
Laser Trabeculotomy for Glaucoma (ELT/FLIGHT)
1. What is Laser Trabeculotomy?
Section titled “1. What is Laser Trabeculotomy?”Laser trabeculotomy is a surgery that uses a laser to penetrate the trabecular meshwork and create a passage (channel) into Schlemm’s canal. It is classified as a trabecular laser procedure in MIGS (minimally invasive glaucoma surgery)1).
While selective laser trabeculoplasty (SLT) induces a biological effect on trabecular meshwork cells to enhance aqueous outflow, laser trabeculotomy fundamentally differs by physically creating channels.
Currently, there are two methods:
- Excimer laser trabeculotomy (ELT): An intraocular (ab interno) procedure using a 308 nm xenon chloride excimer laser
- Femtosecond laser image-guided high-precision trabeculotomy (FLIGHT): A non-incisional method that delivers femtosecond laser through the cornea
Minimally invasive glaucoma surgery has a moderate intraocular pressure-lowering effect compared to traditional filtration surgery but offers a superior safety profile1)2). Although trabeculectomy remains the most effective pressure-lowering surgery, the indications for MIGS are expanding for early to moderate open-angle glaucoma and ocular hypertension to reduce medication burden1).
SLT (selective laser trabeculoplasty) is a procedure that irradiates pigmented cells of the trabecular meshwork to induce cytokine release, biologically enhancing aqueous outflow. In contrast, ELT (excimer laser trabeculotomy) physically penetrates the trabecular meshwork to create channels into Schlemm’s canal. SLT is an outpatient procedure, while ELT requires an incision into the eye and is usually performed in combination with cataract surgery.
2. Excimer Laser Trabeculotomy (ELT)
Section titled “2. Excimer Laser Trabeculotomy (ELT)”Principle
Section titled “Principle”ELT uses a 308 nm xenon chloride (XeCl) excimer laser to create microperforations between the anterior chamber and Schlemm’s canal. Because it is a non-thermal ablation with short pulses (20 Hz, 60–120 nanoseconds), damage to surrounding tissue and collector channels is minimized, and scar formation and inflammatory response are also reduced.
Procedure
Section titled “Procedure”A corneal paracentesis is created, and a disposable fiberoptic probe with an angled metal tip is inserted into the anterior chamber. Under gonioscopic guidance, the tip is placed in contact with the trabecular meshwork, and approximately 10 microperforations (about 0.2 mm in diameter) are created over a 90-degree range. After laser application, bubbles and a small amount of reflux bleeding are observed, indicating penetration of the inner wall of Schlemm’s canal. After the procedure, viscoelastic material is removed, and the wound is closed with corneal stromal hydration.
Efficacy
Section titled “Efficacy”The safety and efficacy of ELT have been reported in multiple studies.
| Study | Subjects | Follow-up | IOP change |
|---|---|---|---|
| Stodtmeister (2011) | 166 eyes, ELT alone | 1 year | 26.4 → 16.9 mmHg |
| Stodtmeister (2013) | 46 eyes, ELT alone | 5 years | 25.5 → 15.9 mmHg |
| Töteberg-Harms (2017) | 113 eyes, PEA combined comparison | 4 years | 19→14 mmHg |
It is often performed in combination with cataract surgery. In a study by Moreno Valladares et al. (34 eyes, mean follow-up 11.5 months), mean intraocular pressure decreased from 20.9 mmHg to 16.3 mmHg, and 81% of eyes were medication-free. In an 8-year follow-up by Riesen et al. (161 eyes), IOP significantly decreased from 19.3 mmHg to 15.4 mmHg, but no significant reduction in the number of medications was observed.
Complications
Section titled “Complications”Reported complications of ELT are rare and mainly consist of clinically insignificant transient microhyphema. The frequency of serious complications is markedly lower compared to trabeculectomy.
3. Femtosecond Laser Image-Guided High-Precision Trabeculotomy (FLIGHT)
Section titled “3. Femtosecond Laser Image-Guided High-Precision Trabeculotomy (FLIGHT)”Principle
Section titled “Principle”FLIGHT (ViaLase® Laser Technology) is a non-incisional method that delivers femtosecond laser pulses through the cornea to the iridocorneal angle, performing precise photodisruption of the trabecular meshwork. The fundamental difference from ELT is that it creates a passage connecting the anterior chamber and Schlemm’s canal without incising the eyeball.
Procedure
Section titled “Procedure”A portable gonioscopic camera is used to visualize the iridocorneal angle and select the treatment site. A coupling lens is fixed to the target eye with a suction ring and docked to the laser system. Using real-time gonioscopic video and OCT, the laser is aimed at the trabecular meshwork surface with micron-level precision, and treatment is activated with a foot switch.
Efficacy and Safety
Section titled “Efficacy and Safety”In a prospective pilot study by Nagy et al. (11 patients, 18 eyes, 2-year follow-up), mean intraocular pressure decreased from 22.3 mmHg to 14.5 mmHg (p=0.00005). Approximately 82% of eyes achieved an IOP reduction of 20% or more from baseline. No serious adverse events such as vision loss, corneal edema, hypotony, hyphema, peripheral anterior synechiae, or IOP spikes were reported. At 24 months, clear channels were confirmed by gonioscopy and anterior segment OCT.
FLIGHT is a non-incisional method that irradiates the laser through the cornea, requiring no incision in the eyeball. In this respect, it differs from ELT and conventional trabeculotomy, making it a less invasive procedure. However, at present, it is still in the preliminary research stage, and large-scale long-term data are not yet available.
4. Comparison with Conventional Trabeculotomy
Section titled “4. Comparison with Conventional Trabeculotomy”External Trabeculotomy
Section titled “External Trabeculotomy”Conventional trabeculotomy is a procedure in which a scleral flap is created, Schlemm’s canal is identified, and a metal probe (trabeculotome) is inserted into Schlemm’s canal and rotated to incise the trabecular meshwork. Complications include hyphema (almost inevitable), Descemet’s membrane detachment, cyclodialysis, and transient ocular hypertension. Postoperative intraocular pressure often ranges from 16 to 20 mmHg 3).
Microhook Internal Trabeculotomy (MIGS)
Section titled “Microhook Internal Trabeculotomy (MIGS)”This is one of the MIGS procedures that has rapidly gained popularity in recent years. It preserves the conjunctiva and sclera, and directly incises the trabecular meshwork under gonioscopy through a small corneal incision. It has short-term efficacy comparable to conventional external trabeculotomy, with less induced astigmatism and faster visual recovery. Simultaneous performance with cataract surgery is standard 3).
5. Latest Research and Future Prospects
Section titled “5. Latest Research and Future Prospects”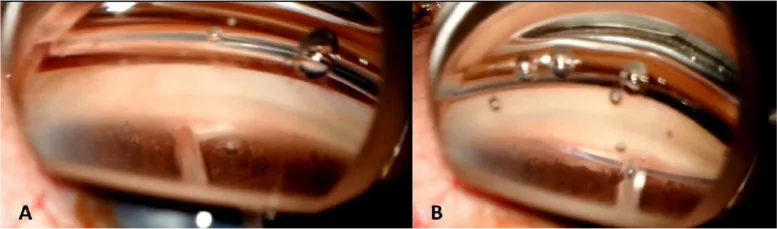
Long-term Outcomes of ELT
Section titled “Long-term Outcomes of ELT”An 8-year follow-up study by Riesen et al. demonstrated the long-term intraocular pressure-lowering effect of ELT combined with cataract surgery. However, the long-term reduction in the number of medications was limited, and some cases required additional treatment. Reoperation was reported to be rare.
Potential of FLIGHT
Section titled “Potential of FLIGHT”FLIGHT is the only laser trabeculotomy that does not require an incision in the eyeball. Pilot studies have shown safety and efficacy, but the number of patients was small and follow-up periods were limited. In the future, large-scale efficacy and safety data from randomized controlled trials are essential.
Reporting Standards for Minimally Invasive Glaucoma Surgery
Section titled “Reporting Standards for Minimally Invasive Glaucoma Surgery”In clinical trials of minimally invasive glaucoma surgery, there is a trade-off between safety and efficacy, and endpoint settings different from those of conventional filtration surgery are required 2). Establishing standardized reporting standards is a future challenge.
Laser trabeculotomy as a minimally invasive glaucoma surgery is mainly indicated for patients with early to moderate open-angle glaucoma or ocular hypertension. It is particularly useful when performed concurrently with cataract surgery to reduce medication burden. For patients with advanced glaucoma or those requiring low target intraocular pressure, conventional filtration surgery is recommended.
6. References
Section titled “6. References”
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
日本緑内障学会緑内障診療ガイドライン改訂委員会. 緑内障診療ガイドライン(第5版). 日眼会誌. 2022;126(2):85-177.