Intravitreal injection of anti-VEGF drugs is a treatment that inhibits the effects of VEGF (angiogenesis and increased vascular permeability) by directly injecting the drug solution into the vitreous cavity. The main indications are retinal vascular diseases such as age-related macular degeneration, diabetic macular edema, and retinal vein occlusion.
Retinopathy of prematurity (ROP): Ranibizumab 0.2 mg (approved 2019), aflibercept 0.4 mg (approved September 2022)3)
Geographic atrophy (GA): Complement inhibitors
Endophthalmitis: Direct administration of antibiotics, antifungals, or antivirals
QWhat diseases is anti-VEGF therapy used for?
A
Age-related macular degeneration, diabetic macular edema, and retinal vein occlusion are the three major indications. In all these conditions, VEGF is overproduced, leading to angiogenesis and increased vascular permeability that cause vision loss in the macula. By directly injecting anti-VEGF drugs into the vitreous, these pathological processes are inhibited, aiming to improve or maintain vision. In recent years, indications have expanded to include PDR, mCNV, ROP, polypoidal choroidal vasculopathy, and others.
Mechanism of action: Inhibits all isoforms of VEGF-A
Key trials: Efficacy established for AMD in MARINA/ANCHOR trials. Equivalent to bevacizumab in CATT trial. 12)
Features: PDS allows supplemental dosing every 6 months. 98% no longer need monthly injections after 2 years. For ROP indication, use 40% of adult dose (0.2 mg). 12)
Aflibercept (Eylea®)
Molecular weight: 115 kDa (fusion protein)
Mechanism of action: Simultaneously inhibits VEGF-A, VEGF-B, and PlGF. Highest VEGF-A affinity Kd = 0.49 pM.
Key trials: Non-inferior to ranibizumab in VIEW trials. High-dose 8 mg (HD) allows up to 16-week intervals. 12, 13)
Features: Broad VEGF inhibition spectrum. For ROP indication, use 20% of adult dose (0.4 mg). 13)
Brolucizumab (Beovu®)
Molecular weight: 26 kDa (scFv, smallest among existing drugs)
Mechanism of action: scFv structure allows administration at approximately 12 times the molar concentration of aflibercept. High tissue penetration.
Key trials: Achieved non-inferiority in HAWK/HARRIER trials. Up to 55% maintained 12-week intervals. 10)
Precautions: IOI, retinal vasculitis, and retinal vascular occlusion have been reported in HAWK/HARRIER; monitor for inflammatory findings after injection. 10)
Mechanism of action: Simultaneous inhibition of VEGF-A and Ang-2 (angiopoietin-2). World’s first dual-target drug.
Key trials: TENAYA/LUCERNE (nAMD) up to Q16W. 63% of nAMD patients achieved Q16W in the second year. 8)
Features: In RVO (BALATON/COMINO), FA leakage disappearance rate superior to aflibercept. 8)
Bevacizumab (Avastin®)
Molecular weight: 148 kDa (full-length IgG)
Mechanism of action: VEGF-A inhibition (off-label use in ophthalmology)
Key trials: CATT study confirmed efficacy equivalent to ranibizumab. 12)
Usage: Significantly lower cost. Used by aseptically aliquoting the intravenous infusion formulation.
Pegaptanib (Macugen®)
Mechanism of action: VEGF165-specific aptamer
Current status: First-generation drug approved in 2008. Newer generation drugs are now mainstream. Contributed to establishing the concept of early anti-VEGF therapy.
QWhich drug should be chosen?
A
The choice depends on the indicated disease, desired dosing interval, and risk of complications. Generally, for nAMD, aflibercept, faricimab, and brolucizumab are superior in terms of extended dosing intervals. For DME, aflibercept and faricimab are standard. Brolucizumab has the advantage of high polyp regression rate in PCV patients, considering the risk of IOI. Faricimab allows up to Q16W (every 16 weeks) dosing, minimizing the burden of clinic visits. Ultimately, the attending physician makes a comprehensive decision.
QCan bevacizumab (Avastin) be used?
A
In ophthalmology, it is used off-label, and the intravenous infusion formulation is aseptically prepared for ophthalmic use. The CATT study confirmed visual acuity improvement equivalent to ranibizumab, and due to its significantly lower cost, it is widely used worldwide. However, in Japan, it is not covered by insurance, and its use is at the discretion of the facility.
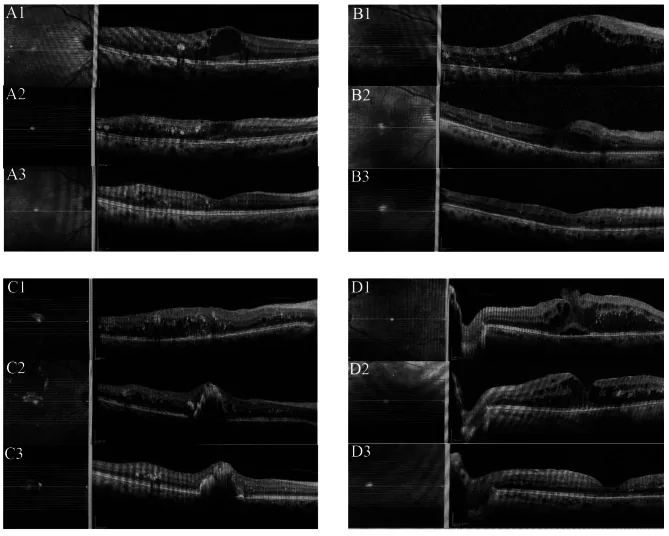
Koc H, Alpay A, Ugurbas SH. Comparison of the efficacy of intravitreal Anti-VEGF versus intravitreal dexamethasone implant in treatment resistant diabetic macular edema. BMC Ophthalmol. 2023 Mar 13;23(1):97. Fig. 1. PMCID: PMC10009964. License: CC BY 4.0.
Macular OCT tomograms of a patient with refractory diabetic macular edema (DME) before intravitreal injection (A1/B1/C1/D1), after three doses of aflibercept (A2/B2/C2/D2), and after six doses (A3/B3/C3/D3). This corresponds to the macular edema resolution effect of anti-VEGF drugs discussed in the section “3. Indications and Dosing Regimens.”
Anti-VEGF drug administration is performed in two phases: induction and maintenance.
Induction phase: To strongly suppress disease activity, fixed monthly doses are given 3 to 6 times (varies by disease and drug).
Maintenance phase has the following three methods:
PRN (pro re nata): Monthly visits, with injection only if recurrence signs are present
Fixed dosing: Regular injections at fixed intervals, e.g., every 2 months or every 3 months
Treat and Extend (T&E): If no activity signs, extend the interval by 2 weeks; shorten if recurrence occurs
For ranibizumab, the basic recommended regimen is 3 monthly induction doses followed by PRN maintenance. For aflibercept, the basic regimen is 3 monthly induction doses followed by fixed dosing every 2 months or T&E. In recent years, T&E has been adopted at many facilities.
Additional doses for recurrence (at least 1 month apart)3)
Management of PCV (Polypoidal Choroidal Vasculopathy): Brolicizumab shows a polyp regression rate of approximately 79%, surpassing other agents, and 76% maintained 12-week intervals at 48 weeks. 14)Faricimab has been reported effective even in ranibizumab-resistant PCV cases. 15)
BALATON trial (BRVO, n=553)8): Faricimab 6.0 mg vs aflibercept 2.0 mg Q4W, 24-week BCVA change was +16.9 letters and +17.5 letters, respectively (non-inferiority achieved, lower bound of 95.03% CI > −4 letters). CST change was −311.4 μm vs −304.4 μm. ≥15-letter improvement: faricimab 56.1% vs aflibercept 60.4%. FA leakage resolution rate was significantly higher with faricimab (33.6% vs 21.0%, nominal p=0.0023).
COMINO trial (CRVO/HRVO, n=729)8): Same regimen, 24-week BCVA change was +16.9 letters and +17.3 letters (non-inferiority achieved). CST change −461.6 μm vs −448.8 μm. ≥15-letter improvement: faricimab 56.6% vs aflibercept 58.1%. FA leakage resolution rate was significantly higher with faricimab (44.4% vs 30.0%, nominal p=0.0002), demonstrating vascular stabilization via Ang-2 inhibition.
IOI safety in RVO (24 weeks)8): In COMINO, IOI occurred in 2.2% with faricimab vs 1.1% with aflibercept. Two cases of severe uveitis (faricimab group). No retinal vasculitis reported in either BALATON or COMINO. APTC events were similar: BALATON 1.1% vs 1.5%, COMINO 1.1% vs 1.4%.
Adjunctive treatment (RVO): In BRVOmacular edema, combination therapy of ranibizumab with subthreshold micropulse laser is being investigated compared to monotherapy. 11)
Anti-VEGF Therapy for Retinopathy of Prematurity (ROP)
Non-inferiority criterion not met, but threshold 66% exceeded
Long-term results of the RAINBOW trial26, 29): High myopia at 5 years was 8% in the ranibizumab 0.2 mg group vs 24% in the laser group (significant difference). Structural abnormality rate was 1.5% in the ranibizumab 0.2 mg group vs 10% in the laser group. Retreatment rate 31%, retreatment timing 4–16 weeks after injection (median 8 weeks).
Follow-up results of the FIREFLEYE trial28): Recurrence rate 21.9%, retreatment rate 17.8%, mean time to retreatment 11 weeks (4–17 weeks). In FIREFLEYE Next (follow-up to 2 years), no treatment-related adverse events on systemic growth or neurodevelopment.
Comparison of recurrence rates between drugs3):
Aflibercept: 13.9–28% (mean recurrence time 11–14.2 weeks)
Ranibizumab: 20.8–83.0% (recurrence time 5.9–9.3 weeks, earlier → careful observation needed from an earlier stage)
Notes on A-ROP3): In A-ROP, anti-VEGF monotherapy requires additional treatment in 75.0–87.5% of cases. Early recurrence occurs within 1–3 weeks after administration; if recurrence occurs within less than 1 month, laser photocoagulation should be combined. When fibrous proliferation is extensive, anti-VEGF monotherapy is contraindicated (risk of tractional retinal detachment due to contraction).
Injection technique for ROP (differences from adults)3):
Insertion site: 1.0–1.5 mm posterior to the limbus (significantly different from 3.5–4 mm in adults; inserting at the adult site risks retinal perforation).
Needle direction: Insert downward (posteriorly) (since the lens is relatively large, aiming centrally risks lens perforation).
Use a 30-gauge or smaller needle.
Confirm dosage: Ranibizumab 0.02 mL, aflibercept 0.01 mL (carefully verify to prevent overdose).
Anesthesia: Choose topical, intravenous, or general anesthesia according to the facility’s situation.
Follow-up3): If retinal vessels have not extended to Zone III, weekly fundus examinations are recommended until 17 weeks after administration. Continue regular fundus examinations for 1 year after administration (tractional retinal detachment has been reported to occur 4–335 days after administration).
QWhich drug is most effective for diabetic macular edema?
A
In the Protocol T study, aflibercept showed the greatest visual improvement at 1 year. However, in the mild group (BCVA ≥20/40), there was no statistically significant difference among the three drugs. 13)Faricimab showed visual improvement equivalent to aflibercept in the YOSEMITE/RHINE trials while allowing longer injection intervals during the maintenance phase (Q16W achieved in 60–64% at year 2). 8) Choose the drug based on patient background and preferences regarding visit frequency.
QWhat is the difference between anti-VEGF therapy and laser treatment for retinopathy of prematurity?
A
Anti-VEGF therapy can be performed in a short time with low invasiveness, and the RAINBOW trial showed superior long-term outcomes in terms of visual field preservation and myopia prevention compared to laser (high myopia at age 5: 8% vs 24%). 26, 29) On the other hand, laser treatment tends to result in more complete retinal vascularization after treatment. Anti-VEGF therapy requires long-term fundus follow-up considering recurrence (ranibizumab 20–83%), and the FIREFLEYE trial reported a recurrence rate of 21.9%. 28) In A-ROP with extensive fibrous proliferation, anti-VEGF monotherapy may be contraindicated. 3)
Anesthesia: Considering the possibility of disinfectant splashing into the fellow eye, administer Benoxil® eye drops to both eyes, then 4% Xylocaine® eye drops to the treated eye twice.
Precautions for PA iodine disinfection:
PA iodine immediately after removal from the refrigerator has reduced antibacterial and antifungal activity, so always return it to room temperature.
When stored in a non-airtight container at 25°C, the residual active ingredient decreases to 60% in 5 hours. Do not use PA iodine that has been left for a long time.
Inactivation of bacteria and fungi requires a contact time of about 1 minute, so after eye washing, keep the eyelids closed to ensure sufficient contact time with the conjunctiva.
Oral bacteria countermeasures: Use a fenestrated drape and have the surgeon, assistants, and all patients wear masks to prevent droplets. Since oral bacteria are among the causative organisms of bacterial endophthalmitis, it is desirable to seal the area between the eye and the drape and mask to prevent exhaled air from spreading to the ocular surface.
The distance from the surgical limbus for injection is as follows. Adhering to the injection site allows insertion at the pars plana (posterior to the pars plicata), preventing lens damage and vitreous hemorrhage.
The needle is inserted toward the center of the vitreous cavity. Insertion too close to the limbus may damage the pars plicata, leading to vitreous hemorrhage, and increases the risk of lens damage due to proximity to the lens.
Apply a fenestrated drape and open the eyelids with a lid speculum.
Measure the distance from the limbus using calipers.
The injection site should be the superotemporal or inferotemporal quadrant (to prevent damage to the horizontal rectus muscles).
Fix the eye with forceps and slightly displace the conjunctiva anteriorly before injection to offset the needle hole after withdrawal and prevent fluid leakage.
Insert a 30G short needle almost perpendicular to the sclera and inject the medication slowly (rapid injection can cause sustained intraocular pressure elevation).
After needle withdrawal, apply pressure to the injection site with a cotton swab.
Immediately after the procedure, check visual acuity (counting fingers). If counting fingers is not perceived, perform anterior chamber paracentesis.
Continue broad-spectrum antibiotic eye drops for 3 days postoperatively.
QDoes the injection hurt?
A
Since the injection is performed after topical anesthesia (Benoxil® or 4% Xylocaine®), the pain during injection is minimal. You may feel irritation from the disinfectant (povidone-iodine), but sodium hyaluronate eye drops are effective for early postoperative discomfort.
Infectious endophthalmitis is the most serious complication, with an incidence of approximately 0.027–0.065%. When it occurs, emergency treatment with intravitreal injection of vancomycin 1.0 mg plus ceftazidime 2.0 mg is required.
Most important preventive measure:
Proper disinfection with povidone-iodine (allow to reach room temperature, contact time of at least 1 minute)
Use of a fenestrated drape (to prevent droplet contamination from oral bacteria)
Regarding postoperative prophylactic antibiotic eye drops, multiple studies have shown that they do not reduce the incidence of endophthalmitis, and the evidence for their efficacy is inconsistent.
This is an intraocular inflammatory reaction without bacterial infection, reported as a rare complication after anti-VEGF drug administration 7). The frequency varies depending on the drug, preparation method, and lot, so differentiation from infectious endophthalmitis is a priority.
Onset timing: Often occurs early after injection, but differentiation from infectious endophthalmitis is necessary 7)
Key findings: May include vitreous opacity, anterior chamber inflammation, and decreased vision 7)
Definitive diagnosis: Negative culture (PCR to rule out pathogens is also useful)
Drug differences: Reported with bevacizumab, ranibizumab, and aflibercept, but the reported frequency varies by study and preparation conditions 7)
Treatment: Conservative treatment is often used for mild cases, but if infectious endophthalmitis cannot be ruled out, prompt decisions including culture collection, intravitreal antibiotic administration, and vitrectomy should be made. 7)
An analysis of 1,044 cases from the IRIS Registry examined outcomes of early vitrectomy for endophthalmitis after intravitreal injection using large-scale data 24).
Intraocular Inflammation (IOI) and Retinal Vasculitis (Brolucizumab-Specific)
Brolucizumab is known to cause IOI more frequently than other anti-VEGF drugs.
Trial / Population
IOI incidence
Notes
HAWK/HARRIER (IOI-related)
Reported
Caution for inflammatory adverse events including retinal vasculitis and vascular occlusion10)
KESTREL (6 mg)
3.7% (control 0.5%)
DME trial10)
MERLIN (4-week interval)
9.3%
Trial discontinued10)
Japanese cases
Reported in case reports and post-marketing data
Caution in frequency estimation
Post-marketing (vasculitis + occlusion complex)
3.73/10,000 injections
The majority of IOI occurs within 6 months after the first dose and within 4 injections. 10)
Mechanism: The involvement of anti-drug antibodies and immune complex-mediated inflammatory mechanisms is being discussed. 10, 25)
Scleritis (first report worldwide): Posterior scleritis after brolucizumab administration has been reported in 3 Japanese patients, accompanied by an increase in intraocular pressure to 24–49 mmHg, and one case progressed to retinal artery occlusion and vasculitis. 9)
Treatment: Subconjunctival or sub-Tenon injection of triamcinolone acetonide (STTA) 5–20 mg is effective. Combination with prophylactic STTA administration has also been reported. 20, 21)
In ROP patients, a complication in which the fibrovascular membrane rapidly contracts after anti-VEGF therapy, leading to tractional retinal detachment (TRD), is called crunch syndrome. 27)
Mechanism: VEGF suppression relatively enhances TGF-β activity. TGF-β promotes fibrosis and extracellular matrix remodeling. Premature infants are physiologically in a period of elevated TGF-β, and anti-VEGF administration amplifies the imbalance. 27)
Prevention: Carefully evaluate fibrotic changes before treatment. Anti-VEGF monotherapy is contraindicated if there is extensive hyperemic fibrovascular proliferation. 3)
Late complication: Tractional retinal detachment has been reported to occur 4 to 335 days after administration, and regular fundus examinations for one year after administration are essential. 3)
After anti-VEGF treatment, complete retinal vascularization may not be achieved, and shunt vessels or abnormal branching patterns may form at the vascular-avascular boundary. 27) Long-term follow-up is necessary (to assess risk of recurrence and late complications). Fluorescein angiography is useful for evaluating normal retinal vascular development.
Transient intraocular pressure elevation immediately after injection occurs in all patients receiving the injection. Injection of 0.05 mL raises intraocular pressure to 50 mmHg instantly, but it is usually reversible. In patients with a history of glaucoma, sustained intraocular pressure elevation requires attention, and anterior chamber paracentesis should be performed for decompression if necessary.
There is a theoretical risk of stroke and myocardial infarction. In the HAWK trial of brolucizumab, ATE occurred in 1.1–1.4%. 10) Caution is required in patients with a history of such events.
QWhat symptoms after injection should prompt a visit to the doctor?
A
If the following symptoms occur, promptly consult an ophthalmologist: (1) sudden vision loss, (2) worsening eye pain or redness, (3) marked increase in floaters, (4) appearance of discharge. These may indicate infectious endophthalmitis or intraocular inflammation (IOI). Particular caution is needed within 24–72 hours after injection.
QWhat should be done if IOI occurs with brolucizumab?
A
If sudden vision loss, worsening floaters, redness, or eye pain occurs, promptly consult an ophthalmologist. After diagnosis, subconjunctival or sub-Tenon injection of triamcinolone acetonide (STTA) is effective, and inflammation improves in most cases. 20, 21) Re-administration should be carefully considered after confirming resolution of inflammation using LFP (laser flare cell photometer) or other methods. In cases with severe vascular occlusion, re-administration may be contraindicated, so switching to an alternative drug should be considered.
6. Pathophysiology (Role of VEGF and mechanism of action of drugs)
VEGF binds to VEGFR-1 and VEGFR-2 on vascular endothelial cells, promoting endothelial cell proliferation, increased vascular permeability, and new blood vessel formation.
DME: Breakdown of the blood-retinal barrier (BRB) leading to macular edema formation
RVO: Ischemia → excess VEGF → macular edema and neovascularization
When VEGF levels are reduced by intravitreal injection, vascular permeability decreases and macular edema improves. The effect of anti-VEGF drugs is temporary, so regular re-administration is necessary.
Pathophysiology of Retinopathy of Prematurity (ROP)
Phase I (Vasocessation phase): In the hyperoxic environment after preterm birth, VEGF and IGF-1 are suppressed. This inhibits normal retinal vascularization, leading to the formation of avascular retina.
Phase II (Pathological neovascularization phase): After oxygen withdrawal, excess VEGF is released from the ischemic retina, which enlarges with growth. Pathological neovascularization occurs at the vascular-avascular junction, progressing from Stage 1–2 demarcation lines and ridges to Stage 3 extraretinal neovascularization. Severe cases progress to Stage 4–5 tractional retinal detachment.
Anti-VEGF drugs inhibit pathological neovascularization by suppressing excess VEGF production in Phase II. However, they also inhibit physiological VEGF-dependent vascularization, so the impact on normal vascular development must be carefully monitored.
Ang-2 acts as an antagonist of the Tie-2 receptor, contributing to vascular destabilization. By inhibiting Ang-2, faricimab normalizes the Tie-2 pathway, improving vascular stability and reducing VEGF sensitivity. This dual inhibition effect is the pharmacological basis for extending the dosing interval.
The reason for administering 3 to 5 fixed monthly doses during the loading phase is to achieve early and strong suppression of disease activity. The treat-and-extend (T&E) method provides a framework that maintains intravitreal drug concentrations within the therapeutic range without allowing recurrence.
7. Latest Research and Future Perspectives (Investigational Reports)
With the ranibizumabPDS (port delivery system), 98% of patients did not require monthly injections with refills every 6 months. 12) In 2025, additional indications for DME are being considered. 13) A significant reduction in injection burden is expected.
In the PULSAR trial (AMD), 79% maintained 12-week intervals and 77% maintained 16-week intervals at 48 weeks. 12) In the PHOTON trial (DME), 93% achieved intervals of 12 weeks or longer. 13)
The PROUD trial (South Korea) targeting PCV and macular telangiectasia type 1 (AT1) is ongoing, and evidence accumulation for Asian-specific diseases is expected. 14, 23)
The SALWEEN trial investigating the effect of faricimab in PCV patients is ongoing. 22) Elevated Ang-2 levels have been confirmed in the aqueous humor of PCV patients, and an additive effect of Ang-2 inhibition is expected.
Combined administration of subconjunctival/sub-Tenon triamcinolone acetonide (STTA) and brolucizumab may be effective for both IOI prevention and exudation control. 20, 21) Research is underway to standardize the optimal dose and timing of administration.
Measurement of cytokine profiles (IL-6, IL-8, IL-10) in vitreous fluid is expected to be a useful adjunct tool for early differentiation between sterile and infectious endophthalmitis. 7)
Biosimilars of ranibizumab and bevacizumab are emerging. Significant cost reductions are expected to improve treatment continuation rates and healthcare access. 12)
Beta-blockers (propranolol): Oral administration prevents progression of Stage 2 ROP. 0.2% eye drops are considered safe and effective (when started in the proliferative phase of Stage 1), but long-term data are insufficient.
Arachidonic acid (AA) and DHA supplements: The Mega Donna Mega Trial reduced severe ROP incidence by 50% (15.8% vs 33.3%).
Caffeine: A treatment for apnea of prematurity, but may suppress ROP progression through downregulation of VEGF and MMPs.
Vitamin A: Meta-analysis showed reduction in ROP incidence and progression.
SAFER-ROP has been proposed as a standardized protocol addressing neonatal-specific challenges (infection prevention in the NICU environment, post-injection monitoring). Based on the acronym Short Needle, Antiseptic/Antibiotic, Follow-Up, Extra Attention to Detail, Recheck, it is used to standardize procedures at each facility.
Lim JI, Kim SJ, Bailey ST, Kovach JL, Vemulakonda GA, Ying GS, Flaxel CJ; American Academy of Ophthalmology Preferred Practice Pattern Retina/Vitreous Committee. Diabetic Retinopathy Preferred Practice Pattern®. Ophthalmology. 2025. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.
日本未熟児網膜症研究会. 未熟児網膜症に対する抗VEGF療法の手引き(第2版). 2024.
Ikuno Y, Ohno-Matsui K, Wong TY, Korobelnik JF, Vitti R, Li T, et al. Intravitreal Aflibercept Injection in Patients with Myopic Choroidal Neovascularization: The MYRROR Study. Ophthalmology. 2015;122(6):1220-7. doi:10.1016/j.ophtha.2015.01.025. PMID:25745875.
Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025 Apr;132(4):P75-P162. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.
American Academy of Ophthalmology. Retinal Vein Occlusion Preferred Practice Pattern. Ophthalmology. 2024. [BRAVO data]
Baudin F, Benzenine E, Mariet AS, Bron AM, Daien V, Korobelnik JF, et al. Association of Acute Endophthalmitis With Intravitreal Injections of Corticosteroids or Anti-Vascular Growth Factor Agents in a Nationwide Study in France. JAMA Ophthalmol. 2018;136(12):1352-1358. doi:10.1001/jamaophthalmol.2018.3939. PMID:30242325. PMCID:PMC6583044.
Tadayoni R, Paris LP, Danzig CJ, Abreu F, Khanani AM, Brittain C, et al. Efficacy and Safety of Faricimab for Macular Edema due to Retinal Vein Occlusion: 24-Week Results from the BALATON and COMINO Trials. Ophthalmology. 2024;131(8):950-960. doi:10.1016/j.ophtha.2024.01.029. PMID:38280653.
Takayama T, Inoda S, Takahashi H, Tsukii R, Yoshida H, Kasuya Y, et al. Scleritis following intravitreal brolucizumab injection: a case series. Journal of medical case reports. 2024;18(1):80. doi:10.1186/s13256-024-04402-9. PMID:38419100; PMCID:PMC10902930.
Sharma A, Kumar N, Parachuri N, Singh S, Bandello F, Regillo CD, Boyer D, Nguyen QD. Understanding retinal vasculitis associated with brolucizumab: complex pathophysiology or Occam’s razor? Ocul Immunol Inflamm. 2022;30(6):1508-1510. doi:10.1080/09273948.2021.1897628.
Nawar AE. Subthreshold micropulse laser combined with ranibizumab versus ranibizumab monotherapy in branch retinal vein occlusion with macular edema. Clin Ophthalmol. 2022;16:1139-1151.
Flaxel CJ, Adelman RA, Bailey ST, et al. Age-related macular degeneration preferred practice pattern. Ophthalmology. 2024;131(1):P1-P68.
Flaxel CJ, Adelman RA, Bailey ST, et al. Diabetic retinopathy preferred practice pattern. Ophthalmology. 2024;131(1):P99-P168.
Parveen Sen, George Manayath, Daraius Shroff, Vineeth Salloju, Priyanka Dhar. Polypoidal Choroidal Vasculopathy: An Update on Diagnosis and Treatment. OPTH. 2023;Volume 17:53-70. doi:10.2147/opth.s385827.
Bloom J, Madani R, Haidar AJ, Alasil T. Faricimab treatment of polypoidal choroidal vasculopathy resistant to intravitreal ranibizumab injections and ranibizumab port delivery (Susvimo). J VitreoRetin Dis. 2024;8(6):731-734. PMID:39554622.
Siddiqui MZ, Durrani A, Smith BT. Faricimab-Associated Retinal Vasculitis. Journal of vitreoretinal diseases. 2024;8(5):627-630. doi:10.1177/24741264241253899. PMID:39318978; PMCID:PMC11418596.
Dhillon N, Macleod S. Intraocular Inflammation Following Intravitreal Faricimab: Insights from Five Bilateral Cases. Journal of vitreoretinal diseases. 2025;9(5):24741264251358623. doi:10.1177/24741264251358623. PMID:40799294; PMCID:PMC12336167.
Christoph R Clemens, Florian Alten, Julian A Zimmermann, Nicole Eter. Old Problem in a New Guise: Retinal Pigment Epithelium Tear after Intravitreal Faricimab (Vabysmo®) Injection. Case Rep Ophthalmol. 2023;241-244. doi:10.1159/000529930.
The combination therapy of subtenon triamcinolone acetonide injection and intravitreal brolucizumab for brolucizumab-related intraocular inflammation. Medicine (Baltimore). 2021;100(42):e27580. doi:10.1097/MD.0000000000027580.
Saito M, et al. A case of intraocular inflammation after intravitreal brolucizumab injection monitored by laser flare-cell photometer. Am J Ophthalmol Case Rep. 2022;28:101727. doi:10.1016/j.ajoc.2022.101727. PMID:36281264; PMCID:PMC9587367.
Cheung CMG, Lai TYY, Teo K, et al. Polypoidal choroidal vasculopathy: consensus nomenclature and non-indocyanine green angiograph diagnostic criteria. Eye. 2024;39:819-834.
Valentina Carta, Filippo Lixi, Filippo Tatti, Enrico Peiretti. Effect of Intravitreal Brolucizumab in the Treatment of Polypoidal Choroidal Vasculopathy With Foveal Lipid Exudation. Cureus. 2023. doi:10.7759/cureus.47942.
Breazzano MP, Bond JB 3rd, Beardsley RM, et al. Intravitreal Antibiotics versus Early Vitrectomy Plus Intravitreal Antibiotics for Postinjection Endophthalmitis: An IRIS (Intelligent Research in Sight Registry) Analysis. Ophthalmol Retina. 2025;9(3):224-231. doi:10.1016/j.oret.2024.09.002.
Teo KYC, et al. Brolucizumab-associated intraocular inflammation: type IV hypersensitivity and cytokine activation. Am J Ophthalmol. 2024.
Stahl A, Lepore D, Fielder A, Fleck B, Reynolds JD, Chiang MF, et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): an open-label randomised controlled trial. Lancet. 2019;394(10208):1551-1559. doi:10.1016/S0140-6736(19)31344-3. PMID:31522845. PMCID:PMC12316478.
Marra KV, Chen JS, Nudleman E, Robbins SL. Review of Retinopathy of Prematurity Management in the Anti-VEGF Era: Evolving Global Paradigms, Persistent Challenges and Our AI-Assisted Future. Clinical & experimental ophthalmology. 2025;53(9):1202-1217. doi:10.1111/ceo.14598. PMID:40908574; PMCID:PMC12747480.
Stahl A, Sukgen EA, Wu WC, et al; FIREFLEYE Study Group. Effect of intravitreal aflibercept vs laser photocoagulation on treatment success of retinopathy of prematurity: the FIREFLEYE randomized clinical trial. JAMA. 2022;328(4):348-359. PMID:35881122. doi:10.1001/jama.2022.10564.
Marlow N, Reynolds JD, Lepore D, Fielder AR, Stahl A, Hao H, et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): five-year outcomes of a randomised trial. EClinicalMedicine. 2024;71:102567. doi:10.1016/j.eclinm.2024.102567. PMID:38638400; PMCID:PMC11024572.
Mintz-Hittner HA, Kennedy KA, Chuang AZ, BEAT-ROP Cooperative Group.. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011;364(7):603-615. doi:10.1056/nejmoa1007374. PMID:21323540; PMCID:PMC3119530.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.