Myopic choroidal neovascularization (myopic CNV) is a choroid-derived new blood vessel that develops in the posterior pole of eyes with pathologic myopia. In recent years, the term “myopic MNV (myopic neovascularization)” has been used internationally to include not only choroid-derived but also retinal vessel-derived new vessels. 6)
High myopia is defined as a spherical equivalent of −6.0 D or less, or an axial length of 26.5 mm or more. Pathologic myopia is defined as eyes with atrophic changes at least as severe as diffuse atrophy in the fundus, or with posterior staphyloma (META-PM classification, 2015). 10)
Myopic MNV is almost always type 2 CNV (CNV located above the RPE) according to the Gass classification. It is often relatively small and exudative changes are usually mild.
Myopic MNV occurs in 5–11% of eyes with high myopia
Over 8 years of follow-up, about 6% of patients with pathologic myopia without a history of MNV develop it
In patients with a history of MNV in one eye, approximately 35% develop it in the fellow eye.
In patients under 50 years of age, about 60% of MNV cases are myopic MNV7).
Pathologic myopia accounts for 13% of visual impairment with corrected visual acuity of 0.1 or less, and is the second leading cause of blindness after glaucoma.
QAt what age does myopic choroidal neovascularization typically develop?
A
Unlike age-related macular degeneration, myopic CNV can develop from a young age (teens). It is the most common cause of choroidal neovascularization in individuals aged 50 years or younger, and is an important disease that impairs central vision in both eyes during the working-age years. Early detection and treatment greatly influence prognosis.
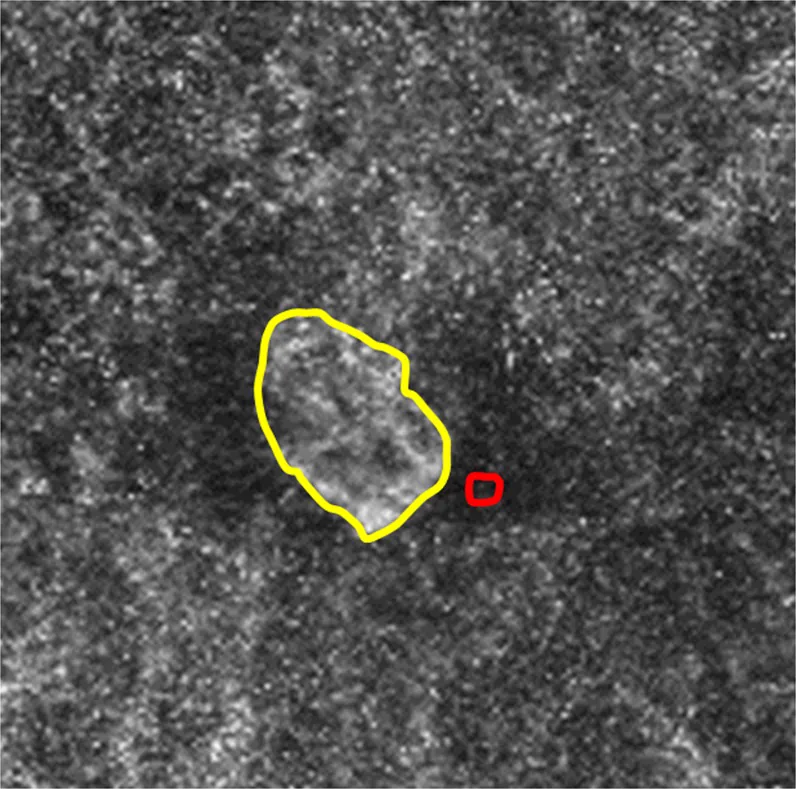
Sawai Y, et al. Usefulness of Denoising Process to Depict Myopic Choroidal Neovascularisation Using a Single Optical Coherence Tomography Angiography Image. Sci Rep. 2020. Figure 3. PMCID: PMC7148361. License: CC BY.
Representative image of the right eye of a 76-year-old woman with myopic choroidal neovascularization, showing the foreground within the yellow line and the background within the red line used to calculate CNR. This corresponds to the choroidal neovascularization discussed in the section “2. Main Symptoms and Clinical Findings.”
When myopic MNV involves the fovea, the following symptoms occur. Because it is type 2 CNV, exudation directly affects the outer retina, causing symptoms to appear early and progress rapidly. 6)
Metamorphopsia: Straight lines appear distorted. New onset of metamorphopsia in a myopic patient is an important sign suggestive of myopic MNV. In cases complicated by myopic traction maculopathy, worsening of distortion may be difficult to notice. 6)
Central scotoma: A dark spot appears in the center of the visual field.
Visual acuity loss: Progresses rapidly when the lesion extends to the fovea. Even if the CNV regresses, if a scar remains at the fovea, irreversible visual loss occurs.
If located outside the macular area, it may be asymptomatic. Careful attention to the patient’s subjective symptoms is important. 6)
OCT findings: Dome-shaped hyperreflective elevation above the RPE. May be accompanied by subretinal fluid, subretinal hemorrhage, cystoid macular edema, or fibrin exudation, but serous changes are not prominent. 6)
Scar and atrophic stages
Fuchs spot: After MNV regression, a scar lesion with pigmentation forms due to hyperplasia of the RPE and basement membrane.
Myopic MNV-related macular atrophy: Expands relatively rapidly over the long term, leading to severe visual impairment. Observed as enlargement of Bruch’s membrane rupture and atrophy of the pigment epithelium, choriocapillaris, and outer retina. Corrected visual acuity ≤0.1 in 88.9% after 5 years and 96.3% after 10 years. 12)
On OCT angiography, the active stage shows a “lace-like network, broad anastomoses, and a low-intensity halo around the lesion,” while the quiescent stage shows “long linear mature vessels and rare anastomoses (dead tree appearance).” Internal blood flow is frequently maintained even outside the active stage (active 100%, scar ~80%, atrophic ~90%). However, OCTA is not suitable for assessing MNV activity. 6)
Long axial length: Risk factor for progression of myopic maculopathy.
Female: Prevalence of myopic chorioretinal atrophy lesions is 3.29 times higher (odds ratio).
QDoes high myopia always lead to choroidal neovascularization?
A
Not all highly myopic eyes develop myopic MNV. The incidence is about 5–11%, and the risk is particularly high in eyes with lacquer cracks or patchy atrophy. 7) Regular eye examinations are important for early detection.
Diagnosis of myopic MNV requires confirmation of fundus changes associated with pathologic myopia and the presence of MNV. 6) Differentiation from simple macular hemorrhage is most important, and anti-VEGF therapy is not recommended for cases where MNV cannot be confirmed. 6)
Diseases that require differentiation from myopic MNV are listed below.
Differential Disease
Key Points for Differentiation
Simple macular hemorrhage
No fluorescein leakage on FA (only fluorescence blockage). OCT shows hyperreflectivity along the Henle fiber layer. Hemorrhage resolves spontaneously within 2–3 months 6), 15)
Common in young myopic women. Multiple small (<500 μm), well-defined yellowish-white lesions at the posterior pole. Choroidal thickening due to inflammation 6)
MNV may develop at the edge of inferior staphyloma6)
QWhat is the difference between simple macular hemorrhage and myopic choroidal neovascularization?
A
Simple macular hemorrhage is caused by damage to the choriocapillaris during lacquer crack formation, resolves spontaneously within 2–3 months, and does not require treatment. On OCT, it appears as hyperreflectivity along the Henle fiber layer. In contrast, myopic MNV is hemorrhage associated with MNV and shows hyperfluorescence (fluorescein leakage) on FA, allowing differentiation. If differentiation is difficult with OCT alone, FA examination is essential. 6)
This is the only treatment whose efficacy has been proven in multicenter prospective randomized controlled trials. 6)
Approved drugs in Japan as of August 2024: ranibizumab (Lucentis®) and its biosimilars, aflibercept (Eylea®). 6)
In a network meta-analysis by Glachs et al. (2024) of 34 studies (2,098 eyes), anti-VEGF agents showed visual acuity improvement of +14.1 letters (95% CI 10.8–17.4) compared to no treatment and +12.1 letters (95% CI 8.3–15.8) compared to PDT within 6 months (both p<0.0001). 1)
Dosing regimen:
Standard: one initial dose followed by PRN (1+PRN) 6), 11)
No significant difference in visual improvement compared to 3+PRN. The 1+PRN group had fewer injections (1.8 vs. 3.2 at 12 months) 1)
Cheung 2017 International Consensus treatment principles:11)
Initiate anti-VEGF therapy promptly for myopic MNV
Consider PDT if anti-VEGF therapy is not possible (similar visual prognosis cannot be expected)
One initial dose followed by PRN
Consider retreatment if OCT shows subretinal fluid, visual decline, or FA shows leakage
Extend interval up to 3 months once MNV is stable 11)
RADIANCE trial: Multicenter RCT of ranibizumab. Demonstrated efficacy. 9)
Comparison between drugs:
No significant difference in visual improvement among bevacizumab, ranibizumab, and aflibercept. 1)Aflibercept shows greater reduction in central retinal thickness, but no difference in visual outcome. 1)
Photodynamic therapy (PDT): Inferior visual improvement compared to anti-VEGF drugs. 1) Possible worsening of macular atrophy in the long term. Not covered by insurance. 6)
Intravitreal triamcinolone acetonide: Inferior to anti-VEGF drugs, with risks of increased intraocular pressure and cataract progression. 1)
Laser photocoagulation: May induce MNV recurrence due to the run-off phenomenon. Currently not recommended.
In young patients and those with small MNV, scar formation is minimal and prognosis is good. Early active intervention as soon as possible after onset is important. 6)
QHow many injections are needed for treatment of myopic choroidal neovascularization?
A
The standard regimen is one injection followed by retreatment as needed (1+PRN), with an average of 1.8 injections over 12 months reported. 1) The number of required injections is generally lower than for age-related macular degeneration. However, long-term follow-up for recurrence and atrophy progression is essential, and early retreatment is recommended. 6)
Choroidal atrophy and decreased elastic fibers in Bruch’s membrane due to axial elongation cause mechanical rupture of Bruch’s membrane, leading to lacquer cracks. Using these rupture sites as a scaffold, connective tissue with MNV proliferates under the retina as a wound healing response. Patchy atrophy and lacquer cracks are predictors of MNV development. 7)
In pathologic myopia, the choriocapillaris and vascular layers are almost absent, and only large choroidal vessels may remain. Studies using EDI-OCT have reported that the choroid is significantly thinner in highly myopic eyes with MNV. Circulatory disturbance in the thinned choroidal tissue promotes VEGF production, leading to the formation of abnormal vascular networks.
Using swept-source OCT and ICGA, findings of short posterior ciliary arteries penetrating the sclera near myopic MNV and adjacent to the MNV were confirmed in 75.0% of cases. Cases where vessels derived from the short posterior ciliary arteries are thought to perfuse the MNV are frequent: 100% in the active stage, 87.9% in the scar stage, and 73.8% in the atrophic stage.
The combination of myopic MNV and myopic foveoschisis (MF) is rare but has important clinical significance.
Sayanagi et al. (2023) reported three cases of MF associated with myopic MNV. 2) In all cases, macular retinal detachment worsened during follow-up. It has been suggested that subretinal fluid from MNV may disrupt the centripetal and centrifugal traction balance, promoting the progression of MF.
Pereira et al. (2023) reported a case in which MNV occurring in a pathologic myopic eye with myopic foveoschisis caused a full-thickness macular hole. 4) It is inferred that mechanical elevation due to MNV exudation applied stress to the Müller cells of the weakened fovea, leading to hole formation.
7. Latest Research and Future Perspectives (Investigational Reports)
Carlà et al. (2025) reported in a long-term study of a European cohort of 1,228 eyes that 57% of myopic maculopathy progressed during follow-up of more than 10 years. 5) 47% of eyes with patchy atrophy progressed to macular atrophy (OR 4.21), and active MNV developed in 15% of eyes at a mean of 4.5 years. MNV development was significantly correlated with visual acuity decline (p=0.001) and progression to macular atrophy (OR 5.81).
Although anti-VEGF therapy provides good short-term visual improvement, long-term outcomes over 5 years are inferior to short-term results. In the natural untreated course, 89% at 5 years and 96% at 10 years have decimal visual acuity of 0.1 or worse. 12) A 5-year study of ranibizumab reported utility in maintaining vision. 13) Developing treatments to suppress the progression of atrophy is a future challenge.
OCT-A Angio-B mode may detect early MNV that is difficult to detect with structural OCT or fluorescein angiography. 3) As a non-invasive and highly sensitive examination method, its application to screening for high myopia is expected.
Glachs L, Embacher S, Berghold A, Wildner B, Michelitsch M, Tscherne A, et al. Treatment of myopic choroidal neovascularization: a network meta-analysis and review. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2024;262(6):1693-1722. doi:10.1007/s00417-023-06271-2. PMID:37950753; PMCID:PMC11106160.
Sayanagi K, Hara C, Fukushima Y, Sato S, Kawasaki R, Nishida K. Three cases of macular retinal detachment exacerbated during follow-up with myopic foveoschisis around myopic choroidal neovascularization. American journal of ophthalmology case reports. 2023;32:101899. doi:10.1016/j.ajoc.2023.101899. PMID:37564973; PMCID:PMC10410127.
Rico S, Sher I, Lavinsky F, Lavinsky D, Rotenstreich Y. Optical coherence tomography Angio-B mode for early detection of myopic choroidal neovascularization and treatment with Bevacizumab. American journal of ophthalmology case reports. 2024;34:102041. doi:10.1016/j.ajoc.2024.102041. PMID:38544916; PMCID:PMC10965462.
Pereira A, Ballios BG, Sarraf D, Yan P. Full-Thickness Macular Hole Due to Choroidal Neovascularization in the Setting of Pathologic Myopia. Journal of vitreoretinal diseases. 2023;7(1):65-69. doi:10.1177/24741264221104592. PMID:37008393; PMCID:PMC9954153.
Carlà MM, Boselli F, Giannuzzi F, et al. Longitudinal Progression of Myopic Maculopathy in a Long-Term Follow-Up of a European Cohort: Imaging Features and Visual Outcomes. Ophthalmol Retina. 2025;9(8):774-786. doi:10.1016/j.oret.2025.02.015. PMID:40010496.
Ohno-Matsui K, Yoshida T, Futagami S, Yasuzumi K, Shimada N, Kojima A, Tokoro T, Mochizuki M.. Patchy atrophy and lacquer cracks predispose to the development of choroidal neovascularisation in pathological myopia. Br J Ophthalmol. 2003;87(5):570-573. doi:10.1136/bjo.87.5.570. PMID:12714395; PMCID:PMC1771643.
Ikuno Y, Ohno-Matsui K, Wong TY, Korobelnik JF, Vitti R, Li T, et al. Intravitreal Aflibercept Injection in Patients with Myopic Choroidal Neovascularization: The MYRROR Study. Ophthalmology. 2015;122(6):1220-7. doi:10.1016/j.ophtha.2015.01.025. PMID:25745875.
Wolf S, Balciuniene VJ, Laganovska G, Menchini U, Ohno-Matsui K, Sharma T, et al. RADIANCE: a randomized controlled study of ranibizumab in patients with choroidal neovascularization secondary to pathologic myopia. Ophthalmology. 2014;121(3):682-92.e2. doi:10.1016/j.ophtha.2013.10.023. PMID:24326106.
Ohno-Matsui K, Kawasaki R, Jonas JB, Cheung CM, Saw SM, Verhoeven VJ, Klaver CC, Moriyama M, Shinohara K, Kawasaki Y, Yamazaki M, Meuer S, Ishibashi T, Yasuda M, Yamashita H, Sugano A, Wang JJ, Mitchell P, Wong TY, META-analysis for Pathologic Myopia (META-PM) Study Group.. International photographic classification and grading system for myopic maculopathy. Am J Ophthalmol. 2015;159(5):877-83.e7. doi:10.1016/j.ajo.2015.01.022. PMID:25634530.
Cheung CMG, Arnold JJ, Holz FG, Park KH, Lai TYY, Larsen M, Mitchell P, Ohno-Matsui K, Chen SJ, Wolf S, Wong TY. Myopic Choroidal Neovascularization: Review, Guidance, and Consensus Statement on Management. Ophthalmology. 2017;124(11):1690-1711. doi:10.1016/j.ophtha.2017.04.028. PMID:28655539.
Yoshida T, Ohno-Matsui K, Yasuzumi K, Kojima A, Shimada N, Futagami S, Tokoro T, Mochizuki M.. Myopic choroidal neovascularization: a 10-year follow-up. Ophthalmology. 2003;110(7):1297-1305. doi:10.1016/s0161-6420(03)00461-5. PMID:12867382.
Onishi Y, Yokoi T, Kasahara K, Yoshida T, Nagaoka N, Shinohara K, Kaneko Y, Suga M, Uramoto K, Ohno-Tanaka A, Ohno-Matsui K.. FIVE-YEAR OUTCOMES OF INTRAVITREAL RANIBIZUMAB FOR CHOROIDAL NEOVASCULARIZATION IN PATIENTS WITH PATHOLOGIC MYOPIA. Retina. 2019;39(7):1289-1298. doi:10.1097/iae.0000000000002164. PMID:29746414.
Miyata M, Ooto S, Hata M, Yamashiro K, Tamura H, Akagi-Kurashige Y, Nakanishi H, Ueda-Arakawa N, Takahashi A, Kuroda Y, Wakazono T, Yoshikawa M, Yoshimura N.. Detection of Myopic Choroidal Neovascularization Using Optical Coherence Tomography Angiography. Am J Ophthalmol. 2016;165:108-114. doi:10.1016/j.ajo.2016.03.009. PMID:26973049.
So Goto, Kaori Sayanagi, Yasushi Ikuno, Yukari Jo, Fumi Gomi, Kohji Nishida. COMPARISON OF VISUAL PROGNOSES BETWEEN NATURAL COURSE OF SIMPLE HEMORRHAGE AND CHOROIDAL NEOVASCULARIZATION TREATED WITH INTRAVITREAL BEVACIZUMAB IN HIGHLY MYOPIC EYES. Retina. 2015;35(3):429-434. doi:10.1097/iae.0000000000000332.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.