The COMPARE Study. Ophthalmology. 2020;127(1):52-61. doi:10.1016/j.ophtha.2019.04.034. PMID:31034856.
Falkenberry SM, et al. CE-IOL plus KDB vs CE-IOL plus iStent: 1-year multicenter RCT results. Ophthalmology. 2020.
Maheshwari D, et al. CE-IOL plus Tanito Microhook vs CE-IOL alone: a randomized single-center trial. 2023.
Sachdeva N, Sun LW, Young J, Chen A. Early to late explantation of Hydrus microstent MIGS device: A case series. American journal of ophthalmology case reports. 2024;36:102105. doi:10.1016/j.ajoc.2024.102105. PMID:39161375; PMCID:PMC11332841.
Otsuka M, et al. Gas Tamponade Improved Cilio-Choroidal Effusion Induced by an Ab Interno Trabeculotomy with a Microhook: Two Cases. Int Med Case Rep J. 2024;17:479-486. doi:10.2147/imcrj.s465485.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.