Cystoid Macular Edema (CME) is a condition in which breakdown of the blood-retinal barrier (BRB) causes fluid leakage from capillaries in the macular area (around the fovea), leading to cystoid fluid accumulation mainly in the outer plexiform layer and inner nuclear layer. The cyst walls are composed of Müller cells and nerve axon fibers, and fluid accumulation along the Henle fiber layer forms a characteristic petaloid pattern.
It is one of the leading causes of central vision loss in developed countries and can be caused by various ocular diseases, systemic diseases, and medications. CME involves three basic mechanisms: (1) exudative (vascular leakage due to BRB breakdown), (2) degenerative (intracellular fluid accumulation due to Müller cell dysfunction), and (3) tractional (mechanical deformation due to vitreomacular traction or epiretinal membrane). 3)
Stratified localization of fluid on OCT provides clues for estimating the cause. Localization limited to the inner nuclear layer suggests a degenerative mechanism, limited to the outer nuclear layer suggests acute Müller cell edema or traction, and distribution across both layers suggests an exudative mechanism. 3)
QDoes cystoid macular edema resolve on its own?
A
In many cases, it resolves spontaneously within 3 to 4 months. However, if it becomes chronic (lasting 6 to 9 months or more), permanent damage to photoreceptors may occur. Identifying the cause and appropriate treatment intervention are important; for details, refer to the section on Standard Treatment.
Loss of the foveal reflex on slit-lamp examination is an important early finding. A central foveal thickness ≥300 μm is recognized as clinically significant edema. Green light (red-free) illumination enhances the outline of cysts.
On fundus examination, petaloid cysts are often observed in a honeycomb pattern centered on the fovea. In severe cases, cysts may coalesce to form large cysts.
The main causes of CME are organized by the mnemonic “DEPRIVENS”: Diabetes (diabetic retinopathy), Epinephrine, Pars planitis (intermediate uveitis), Retinitis pigmentosa, Irvine-Gass syndrome (post-cataract surgery), Vein occlusion, Nicotinic acid, External beam radiation, Surgery.
Post-cataract surgery CME is the most common type of postoperative CME. It occurs in up to 20% of eyes with IOL implantation, but only 1–20% are associated with visual loss. Posterior capsule rupture is a high-risk factor. Onset is most common 6–10 weeks after surgery, and 95% resolve spontaneously within 6 months. The incidence of CME after macular hole surgery is less than 10%. 14)
Onset even 10 years after discontinuation. Complicated in 17% of maculopathy10)
Prostaglandin analogs (PGAs) disrupt the blood-aqueous barrier and induce CME. In a review by Warwar et al. on latanoprost, 2.1% of 94 patients developed CME, and in a review by Hu et al., 47 of 48 eyes were pseudophakic or aphakic. 1) Onset in phakic eyes is rare, but cases after 22 years of long-term use have been reported. 1)
Retinal vein occlusion (RVO): Both branch and central vein occlusion frequently complicate CME. Hyperhomocysteinemia (23.3 μmol/L exceeding the normal range of 5–13 μmol/L) increases RVO risk via hypercoagulability and can directly damage the BRB, leading to CME. 6)
Central retinal artery occlusion (CRAO): In the acute phase, CME localized to the outer nuclear layer may occur and spontaneously resolve within two weeks. In the chronic phase, degenerative CME localized to the inner nuclear layer develops without FA leakage. 3)
QWhat is the probability of CME after cataract surgery?
A
CME (Irvine-Gass syndrome) occurs in up to 20% of eyes with IOL implantation, but only 1–20% actually develop vision loss. The risk is higher if the posterior capsule is ruptured. 95% resolve spontaneously within 6 months after surgery, but prophylactic NSAIDs are recommended for high-risk cases. 12)
QCan oral medications cause CME?
A
CME has been reported with fingolimod and siponimod (for multiple sclerosis), nab-paclitaxel (anticancer), ibrutinib (for blood cancers), and pentosan polysulfate (for interstitial cystitis). Discontinuation of the causative drug is the most effective treatment; for details, see the “Standard Treatments” section.
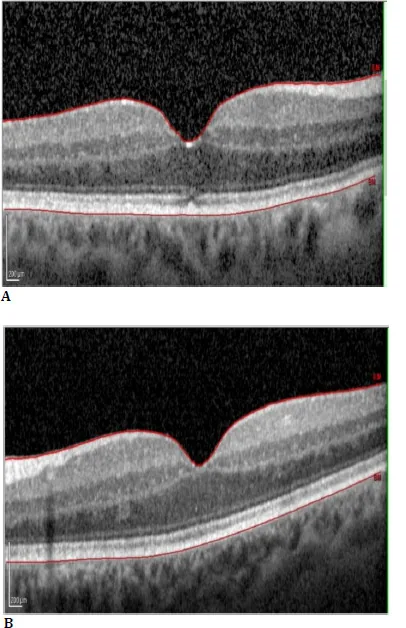
Radomir Babovic; Ben Burton; Nimesha Alex; Lakshmi Harihar; Tihomir Dugandzija. Unraveling the Mystery of Taxol-Induced Cystoid Macular Oedema: Case Report and Literature Review. Rom J Ophthalmol. 2025 Jan-Mar; 69(1):3-9. Figure 5. PMCID: PMC12049643. License: CC BY.
SD-OCT horizontal scan of the right eye (A) and left eye (B) shows complete resolution of the cystoid macular oedema after discontinuing paclitaxel treatment
Multiple imaging tests are used to diagnose CME. The main tests are listed below.
The most important examination method. It enables quantitative assessment of cyst location, distribution, and retinal thickness, and is essential for longitudinal monitoring of treatment response. There are three basic OCT findings in CME: (1) retinal swelling (diffuse), (2) cystoid edema (cyst formation), and (3) serous retinal detachment.
Layer-specific localization is useful for inferring the cause: inner nuclear layer involvement suggests a degenerative mechanism, while outer nuclear layer involvement suggests acute Müller cell edema. 3) En face OCT is useful for visualizing the distribution pattern of CME. 3)
A systematic review of OCT biomarkers for treatment response showed the following: 13)
Subretinal fluid improved in 67% of cases, intraretinal cysts improved in 76%, while EZ (ellipsoid zone) disruption remained unchanged or worsened in 64%, ELM (external limiting membrane) disruption remained unchanged or worsened in 67%, hyperreflective foci remained unchanged or worsened in 63%, and DRIL (disorganization of retinal inner layers) remained unchanged or worsened in 50%. 13)
The presence of EZ and ELM disruption is a poor prognostic biomarker indicating limited visual recovery after treatment. 13)
In the late phase (10–20 minutes), petaloid leakage along the Henle fiber layer is characteristic. However, in taxane-induced CME, FA leakage is often absent (due to a degenerative mechanism), so CME cannot be ruled out even with negative FA. 2)
In pentosan polysulfate (PPS)-associated maculopathy, a characteristic FAF abnormality pattern is observed, which is often initially misdiagnosed as AMD. 10)FAF is more useful for evaluating RPE damage than CME itself.
QWhat can OCT tell us?
A
It enables quantitative assessment of cyst location, distribution, size, and retinal thickness, and is essential for longitudinal evaluation of treatment response. Layer-specific localization (inner vs. outer nuclear layer) provides clues for inferring the cause. EZ and ELM disruption are evaluated as biomarkers affecting visual prognosis. 13)
Treatment is selected according to the underlying disease and pathology. For drug-induced CME, discontinuation of the causative drug is the first-line treatment.
Ketorolac 0.5%, nepafenac 0.1%, and bromfenac 0.07% are used. They inhibit cyclooxygenase (COX), suppressing prostaglandin production and stabilizing the blood-retinal barrier (BRB).
Perioperative prophylactic administration of NSAIDs is recommended for high-risk eyes (e.g., posterior capsule rupture, monocular, diabetic cases). Starting preoperative administration and continuing immediately after surgery promotes visual recovery. 12)
In a case of CME due to Hydrus Microstent bending, complete resolution (visual acuity 20/60 → 20/25) was reported after 2 months of ketorolac plus prednisolone eye drops. 9)
Sub-Tenon triamcinolone injection: Local anti-inflammatory effect. Multiple doses are often required.
Intravitreal triamcinolone injection: More direct drug delivery. Caution is needed for increased intraocular pressure and cataract progression.
Systemic steroids: Used for severe inflammatory CME, but side effect management is important with long-term administration.
Steroids are suggested to stimulate adenosine signaling in Müller cells, reducing VEGF production. In IRU-related CME where steroids are contraindicated (e.g., femoral head necrosis), tocilizumab may be an alternative (discussed later).
Main treatment for diabetic macular edema and RVO-related CME. Bevacizumab 1.25 mg/0.05 mL, ranibizumab 0.5 mg, aflibercept 2 mg, etc. are used.
Complete resolution of PPS-related CME has been reported after two injections of bevacizumab 1.25 mg/0.05 mL. A good outcome was achieved in this case where NSAIDs and steroid eye drops were ineffective. 10)
Improvement was also obtained with two anti-VEGF injections in a case of bilateral venous stasis and CME associated with hyperhomocysteinemia. 6)
Enhances RPE pump function and promotes absorption of subretinal fluid. Administered as eye drops (dorzolamide, brinzolamide) or orally (acetazolamide). In latanoprost-induced CME, switching from latanoprost to dorzolamide resulted in resolution within one month (CMT 319→218 μm, 326→227 μm). 1)
In drug-induced CME, discontinuation of the causative drug is the most effective treatment.
Latanoprost: Resolution within 1 month after discontinuation or switching. 1)
Fingolimod: May be continued while awaiting spontaneous resolution due to risk of MS worsening. Spontaneous resolution after 13 months has been reported. 8)
Siponimod: Marked improvement 1 week after discontinuation, complete resolution in 1 month. 4)
Nab-paclitaxel: Improvement 2 months after discontinuation of chemotherapy. Sub-Tenon triamcinolone was ineffective. 2)
Ibrutinib: Complete resolution 6 months after discontinuation (visual acuity 6/15 to 6/12). NSAIDs + steroid eye drops for 2 years only partial response. 7)
PPS: CME may develop even after discontinuation, with cases occurring up to 10 years later. 10)
In tractional CME with VMT, vitrectomy improves CME in 80–92% of cases. Ocriplasmin (enzymatic vitreolysis) showed VMT resolution within 1 month in 58% of patients in phase 2/3 trials.
QWhat are the treatment options for CME?
A
Depending on the cause, options include NSAIDs eye drops, steroids (sub-Tenon/intravitreal injection), anti-VEGF intravitreal injection, carbonic anhydrase inhibitors, and vitrectomy. In drug-induced CME, discontinuation of the causative drug is the most effective first-line treatment. For details, see the “Standard treatment” section.
The BRB consists of two layers: the inner BRB (tight junctions between retinal vascular endothelial cells) and the outer BRB (tight junctions between retinal pigment epithelial cells), which maintain retinal fluid homeostasis. When tight junctions are weakened by inflammation, ischemia, or toxic substances, serum proteins and lipids leak out, leading to increased osmotic pressure. 11)
Müller cells normally prevent fluid accumulation through a drainage mechanism using aquaporin-4 and Kir4.1 channels. When BRB breakdown becomes severe, this compensatory drainage mechanism becomes saturated, and CME becomes apparent. 11)
S1P receptor modulators (fingolimod, siponimod): They inhibit the regulation of vascular endothelial cadherin, increase vascular permeability, and disrupt the BRB. 4) In the EXPAND trial, CME occurred in 2% of the siponimod group (placebo group <1%). 4)
Ibrutinib (BTK inhibitor): Due to its ability to cross the blood-brain barrier (BBB), it is suggested that it may also disrupt the BRB. In a phase 3 trial, 10% of the ibrutinib group reported blurred vision (ofatumumab group 3%). 7)
Acute CRAO: Ischemia disrupts extracellular ion homeostasis, causing a rapid influx of ions into Müller cells. This increases the expression of aquaporin-4 and Kir4.1 channels, leading to Müller cell edema (limited to the outer nuclear layer). 3)
7. Latest Research and Future Perspectives (Investigational Reports)
Cases have been reported where tocilizumab was effective for CME secondary to immune recovery uveitis (IRU).
Nguyen et al. (2024) treated a 17-year-old female with CME due to CMV retinitis followed by IRU after treatment for T-cell acute lymphoblastic leukemia (systemic steroids contraindicated due to femoral head necrosis) with tocilizumab 8 mg/kg IV once monthly for 2 cycles. After 2 cycles, marked improvement in CME was observed. 5)
The STOP-UVEITIS trial showed that tocilizumab improves CME, and it is expected to be positioned as an alternative treatment in cases where steroids are contraindicated. This finding suggests that IL-6 is directly involved in CME pathogenesis. 5)
Long-term course of PPS-associated maculopathy and CME
PPS-associated maculopathy is a relatively new disease concept first recognized in 2018. Lesions may progress and CME may develop even more than 10 years after discontinuation of PPS, highlighting the importance of long-term follow-up. 10)
Szelog et al. (2023) reported a 57-year-old woman who developed CME 10 years after discontinuing PPS after 3 years of use. Initially misdiagnosed as AMD, she did not respond to NSAIDs or steroid eye drops, but complete resolution was achieved with two doses of bevacizumab 1.25 mg/0.05 mL. CME also developed in the fellow eye 5 months later. 10)
CME is reported to complicate 17% of PPS-associated maculopathy, and maculopathy occurs in over 10% of patients with cumulative use of 500 g or more. 10)
Studies systematically evaluating the treatment responsiveness of OCT findings have shown that the following biomarkers are useful for prognostic prediction. 13)
A 2025 systematic review published in Survey of Ophthalmology reported that intraretinal cysts (76% improvement) and subretinal fluid (67% improvement) showed high treatment responsiveness, while EZ disruption (64% unchanged/worsened), ELM disruption (67% unchanged/worsened), hyperreflective foci (63% unchanged/worsened), and DRIL (50% unchanged/worsened) suggested poor prognosis. 13)
Efforts are underway to incorporate the presence or absence of EZ and ELM disruption into treatment decision-making.
Analysis of CME distribution patterns using en face OCT is identifying image features useful for differentiating causative diseases. 3) In particular, the difference in laminar distribution between acute and chronic phases in CRAO-associated CME is attracting attention as a noninvasive means of etiological estimation.
Lin WC, Hsieh JW, Tsai SH, Lan YW.. Latanoprost-associated cystoid macular edema in a patient with phakic eyes. Taiwan J Ophthalmol. 2023;13(2):242-244. doi:10.4103/tjo.tjo_19_22. PMID:37484608; PMCID:PMC10361437.
Yamane H, Itagaki T, Kajitani K, Koura Y, Kawabuchi Y, Ohara M. Cystoid Macular Edema following Treatment with Nanoparticle Albumin-Bound Paclitaxel and Atezolizumab for Metastatic Breast Cancer. Case reports in oncology. 2023;16(1):1121-1128. doi:10.1159/000533999. PMID:37900858; PMCID:PMC10601834.
Estawro R, Abraham N, Fouad Y, Bousquet E, Sarraf D. Cystoid macular edema as a complication of central retinal artery occlusion. American journal of ophthalmology case reports. 2024;33:101998. doi:10.1016/j.ajoc.2024.101998. PMID:38333032; PMCID:PMC10850887.
Kim MY, Alkhabaz A, Smith SJ, Liao YJ. Siponimod-associated cystoid macular edema without known risk factors. American journal of ophthalmology case reports. 2024;36:102124. doi:10.1016/j.ajoc.2024.102124. PMID:39156909; PMCID:PMC11327528.
Nguyen BT, Hung JH, Thng ZX, El Feky D, Mobasserian A, Saengsirinavin AO, Zhang X, Anover FA, Mohammadi SS, Than NTT, Khatri A, Yavari N, Ganbold B, Yasar C, Elaraby O, Akhavanrezayat A, Yoo WS, Gupta AS, Nguyen QD.. Tocilizumab for Cystoid Macular Edema Secondary to Immune Recovery Uveitis in a Patient with Contraindications to Long-Term Systemic Corticosteroid. Yale J Biol Med. 2024;97(4):423-430. doi:10.59249/nqrt7239. PMID:39703613; PMCID:PMC11650910.
Chaloulis SK, Tsaousis KT.. Cystoid Macular Edema Associated With Venous Stasis in a Patient With Previously Undiagnosed Hyperhomocysteinemia. Cureus. 2021;13(12):e20782. doi:10.7759/cureus.20782. PMID:35111466; PMCID:PMC8794224.
Ben-Avi R, Dori D, Chowers I. Cystoid macular edema secondary to ibrutinib. American journal of ophthalmology case reports. 2022;26:101436. doi:10.1016/j.ajoc.2022.101436. PMID:35243171; PMCID:PMC8881370.
Fukuoka H, Kojima K, Iwama A, Okumura T, Sotozono C. Fingolimod-associated severe bilateral cystoid macular edema. Am J Ophthalmol Case Rep. 2022;26:101553. PMID: 35514796. PMCID: PMC9062136. doi:10.1016/j.ajoc.2022.101553.
Karaca I, Korot E, Ghoraba H, Regenold J, Mobasserian A, Khan Y, et al. Acute iridocyclitis and cystoid macular edema related to kinked Hydrus(®) Microstent in advanced glaucoma. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2022;36(4):390-393. doi:10.4103/sjopt.sjopt_215_21. PMID:36618568; PMCID:PMC9811929.
Szelog JT, Shah NS, Camejo MD. Cystoid Macular Edema Arising 10 Years After Cessation of Pentosan Polysulfate Sodium Successfully Treated With Bevacizumab. Journal of vitreoretinal diseases. 2023;7(1):83-86. doi:10.1177/24741264221136907. PMID:37008392; PMCID:PMC9954163.
Miller KM, Oetting TA, Tweeten JP, et al.; American Academy of Ophthalmology Preferred Practice Pattern Cataract/Anterior Segment Panel. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID:34780842.
OCT biomarkers systematic review. Surv Ophthalmol. 2025. [出典: PIIS0039625725001766.pdf]
Royal College of Ophthalmologists. DRAFT Clinical Guideline on Idiopathic Full-Thickness Macular Holes. 2024.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.