Macular holes are classified by cause into idiopathic and secondary types. Among secondary types, those caused by trauma are called traumatic macular holes. The mechanism involves compression and rebound stretching of the posterior pole retina at the time of trauma, along with traction on the fovea by the attached vitreous, leading to a foveal tear.
Traumatic macular holes account for approximately 5–10% of all macular holes. While idiopathic macular holes are more common in middle-aged and older women, traumatic macular holes are epidemiologically characterized by a higher incidence in young men.
Traumatic macular holes are classified into full-thickness holes and partial-thickness (lamellar) holes based on OCT findings. Full-thickness holes are defects extending from the internal limiting membrane to the retinal pigment epithelium (RPE), while partial-thickness holes involve only a portion of the retinal layers. OCT examination is essential for differentiating between the two.
QWhat is the difference between traumatic macular holes and idiopathic macular holes?
A
Traumatic holes are more common in young males and are often accompanied by traumatic changes such as retinal commotion, hemorrhage, and choroidal rupture around the hole. Additionally, the possibility of spontaneous closure is a major difference from idiopathic holes. In addition to a history of trauma, anterior segment findings such as angle recession can be clues for differentiation.
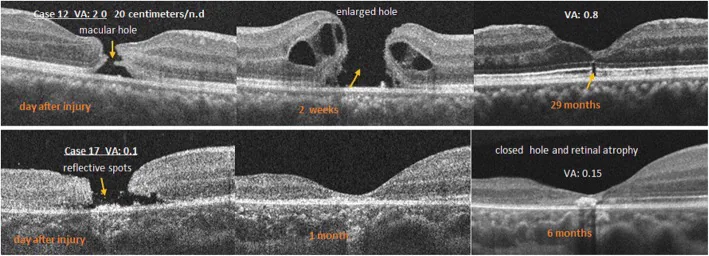
Li D, et al. Optical coherence tomography patterns and outcomes of contusion maculopathy caused by impact of sporting equipment. BMC Ophthalmol. 2018. Figure 4. PMCID: PMC6048845. License: CC BY.
Top left shows a full-thickness macular hole, center shows hole enlargement and surrounding retinal detachment, right shows hole closure and ellipsoid zone defect; middle row shows hole and reflective dots 2 days after injury, closure at 1 month, and atrophic scar at 6 months. Corresponds to traumatic macular holes discussed in section “2. Main Symptoms and Clinical Findings”.
When only a macular hole is present, the main symptoms are decreased visual acuity and distortion (metamorphopsia). When there are associated injuries, symptoms can be diverse.
Decreased visual acuity: Marked reduction in central vision. Varies depending on the extent of associated choroidal rupture and hemorrhage.
Metamorphopsia (distorted vision): Objects appear distorted. Due to morphological changes in the macula.
Central scotoma: Visual field defect in the central area. Reflects functional impairment of the macula.
Commotio retinae: Contusion edema of the retina. Produces a gray-white opacity in the posterior pole.
Vitreous hemorrhage: Bleeding into the vitreous cavity associated with blunt trauma. Obstructs fundus examination.
Retinal contusion necrosis: Necrotic changes in the retinal tissue around the hole. Seen in severe trauma.
Choroidal rupture, vitreous hemorrhage, and subretinal hemorrhage are factors that prevent visual improvement even after hole closure. The presence and extent of these complications greatly influence the final visual prognosis.
The causes of traumatic macular holes are broadly divided into blunt trauma and laser trauma.
Blunt ocular trauma (most common cause):
Sports injuries: A baseball or soccer ball directly hits the eye. Due to the large number of athletes, sports are an important cause.
Assault (fist): Blow with a fist. One reason it is common in young men.
Traffic accidents / occupational injuries: Cases caused by direct impact to the eye.
Laser injury:
When accidentally looking directly at laser light such as a pulsed YAG laser, the macular tissue is thermally and photochemically destroyed, resulting in a macular hole.
Macular damage from laser pointers (especially high-power ones) has also been reported.
Laser-induced macular holes primarily involve direct destruction of photoreceptor cells, and the mechanism of onset differs from that of blunt trauma.
Being a young male (higher incidence of sports and trauma) is the greatest risk factor. Participation in sports without protective eyewear and improper handling of high-power laser devices are triggers.
QCan a macular hole develop just by looking at laser light?
A
When directly viewing a high-energy laser such as a pulsed YAG laser, the macular tissue can be thermally and photochemically destroyed, leading to a macular hole. Damage from laser pointers has also been reported, especially high-power ones (equivalent to Class 3B or Class 4). Laser-induced macular holes primarily involve damage to the photoreceptor cells themselves, unlike blunt trauma.
If there is a clear history of trauma, differentiation from idiopathic macular hole and pseudohole is easy. If the trauma history is unclear or the time of injury cannot be determined, the following findings can aid in differentiation.
OCT is a core examination for diagnosis and follow-up of traumatic macular hole. It objectively enables differentiation between full-thickness and partial-thickness holes, measurement of hole diameter, evaluation of surrounding retinal layer structure, and assessment of vitreoretinal relationship (presence of posterior vitreous detachment). It is also indispensable for determining postoperative hole closure.
Fluorescein angiography is performed to evaluate the extent of choroidal rupture and retinal pigment epithelium (RPE) damage, and to confirm the presence and location of choroidal neovascularization (CNV). Note that traumatic cases often involve RPE and choroidal damage, unlike idiopathic cases.
Since spontaneous closure of traumatic macular holes has been reported in some cases, observation is initially recommended if no complications are present. Follow-up with OCT over several months is performed; if no closure tendency is observed, vitrectomy is considered.
If subretinal hemorrhage occurs, urgent surgery is necessary. The longer subretinal hemorrhage persists, the more toxic it becomes to photoreceptors, worsening visual prognosis 1).
Creation/confirmation of posterior vitreous detachment (PVD): Release adhesions between the vitreous cortex and retina to eliminate traction on the fovea.
Internal limiting membrane (ILM) peeling: Expected to improve closure rates, but efficacy in traumatic holes is unclear. Consider natural closure possibility and OCT findings to determine indication on a case-by-case basis 4).
Fluid-air exchange: Replace intraocular fluid with air.
Long-acting gas tamponade: Replace with long-acting gas such as SF₆ (sulfur hexafluoride) or C₃F₈ (octafluoropropane) to complete surgery.
Postoperatively, maintaining a face-down position allows the gas to tamponade the macula and promote hole closure. Activities are restricted while gas remains, and air travel is prohibited.
QCan a traumatic macular hole heal on its own?
A
Spontaneous closure within a few months has been reported. Therefore, if there is no complication such as subretinal hemorrhage, observation with OCT is often performed first, and vitrectomy is considered if no closure tendency is seen. Spontaneous closure rates vary among reports, and smaller holes are more likely to close spontaneously 1).
QHow much does vision improve after surgery?
A
The macular hole closure rate after vitrectomy is reported to be over 90%. However, visual improvement depends not only on hole closure but also on the extent of choroidal rupture, hemorrhage, and photoreceptor damage. If the associated injuries are severe, improvement may be difficult. Adequate preoperative explanation and sharing of realistic expectations are important 3).
When a blunt external force is applied to the eye, the eyeball undergoes a temporary rapid deformation (shortening of the anteroposterior diameter and expansion of the equatorial diameter). This sudden deformation places the following complex mechanical stresses on the posterior pole retina.
Compression and rebound stretching: Compression of the posterior pole retina due to shortening of the anteroposterior diameter of the eye, followed by strong stretching forces during restoration of the eyeball shape.
Vitreous traction: During ocular deformation, strong traction forces act between the vitreous and the retina near the fovea. In young individuals without posterior vitreous detachment, this traction is particularly strong.
Contrecoup mechanism: The impact energy from the front is transmitted to the posterior pole and concentrates at the fovea.
These mechanisms act in combination, and when tissue tolerance is exceeded, a crack (macular hole) forms at the fovea. One reason traumatic macular holes are more common in young people is that posterior vitreous detachment has not occurred, making vitreous traction more likely.
When high-energy laser light is directed at the macula, thermal and photochemical tissue destruction occurs due to absorption of light energy by the retinal pigment epithelium (RPE), photoreceptors, and retinal pigment. With pulsed YAG lasers, high-density energy is concentrated in a short time, causing explosive destruction of the retinal tissue at the irradiation site, leading to perforation. In laser-induced cases, the photoreceptors themselves are damaged, so the visual prognosis tends to be poorer compared to blunt trauma.
Choroidal rupture results from a tear in Bruch’s membrane, leading to bleeding from the choriocapillaris (subretinal and choroidal hemorrhage) and impaired blood flow to the photoreceptors. Choroidal neovascularization (CNV) may later develop at the site of choroidal rupture. CNV is an important late complication that causes significant vision loss when it occurs in the macula.
Commotio retinae is an opacification and degeneration of the photoreceptor outer segments that occurs early after trauma, reflecting the acute phase of photoreceptor damage. In severe cases, photoreceptors undergo irreversible degeneration, resulting in permanent visual dysfunction.
Research is progressing on the spontaneous closure rate of traumatic macular holes and its predictive factors. Miller et al. (2015) reported a spontaneous closure rate of approximately 30%, and factors such as small hole size in the early post-injury period, presence of posterior vitreous detachment, and OCT morphological findings are being investigated as predictors of spontaneous closure 1).
Yamashita et al. (2002) examined the optimal timing of vitrectomy for traumatic macular holes and suggested that relatively early intervention may be superior in terms of closure rate and visual prognosis 2). However, policies regarding the waiting period considering the possibility of spontaneous closure vary among institutions, and a unified protocol has not been established.
Indications for ILM Peeling and Considerations for Young Patients
Internal limiting membrane (ILM) peeling is standard for idiopathic macular holes, but for traumatic macular holes, spontaneous closure is possible. It is important to determine the timing of surgery and follow-up based on OCT findings, and the indication for peeling should be considered on a case-by-case basis 4).
Anti-VEGF Therapy for Choroidal Neovascularization (CNV)
The therapeutic efficacy of anti-vascular endothelial growth factor (anti-VEGF) drugs for CNV arising at the site of choroidal rupture has been reported. Intravitreal injections of ranibizumab, aflibercept, and bevacizumab are expected to improve visual acuity and suppress exudation, but large-scale RCTs specifically for traumatic CNV are currently lacking 5).
Pharmacologic vitreolysis with ocriplasmin (recombinant microplasmin) was developed for non-invasive release of vitreoretinal traction. It has shown some efficacy for idiopathic small macular holes, but its application to traumatic macular holes is still at the research stage 6).
Miller JB, Yonekawa Y, Eliott D, Vavvas DG. Spontaneous closure of traumatic macular holes: natural history, outcomes, and predictive factors. Retina. 2015;35(8):1587–1594.
Yamashita T, Uemara A, Uchino E, Doi N, Ohba N. Spontaneous closure of traumatic macular hole. Am J Ophthalmol. 2002;133(2):230–235. doi:10.1016/s0002-9394(01)01303-4.
Johnson RN, McDonald HR, Lewis H, Grand MG, Murray TG, Mieler WF, Johnson MW, Boldt HC, Olsen KR, Tornambe PE, Folk JC.. Traumatic macular hole: observations, pathogenesis, and results of vitrectomy surgery. Ophthalmology. 2001;108(5):853-857. doi:10.1016/s0161-6420(00)00650-3. PMID:11320012.
Stalmans P, Benz MS, Gandorfer A, Kampik A, Girach A, Pakola S, Haller JA; MIVI-TRUST Study Group. Enzymatic vitreolysis with ocriplasmin for vitreomacular traction and macular holes. N Engl J Med. 2012;367(7):606-615. doi:10.1056/NEJMoa1110823.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.