ECP is a type of cyclodestructive procedure developed by Martin Uram in 1992. Conventional transscleral approaches do not allow direct visualization of the ciliary body, leading to poor quantification of the degree of destruction. ECP uses a fiber-optic cable that integrates an 810 nm semiconductor diode laser, video camera, aiming beam, and 175 W xenon light source to directly visualize the ciliary processes from inside the eye and treat them2). This enables more precise titration of laser treatment2).
The efficacy of ECP is good, with intraocular pressure reduction rates of 34–57% reported2). Most studies treat 270–360 degrees of the ciliary body2). As of 2005, 47% of Medicare cyclophotocoagulation procedures were ECP, increasing to 77% by 20122).
Indications for cyclophotocoagulation include cases where filtration surgery or drainage devices are unlikely to succeed, have failed, or cannot be performed, with refractory glaucoma being the main target1). However, in recent years, its use has increased in cases with less severe glaucoma.
ECP (Endoscopic Method)
Irradiation route: Direct visualization of ciliary processes from inside the eye 2)
Tissue damage: Localized shrinkage limited to ciliary processes. Partial reperfusion after 1 month
Complication risk: Lower risk of hypotony and phthisis bulbi compared to TSCPC
Expanded indications: Can be used for mild to moderate glaucoma when combined with cataract surgery
TSCPC (Transscleral approach)
Irradiation route: Transscleral. Ciliary body cannot be directly visualized
Tissue damage: Severe destruction of ciliary processes and iris root. Persistent occlusive vascular damage
Complication risk: Higher risk of hypotony and phthisis bulbi
Indications: Mainly eyes with poor visual prognosis or not candidates for incisional surgery 2)
QWhat is the difference between ECP and transscleral cyclophotocoagulation (TSCPC)?
A
The biggest difference is whether visualization is possible. ECP uses an endoscope to directly visualize the ciliary processes while delivering laser, resulting in higher treatment precision and less damage to surrounding tissues. Histological studies show that TSCPC causes severe destruction of the ciliary processes and iris root, whereas ECP produces localized shrinkage only in the ciliary processes, with partial blood flow recovery after one month. Therefore, ECP is associated with a lower risk of serious complications such as hypotony and phthisis bulbi. However, ECP requires specialized equipment and intraocular manipulation via a corneal limbal or pars plana approach.
Since ECP is a treatment for glaucoma, target patients have visual field defects due to glaucoma. After ECP, transient blurred vision, eye pain, and redness may occur.
Preoperative findings: Elevated intraocular pressure, enlarged optic disc cupping, visual field defects. Gonioscopy and assessment of lens and vitreous status are important for determining ECP indication.
Intraoperative findings: Whitening and shrinkage of the ciliary processes are indicators of optimal treatment effect. Laser is applied with continuous wave at 100–300 mW.
Postoperative findings: Postoperative intraocular pressure spike (due to retained viscoelastic) occurs in 14.5% of cases. Hyphema 3.8%, choroidal detachment 0.36%, cystoid macular edema 0.7%.
Since ECP is a treatment, this section describes risk factors for complications.
Advanced glaucoma: Severe complications (retinal detachment 0.2%, choroidal hemorrhage 0.09%, hypotony 0.12%, no light perception 0.12%) all occurred in eyes with neovascular glaucoma. These complications have not been reported in POAG or pseudoexfoliation glaucoma.
Overtreatment: Excessive energy delivery to the ciliary body increases the risk of phthisis bulbi. If destruction is excessive, it may lead to phthisis.
Choice of viscoelastic: Healon 5 provides excellent space maintenance but may increase the risk of early postoperative IOP spike. Dispersive viscoelastics have poor space maintenance and absorb laser energy.
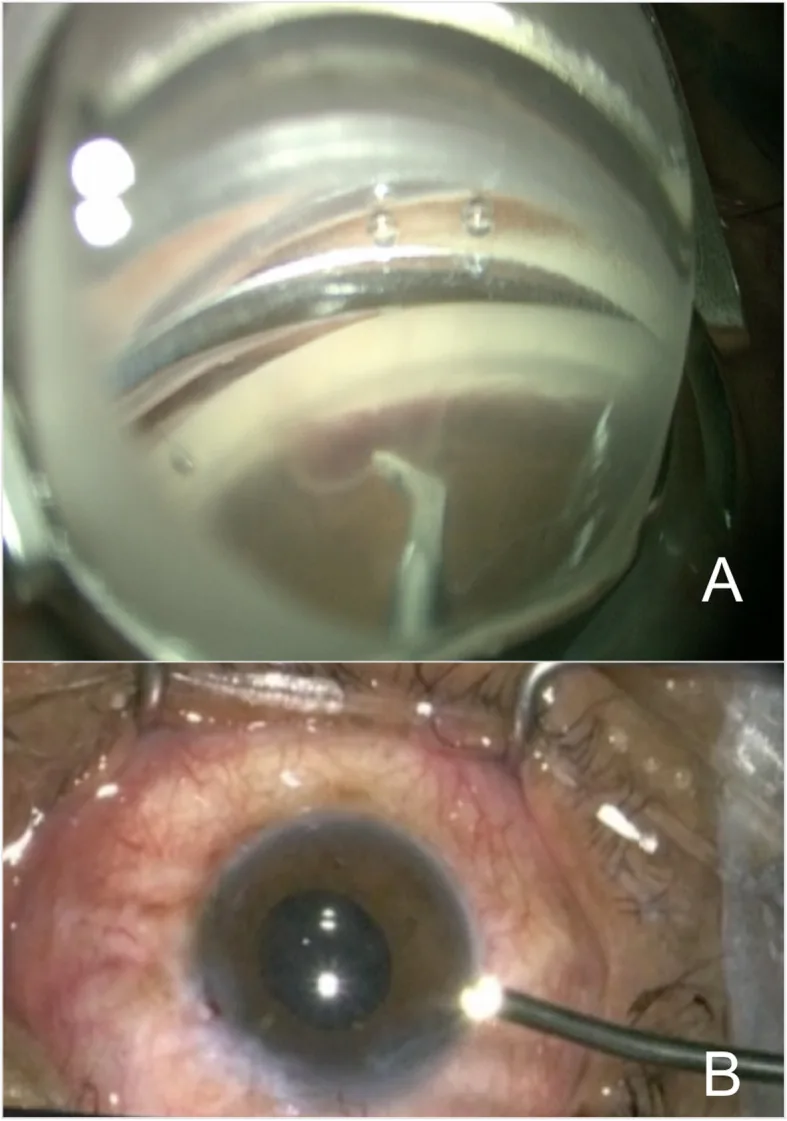
Izquierdo JC, Mejías J, Cañola-R L, et al. Primary outcomes of combined cataract extraction technique with Ab-Interno trabeculectomy and endoscopic Cyclophotocoagulation in patients with primary open angle Glaucoma. BMC Ophthalmol. 2020;20(1):406. Figure 2. PMID: 33036581; PMCID: PMC7545548; DOI: 10.1186/s12886-020-01643-2. License: CC BY.
The upper panel shows the ciliary processes visualized under endoscopy, and the lower panel shows the actual procedure. This intraoperative photograph helps readers understand the flow of ECP.
Limbal approach: Common for ECP combined with cataract surgery. Insert the endoscope through a 1.5–2.2 mm incision. Both clear corneal incision and scleral tunnel incision can be used.
Pars plana approach: Considered in pseudophakic eyes. Allows the most complete visualization of ciliary processes, but requires concurrent anterior vitrectomy.
Stabilize the anterior chamber with an ophthalmic viscosurgical device (OVD) to deepen the ciliary sulcus. Cohesive OVDs (Healon, Healon GV) are optimal.
Position the 18–23 gauge endoscope probe approximately 2 mm from the ciliary processes.
Apply 810 nm semiconductor diode laser at 100–300 mW in continuous wave mode.
Systematically coagulate each ciliary process until whitening and shrinkage are observed.
At least 270 degrees of treatment is required for optimal intraocular pressure reduction. 360-degree treatment is more effective when performed through two incisions.
For refractory cases where multiple glaucoma surgeries have failed, this technique extends the treatment area 1–2 mm to the pars plana via a pars plana approach. Vitrectomy is required, and pseudophakic or aphakic eyes are indicated. At 2 years postoperatively, intraocular pressure decreased from 27.9±7.5 mmHg to 11.1±6.5 mmHg, and the number of medications decreased from 3.4±1.2 to 0.6±1.3, but hypotony was reported in about 7.5%, which is higher than standard ECP.
ECP can be performed through the same corneal limbal incision as cataract surgery (phacoemulsification), so it is widely used as a combined procedure2).
Outcome
phaco-ECP
Phaco alone
IOP change (final visit)
MD −1.49 mmHg
Reference
Medication change (final visit)
MD −0.75 medications
Reference
In a 2024 meta-analysis (9 studies, 5,389 eyes), the phaco-ECP group consistently had lower intraocular pressure and fewer medications at all time points compared to the phaco-alone group3). However, best-corrected visual acuity was slightly better in the phaco-alone group (MD 0.09 logMAR)3). Complication rates were significantly higher in the phaco-ECP group for both general complications (OR 3.96) and serious complications (OR 8.82)3).
Advantages of phaco-ECP
IOP reduction: MD −1.84 mmHg at 6 months, MD −1.68 mmHg at 12 months3)
Reduction of medication burden: At the final visit, MD −0.75 medications 3)
Simplicity of procedure: Can be performed through the same incision as cataract surgery 2)
Precautions for phaco-ECP
Increased complication rate: General complications OR 3.96, serious complications OR 8.82 3)
Visual prognosis: The phaco-alone group had slightly better final BCVA 3)
Long-term efficacy: In a 6-year analysis, 68% required additional intervention
During the perioperative period, broad-spectrum antibiotic eye drops, steroid eye drops (1% prednisolone acetate or difluprednate), and NSAID eye drops are used. Glaucoma medications (eye drops or oral) may be added to prevent early postoperative intraocular pressure spikes. Glaucoma medications are tapered 1–2 months after surgery depending on intraocular pressure levels and targets.
Postoperatively, pain management is considered, and steroid eye drops and atropine eye drops are used as needed 1). Intraocular pressure is monitored immediately after surgery, and antiglaucoma medications are adjusted accordingly 1).
QWhich patients are suitable for combined cataract surgery and ECP?
A
Patients with visually significant cataract and mild to moderate glaucoma are good candidates. It is particularly useful when the patient is using two or more glaucoma eye drops and a reduction in medication burden is desired. Meta-analyses have shown sustained effects in lowering intraocular pressure and reducing the number of medications, but the complication rate is higher than with phaco alone, so careful individual risk-benefit assessment is necessary. For refractory glaucoma, ECP Plus may be considered, but caution is needed due to the increased risk of hypotony.
ECP destroys the ciliary epithelium, which produces aqueous humor, through laser photocoagulation, reducing aqueous humor production and thereby lowering intraocular pressure. The 810 nm diode laser is absorbed by the ciliary epithelium, causing tissue whitening and contraction.
In angle-closure glaucoma, endoCPG is thought to have a dual effect: suppressing aqueous humor production and widening the angle recess 4). However, meta-analyses show that endoCPG is inferior to ab interno trabeculotomy (AIT), possibly due to insufficient treatment extent 4). At least 270 degrees of treatment is required for significant IOP reduction 4).
Histological studies show that TSCPC causes severe destruction of the ciliary processes and iris root, with occlusive vascular damage persisting for up to one month. In contrast, ECP causes localized contraction only in the ciliary processes, with partial reperfusion observed after one month. This partial blood flow recovery is thought to explain why ECP is less likely to cause hypotony or phthisis compared to TSCPC.
A common drawback of all cyclophotocoagulation procedures is that insufficient destruction fails to lower intraocular pressure, while excessive destruction can lead to phthisis; the procedure lacks quantifiability. The need for retreatment is high, with retreatment rates of 0–59% reported for transscleral methods.
The 2024 meta-analysis by Amaral et al. (9 studies, 5,389 eyes) is the first meta-analysis comparing phaco-ECP with phaco alone 3). The phaco-ECP group showed superior IOP reduction and medication reduction at all time points, but had a significantly higher complication rate 3).
Outcome
Result (MD/OR)
P value
IOP at 6 months
−1.84 mmHg
0.002
IOP at 12 months
−1.68 mmHg
0.0002
Number of medications (final)
−0.75 medications
<0.00001
Serious complications
OR 8.82
0.03
In the MIGS meta-analysis for PACG, adverse events were reported in 27 of 156 eyes (17.3%) with endoCPG 4). These included 4 cases of cystoid macular edema, 11 cases of fibrinous uveitis, 1 case of hemorrhagic choroidal detachment, 2 cases of secondary pupillary block, and 1 case of malignant glaucoma4).
A 2019 Cochrane review concluded that there was insufficient evidence to determine whether cyclodestructive procedures for refractory glaucoma result in better outcomes or fewer complications compared to other treatments 2). No studies on ECP for open-angle glaucoma were identified 2). Additional RCTs are needed to compare different types of cyclophotocoagulation and to compare them with other glaucoma surgeries 2).
Regarding the long-term efficacy and safety of ECP, a 6-year analysis reported that 68% required additional interventions. Long-term RCTs comparing ECP with TSCPC or trabeculectomy are still lacking. The choice of cyclophotocoagulation procedure is left to the discretion of individual surgeons 2).
A novel application of the ECP probe is the ablation of collector channels for recurrent hyphema after trabeculotomy, as reported in one study 5).
QWhat is the long-term effectiveness of ECP?
A
In a 3-year study of ECP combined with cataract surgery, the success rate (IOP ≤21 mmHg, ≥20% reduction, no additional surgery) decreased over time: 70% at 1 year, 54% at 2 years, and 45% at 3 years. A 6-year analysis showed that 68% required additional intervention. In contrast, ECP Plus for refractory glaucoma achieved a 60% IOP reduction at 2 years with a significant decrease in medication number. Long-term effectiveness varies widely among cases, and no direct RCT comparing ECP with TSCPC or trabeculectomy exists, so further research is needed.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. PMID:41026937. doi:10.1136/bjophthalmol-2025-egsguidelines.
2. Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
3. Amaral DC, Louzada RN, Moreira PHS, de Oliveira LN, Yuati TT, Guedes J, et al. Combined Endoscopic Cyclophotocoagulation and Phacoemulsification Versus Phacoemulsification Alone in the Glaucoma Treatment: A Systematic Review and Meta-Analysis. Cureus. 2024;16(3):e55853. doi:10.7759/cureus.55853. PMID:38590498; PMCID:PMC11001325.
4. Paik JS, et al. Outcomes and Complications of Minimally Invasive Glaucoma Surgery in Primary Angle Closure Glaucoma: A Systematic Review and Meta-Analysis. Clin Ophthalmol. 2025;19:493-502.
5. Gallardo MJ, Reyes T. A novel use of the endoscopic cyclophotocoagulative probe for the management of excisional goniotomy induced chronic recurrent hyphema. American journal of ophthalmology case reports. 2022;26:101492. doi:10.1016/j.ajoc.2022.101492. PMID:35340745; PMCID:PMC8943413.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.