Developmental glaucoma is a general term for glaucoma caused by developmental abnormalities of the aqueous humor outflow pathway, and is classified into early-onset and late-onset types based on the timing of onset. Early-onset developmental glaucoma corresponds to what was previously called “primary congenital glaucoma,” and the cause of elevated intraocular pressure is limited to developmental abnormalities of the trabecular meshwork. Late-onset developmental glaucoma has a milder degree of angle developmental abnormality, leading to later onset; it is difficult to detect abnormalities by gonioscopy, and corneal enlargement or Haab striae are often absent.
Primary congenital glaucoma (PCG) is a rare disease in which intraocular pressure rises due to genetically determined abnormalities of the trabecular meshwork and anterior chamber angle, without other ocular or systemic developmental abnormalities. Previously, terms such as trabeculodysgenesis, goniodysgenesis, and primary infantile glaucoma were used, but the 2013 international classification by the Childhood Glaucoma Research Network (CGRN) unified the term to primary congenital glaucoma 1).
Primary congenital glaucoma is the most common form of primary childhood glaucoma and is classified into the following four types based on the timing of onset 1).
Neonatal onset (0-1 month): the most severe type.
Infantile onset (over 1 month to 24 months): the most frequent type, typically occurring between 3 and 9 months of age.
Late-onset (delayed recognition type) (over 2 years): The later the onset, the fewer the symptoms and signs.
Spontaneously arrested type: Extremely rare. Intraocular pressure is normal, but typical findings of primary congenital glaucoma such as buphthalmos and Haab striae are present.
The incidence in white Europeans is 1 in 12,000 to 18,000 births 1). In some regions of Eastern Europe, it is as high as 1 in 1,250. With consanguineous marriage, the incidence increases 5 to 10 times 1). 65–80% of cases are bilateral, and the male-to-female ratio is about 3:2, with a male predominance 1).
Primary congenital glaucoma accounts for less than 0.01% of all eye disease patients, but is estimated to account for 5% of childhood blindness worldwide. 75% are bilateral, 65% occur in boys, and 80% develop within the first year of life.
In a large ANZRAG cohort (290 cases of childhood glaucoma), PCG was the most common at 57.6% (167/290 cases), and infantile-onset PCG was the most common at 53.3% (89/167 cases). The male-to-female ratio for PCG was 1.46:1, and the median age at diagnosis was 0.25 years (IQR 0–0.6 years) 7).
Classification of Secondary Childhood Glaucoma (WGA)
Congenital glaucoma includes not only primary congenital glaucoma but also secondary types. The four categories of secondary childhood glaucoma according to the World Glaucoma Association (WGA) are shown below.
Category
Main Diseases
Glaucoma associated with congenital ocular anomalies
Young age at surgery and microphthalmia are risk factors
QHow often does primary congenital glaucoma occur?
A
In Caucasians, it is reported in 1 in 12,000 to 18,000 births, but in regions with high consanguinity, it rises to 1 in 1,250. 65–80% of cases are bilateral1).
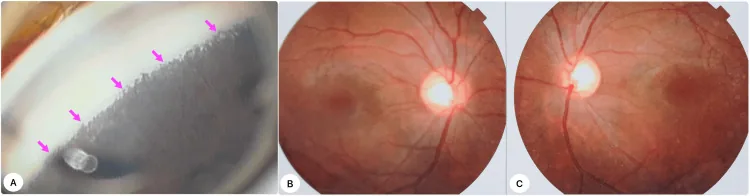
Iqbal MI, et al. A Landmark Case of Childhood Glaucoma Care in Bangladesh: Gonioscopy-Assisted Transluminal Trabeculotomy in Primary Congenital Glaucoma. Cureus. 2025. Figure 1. PMCID: PMC11934033. License: CC BY.
Left: Gonioscopy photograph showing anterior iris insertion indicating angle dysgenesis. Center and right: Fundus photographs of both eyes showing enlarged optic disc cupping. These correspond to the clinical findings of primary congenital glaucoma discussed in the section “Main Symptoms and Clinical Findings.”
Patients with primary congenital glaucoma present with one or more of the following “clinical triad” as irritative symptoms due to corneal edema from elevated intraocular pressure1).
Visual loss due to corneal edema/opacity, progressive myopia, and astigmatism may also occur. In infants, caregivers often notice “white eye,” “large eye,” or “bluish eye” and seek medical attention.
Clinical Findings (Findings Confirmed by Physician Examination)
Haab striae: Horizontal to oblique breaks in Descemet’s membrane, a strong indicator of congenital glaucoma1).
Increased corneal diameter: Normal at birth is 9.5–10.5 mm. Over 12 mm before age 1, or over 13 mm at any age, strongly suggests glaucoma.
Corneal edema and opacity: Epithelial (sometimes stromal) edema. If untreated, it can lead to permanent scarring.
Ocular and Optic Nerve Findings
Buphthalmos: Enlargement of the entire eyeball due to elevated intraocular pressure. Corneal enlargement may progress until about age 3, and scleral stretching until about age 10.
Optic disc cupping: In infants, a cup-to-disc ratio of 0.3 or more suggests glaucoma. Cupping may improve (reverse) after normalization of intraocular pressure.
Increased axial length: Over 20 mm at birth, or over 22 mm after age 1, is abnormal 1).
About Haab striae: When the corneal diameter increases rapidly, Descemet’s membrane cannot stretch enough and tears. These tears are called Haab striae, which cause corneal astigmatism and can hinder visual development.
As a reference for normal corneal diameter, it is approximately 9.5–10.5 mm in newborns and increases to 10.0–11.5 mm by about 1 year of age. If it exceeds 12.0 mm shortly after birth, this condition is strongly suspected.
Diagnostic criteria (based on the Glaucoma Practice Guidelines)
According to the Glaucoma Practice Guidelines, the diagnosis is based on the presence of at least one of the following four findings:
Intraocular pressure of 22 mmHg or higher measured on two or more occasions
Large cup-to-disc ratio (0.3 or more, or asymmetry of 0.2 or more)
Visual field defects suggestive of glaucoma
Increased corneal diameter or axial length
According to the EGS 6th edition, a diagnosis of primary congenital glaucoma is made when at least 2 of the following 5 items are met1).
Intraocular pressure: >21 mmHg
Corneal findings: Haab striae, corneal edema, increased corneal diameter (neonates ≥11 mm, 1 year ≥12 mm, any age >13 mm)
Optic disc cupping: Progressive rim thinning, cup-to-disc ratio difference ≥0.2 between eyes
Progressive myopia: Axial length increase disproportionate to age
Angle findings: High iris insertion, persistent uveal tissue, trabecular dysgenesis
QCan a child with just large eyes have glaucoma?
A
A corneal diameter exceeding 13 mm at any age is highly suspicious for glaucoma. In spontaneously arrested primary congenital glaucoma, buphthalmos and Haab striae may be present despite normal intraocular pressure, requiring follow-up as suspected glaucoma.
Most cases of primary congenital glaucoma are sporadic (no family history), but about 10–40% are familial with autosomal recessive inheritance and penetrance of 40–100%1). Linkage analysis has identified five genetic loci.
The main causative genes are as follows:
Gene
Locus
Chromosome
Function
CYP1B1
GLC3A
2p22-p21
Fatty acid/vitamin metabolism enzyme
LTBP2
GLC3D
14q24.2-q24.3
Latent TGF-beta binding protein
TEK/TIE2
GLC3E
9p21
Schlemm’s canal development signal
CYP1B1 (GLC3A): The most common causative gene. It is expressed in the neuroepithelium and ciliary body of the fetus and adult, and metabolizes compounds essential for eye development. CYP1B1-deficient mice show severe trabecular meshwork atrophy. CYP1B1 mutations tend to cause relatively early onset, bilateral, and typical progression.
LTBP2 (GLC3D): Expressed in the trabecular meshwork and ciliary processes, but its role in the eye is not fully understood.
TEK/TIE2 (GLC3E): The angiopoietin/TEK signaling pathway is essential for the development of Schlemm’s canal, and TEK knockout mice lack Schlemm’s canal.
MYOC: May be involved in up to 5.5% of primary congenital glaucoma cases.
EFEMP1 has also been reported as a candidate gene 1).
According to the ANZRAG cohort report on genetic diagnostic yield, molecular diagnosis was achieved in 24.7% (125/506) of all cases. In PCG, molecular diagnosis was possible in 30.4% (41/135), including CYP1B1 biallelic mutations in 15.6% (21 cases), TEK heterozygous mutations in 5.9% (8 cases), CPAMD8 in 3.7% (5 cases), and FOXC1 heterozygous mutations in 3.7% (5 cases). Reclassification of PCG subtype based on genetic diagnosis occurred in 10.4% (FOXC1 mutations reclassified as ARS, CPAMD8 mutations as ASD) 7). CYP1B1 biallelic mutations tended to be more common in females with PCG (66.7% vs 33.3%, P=0.02) 7).
The probability of identifying a cause through genetic testing is approximately 24–40%. Genetic testing is recommended for exclusion of other congenital anomalies and for family planning 1).
Consanguineous marriage is considered a factor for disease severity and poor prognosis 1). The probability that a second child of a patient with primary congenital glaucoma will be affected is usually less than 3%, but if two children are already affected, it rises to 25% assuming autosomal recessive inheritance.
QShould I undergo genetic testing?
A
The EGS guidelines recommend genetic testing for exclusion of other congenital anomalies and for family planning 1). The ANZRAG cohort showed a genetic diagnostic rate of 30.4% for PCG, and genetic diagnosis led to reclassification of the disease subtype in 10.4% of cases 7). A negative test does not rule out primary congenital glaucoma, but it may contribute to diagnostic accuracy and appropriate management.
The diagnosis of primary congenital glaucoma can often be made clinically even if intraocular pressure measurements are not accurate. The presence of Haab striae is a strong indicator of congenital glaucoma1).
Intraocular pressure measurement: It is best to measure with a handheld tonometer (including a rebound tonometer) at rest while awake1). Note that crying can cause falsely high values, and general anesthetics can cause falsely low values. Rebound tonometers can also be used for home measurement1). All drugs used under general anesthesia lower intraocular pressure. The only exception is the dissociative anesthetic ketamine hydrochloride, which may slightly increase intraocular pressure. If intraocular pressure is 20 mmHg under sevoflurane anesthesia, it will exceed 30 mmHg when awake. Some consider 15 mmHg or 12 mmHg as the upper normal limit under sevoflurane anesthesia.
Corneal diameter and thickness measurement: Corneal diameter should be monitored over time; if it exceeds the age-appropriate normal range, poor intraocular pressure control is suspected. Central corneal thickness may be increased even without edema and can affect intraocular pressure measurements1).
Axial length measurement: Essential for diagnosis and follow-up. Progression of myopia and increase in axial length suggest glaucoma progression.
Gonioscopy: Essential for type diagnosis and treatment selection, but often requires general anesthesia in infants. If corneal opacity makes gonioscopy difficult, ultrasound biomicroscopy (UBM) is useful.
Optic disc evaluation: Baseline fundus photographs should be recorded. Improvement in cupping is often seen after intraocular pressure reduction. In particular, about 50% of cases under 1 year of age who achieve good intraocular pressure control with surgical treatment show a decrease in cup-to-disc ratio of 0.2 or more, indicating that optic disc cupping in children is reversible, unlike in adults.
Visual acuity and refraction testing: Irregular astigmatism, corneal opacity, and Haab’s striae can cause amblyopia, so refraction testing should be performed regularly alongside intraocular pressure measurement during follow-up.
Surgery is the first-line treatment 2). This is because primary congenital glaucoma is caused by developmental abnormalities of the angle that can be surgically corrected, it is difficult to confirm the effectiveness of drug therapy in infants, and there are issues with caregiver-dependent adherence 2). Drug therapy is used as a perioperative or postoperative adjunct 2).
Surgery should be performed at a facility with sufficient experience in pediatric ophthalmology and glaucoma treatment, and comprehensive management including reoperation, long-term follow-up, and amblyopia treatment is necessary 2).
Trabeculotomy: Has the advantage of being feasible even when corneal transparency is poor 2). Creation of conjunctival and scleral flaps is required, which may make future filtration surgery difficult. 360-degree trabeculotomy using a microcatheter has also been attempted 2). The success rate is 78% for cases with onset within 2 months of birth, which is somewhat low, but 96% for cases with onset after that.
Goniotomy: Indicated for cases with clear corneas 2). A single surgery can incise 90-120 degrees, and up to three approaches from different sites are possible 2). The success rate is particularly good at 94% for onset between 1 month and 2 years of age. However, it is low at 26% for onset before 1 month and 38% for onset after 2 years.
For primary congenital glaucoma with onset between 3 and 12 months of age, both goniotomy and trabeculotomy have similar success rates (70-90%) 2). The choice of procedure depends on the surgeon’s experience. Risk factors for failure are the degree of angle underdevelopment and excessive enlargement of the anterior segment 2).
Trabeculectomy: Indicated for cases where angle surgery is ineffective 2). The sclera in primary congenital glaucoma patients is thin, making flap creation difficult, and bleb formation may be challenging even with antimetabolites. The 1-year success rate is 50-87%, which is poorer than in adults 2).
Glaucoma drainage device (GDD) surgery: Used in cases where filtration surgery is ineffective. A meta-analysis of 32 studies involving 1,221 eyes with Ahmed valve and Baerveldt implant showed that the mean preoperative IOP of 31.8 ± 3.4 mmHg decreased to a mean postoperative IOP of 16.5 mmHg (95% CI 15.5–17.6) at 12 months 8). The success rate decreased over time: 87% at 12 months (95% CI 0.83–0.91), 77% at 24 months (95% CI 0.71–0.83), and 37% at 120 months. There was no significant difference in success rates between the Ahmed and Baerveldt groups 8). Major complications included shallow anterior chamber (13.6%), hypotony (11.7%), and choroidal effusion (8.3%).
Cyclodestructive procedures: Considered when intraocular pressure cannot be controlled with all the above treatments 2).
Medication therapy is an adjunctive treatment aimed at short-term intraocular pressure reduction before surgery and postoperative intraocular pressure control 2). Medications are used in combination according to primary open-angle glaucoma, but the following precautions are necessary.
In infants, the dose tends to be excessive relative to body weight and body surface area, so start with the lowest possible concentration of medication.
Oral acetazolamide (carbonic anhydrase inhibitor): Administer 5–10 mg/kg every 6–8 hours. It is useful for emergency intraocular pressure reduction before surgery 2).
Beta-blockers (e.g., timolol): Parents must be informed about side effects such as bronchial asthma and bradycardia. In neonates, there have been reports of apnea, so caution is needed.
Alpha-2 adrenergic receptor agonists (e.g., brimonidine) are absolutely contraindicated in children under 2 years of age. They can cause neuropsychiatric symptoms (somnolence, bradycardia, hypotension, etc.) 1)2).
Prostanoid FP receptor agonists have weaker effects in children compared to adults 2). In children, the uveoscleral outflow pathway is underdeveloped, so there are many non-responders, but they are considered to have slightly better intraocular pressure-lowering effects than beta-blockers.
Eye drops enter the systemic circulation directly from the lacrimal sac and nasal mucosa, so even one drop can easily cause serious systemic side effects in children. Instruction on nasolacrimal occlusion after instillation is recommended.
Lifelong intraocular pressure monitoring is essential, and optimal visual development support through refractive correction and amblyopia treatment is also indispensable 1).
QWhy is surgery the first choice instead of medication therapy?
A
Primary congenital glaucoma is caused by abnormal development of the angle, which can be surgically corrected. In infants, it is difficult to confirm the effectiveness of medications, and there are also adherence issues. Furthermore, the drugs available for children are limited, such as contraindications to α₂ receptor agonists and reduced efficacy of prostanoids 2).
Elevated intraocular pressure in primary congenital glaucoma results from impaired aqueous humor outflow due to abnormal development of the anterior chamber angle 1).
In the 1950s and 1960s, the cause was explained by a non-perforating membrane (Barkan membrane) covering the angle, but subsequent histological studies have denied the existence of such a membrane. Currently, outflow obstruction is thought to originate from the trabecular meshwork itself.
Normally, during the third trimester of pregnancy, the ciliary body and peripheral iris move posteriorly away from the cornea and sclera. In primary congenital glaucoma, it is proposed that excessive or premature accumulation of collagen beams within the trabecular meshwork prevents this posterior migration, leaving the iris root and ciliary muscle attached anteriorly, obstructing the trabecular meshwork or compressing Schlemm’s canal.
Rao (2025) performed histological analysis of trabecular meshwork specimens from four patients with primary congenital glaucoma and reported enlargement of the juxtacanalicular meshwork (JCM) and corneoscleral meshwork, thickening of TM beams, an increase in spindle-shaped nuclei (suggesting epithelial-mesenchymal transition), and the presence of two morphologically distinct zones within the JCM 3). These findings suggest abnormal differentiation and heterogeneity of differentiation in various TM regions in primary congenital glaucoma.
7. Latest Research and Future Perspectives (Research Stage Reports)
GATT (gonioscopy-assisted transluminal trabeculotomy) is a relatively new procedure in which a microcatheter or suture is inserted into Schlemm’s canal under gonioscopy through a corneal incision to incise the entire circumference of the trabecular meshwork. Its efficacy is being established in adult glaucoma, and its application in children is advancing.
Song et al. (2022) reported a case of GATT performed on a 3-year-old boy with primary congenital glaucoma. The iris covered the entire angle up to Schwalbe’s line, making normal angle structures invisible, but the iris was detached using a hook to identify Schlemm’s canal, and GATT was successfully performed. Intraocular pressure was stable at 6 months postoperatively 4).
Elhusseiny et al. (2023) reported one-year outcomes of GATT in 7 eyes of 6 patients with primary congenital glaucoma who had previous glaucoma surgery. Mean intraocular pressure significantly decreased from 25.7±5.9 mmHg preoperatively to 12.0±1.5 mmHg at 12 months. The complete success rate was 85.7% (6/7 eyes), and including qualified success it was 100%; no eyes required additional glaucoma surgery. No serious complications were observed5).
Dada et al. (2022) reported a new technique for primary congenital glaucoma with corneal opacity, performing goniotomy while visualizing the angle structure using a 23G laser endoscope probe6). Traditionally, goniotomy required a clear cornea, but with endoscopic assistance, it may become feasible even in eyes with corneal opacity.
For high-risk groups such as those with a family history or in regions with high consanguinity, prenatal genetic screening may emerge as a preventive measure in the future. In the ANZRAG cohort, genetic diagnosis reclassified the PCG subtype in 10.4% of cases, suggesting that genetic diagnosis contributes to more accurate diagnosis and appropriate management7). Accumulation of evidence from future large international cohorts is expected.
A systematic review of QOL in pediatric glaucoma patients found that 10 types of patient-reported outcome measures (PROMs) have been used, but no questionnaire specific to pediatric glaucoma currently exists9). IVI_C, CVAQC, and LVP-FVQ-II received relatively high ratings (5/7 points) as vision-specific pediatric instruments. Pediatric glaucoma patients have concerns about the future (employment, family planning, fear of surgery) that are not adequately covered by existing PROMs9). Development of pediatric glaucoma-specific PROMs is a future challenge.
In successful surgical cases, long-term visual prognosis is relatively good. With either goniotomy or trabeculotomy, approximately 60% of successful cases maintain corrected visual acuity of 0.5 or better.
Perform refraction testing and refractive correction as early as possible, and conduct frequent refraction tests to keep up with changes in prescription.
Lifelong intraocular pressure monitoring is essential.
Health-Related QoL (HRQoL) in pediatric glaucoma patients is comparable to that of children with congenital heart disease or acute lymphoblastic leukemia (PedsQL 4.0 score approximately 76–79/100). Better QoL is associated with good visual acuity, primary type, and unilateral involvement; number of surgeries, number of eye drops, and bilateral involvement are associated with lower QoL9).
QWhat is the long-term visual prognosis after surgery?
A
In successful surgical cases, approximately 60% maintain a corrected visual acuity of 0.5 or better. However, lifelong intraocular pressure management, refractive correction, and amblyopia treatment are essential. Addressing corneal astigmatism due to Haab’s striae and progressive myopia is key to maintaining visual function. In cases requiring GDD surgery, the success rate decreases over time: 87% at 12 months and 77% at 24 months, making long-term follow-up mandatory 8).
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Rao A. Histopathological changes in the trabecular meshwork in primary congenital glaucoma. American journal of ophthalmology case reports. 2025;38:102340. doi:10.1016/j.ajoc.2025.102340. PMID:40475128; PMCID:PMC12138567.
Song Y, Zhang X, Weinreb RN.. Gonioscopy-assisted transluminal trabeculotomy in primary congenital glaucoma. Am J Ophthalmol Case Rep. 2022;25:101366. doi:10.1016/j.ajoc.2022.101366. PMID:35146211; PMCID:PMC8818529.
Elhusseiny AM, Aboulhassan RM, El Sayed YM, Gawdat GI, Elhilali HM. Gonioscopy-Assisted Transluminal Trabeculotomy following Failed Glaucoma Surgery in Primary Congenital Glaucoma: One-Year Results. Case reports in ophthalmological medicine. 2023;2023:6761408. doi:10.1155/2023/6761408. PMID:37304219; PMCID:PMC10250098.
Dada T, Satpute K, Bukke AN, Verma S. Endoscope-assisted goniotomy in primary congenital glaucoma with corneal opacification. BMJ case reports. 2022;15(11). doi:10.1136/bcr-2022-252958. PMID:36357114; PMCID:PMC9660561.
Knight LSW, Ruddle JB, Taranath DA, et al. Childhood and early onset glaucoma classification and genetic profile in a large Australasian disease registry. Ophthalmology. 2024;131(1):62-73.
Stallworth JY, O’Brien KS, Han Y, Oatts JT. Efficacy of Ahmed and Baerveldt glaucoma drainage device implantation in the pediatric population: a systematic review and meta-analysis. J AAPOS. 2023;27(3):139.e1-139.e10.
Stingl JV, Ortolano LC, Azuara-Blanco A, Hoffmann EM. Systematic Review of Instruments for the Assessment of Patient-Reported Outcomes and Quality of Life in Patients with Childhood Glaucoma. Ophthalmology. Glaucoma. 2024;7(4):391-400. doi:10.1016/j.ogla.2024.02.009. PMID:38423388.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.