Lacrimal passage obstruction (stenosis or occlusion) causing tearing as the main symptom is called lacrimal duct obstruction. Among these, obstruction at or beyond the entrance of the nasolacrimal duct is termed nasolacrimal duct obstruction (NLDO).
Slit-lamp examination may reveal a high tear meniscus, and delayed clearance of fluorescein staining suggests lacrimal duct obstruction. Diagnosis is confirmed by irrigation test.
Drug-induced: Glaucoma eye drops such as timolol, dorzolamide, and pilocarpine; IDU (antiviral drug); S-1 (TS-1®).
Canalicular obstruction
Definition: A condition in which the canaliculi (upper and/or lower) are obstructed.
Yabe-Suzuki classification: Grade 1 (common canaliculus obstruction with communication), Grade 2 (no communication between upper and lower, insertion possible 7–8 mm or more), Grade 3 (obstruction more proximal than Grade 2).
Features: Anticancer drug-related cases often involve bilateral and simultaneous upper and lower involvement.
Common canaliculus obstruction
Definition: A condition in which the junction of the upper and lower canaliculi (common canaliculus) is obstructed.
Treatment strategy: Recanalization by DEP or SEP is the basic approach but is technically challenging; if not possible, CDCR (conjunctivodacryocystorhinostomy) is considered.
Nasolacrimal duct obstruction
Definition: A condition in which the nasolacrimal duct from the lacrimal sac to the opening in the inferior meatus is obstructed.
Most common site: Obstruction at the entrance of the nasolacrimal duct is the most frequent.
Since lacrimal endoscopy was covered by insurance in 2018 1), it has become possible to observe the degree of fibrosis and mucosal inflammation at the obstruction site, improving the accuracy of differentiating between common canaliculus and nasolacrimal duct obstruction. The concordance rate between obstruction site estimation by irrigation test and lacrimal endoscopy findings is about 70% 1), highlighting the significance of direct endoscopic observation.
Tearing includes not only lacrimal drainage obstruction but also hypersecretion of tears (e.g., reflex tearing due to dry eye). If reflux is observed during lacrimal irrigation, obstruction can be diagnosed. Evaluate tear secretion by BUT measurement or Schirmer test for differentiation.
Punctal and canalicular obstruction occurring during anticancer treatment with S-1 (tegafur/gimeracil/oteracil potassium combination, TS-1®) often becomes severe. Early tube insertion is recommended. Among anticancer drug-related lacrimal obstructions, punctal and canalicular disorders account for about 60% 1). If the tube is removed during anticancer drug use, reobstruction is likely, so it is desirable to continue tube placement during treatment 1).
Nasolacrimal duct obstruction is the most common cause of adult epiphora. It is more frequent in women and the elderly, and anatomical narrowing of the nasolacrimal duct is considered a contributing factor. Cone-beam CT dacryocystography analysis has shown that the angle between the superior orbital rim, the internal common punctum, and the nasolacrimal duct opening is anteriorly flexed in 92% of cases 3), and this morphological characteristic is thought to contribute to the risk of obstruction.
Lacrimal sac stones: Complicated in 7.5% of nasolacrimal duct obstruction cases, posing a risk for acute dacryocystitis4).
Intracanalicular tumors: Pathological examination during DCR reveals granulation tissue/reactive lymphoid hyperplasia in 5.9% and tumors in 1.4% (of which 69% are malignant)5).
Chronic dacryocystitis: Stagnation of tears and secretions proximal to the obstruction leads to bacterial overgrowth, resulting in chronic dacryocystitis.
Causes of nasolacrimal duct obstruction include chronic inflammation, age-related changes, as well as Stevens-Johnson syndrome, ocular cicatricial pemphigoid, and drug-induced factors (glaucoma eye drops, antiviral drugs, anticancer agents).
Giombi F, Muci G, Cerasuolo M, et al. Enhancing Endoscopic Dacryocystorhinostomy: A Novel Transethmoidal Approach to the Lacrimal Fossa. Cureus. 2025;17:e92327. Figure 1. PMID: 41103842; PMCID: PMC12522051. DOI: 10.7759/cureus.92327. License: CC BY 4.0.
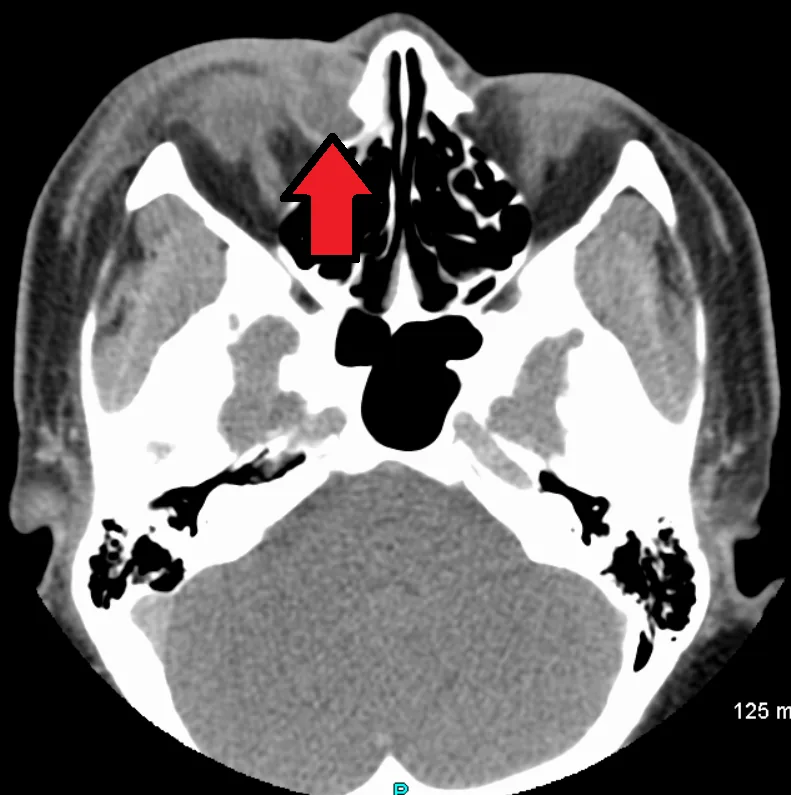
Iodinated contrast CT shows a left lacrimal sac mucocele associated with lower nasolacrimal duct obstruction in coronal and axial views. This corresponds to the evaluation of lacrimal sac dilation and nasolacrimal duct obstruction site by CT discussed in the “Diagnosis and Examination Methods” section.
Direct visualization of obstruction, fibrosis, mucosal inflammation
Moderate
Since 2018
Orbital and sinus CT
Lacrimal sac fossa, nasal cavity shape, sinusitis, mass
Moderate
Yes (preoperative)
Lacrimal endoscopy was covered by insurance in 2018 1) and is useful for diagnosing the degree of fibrosis at the obstruction site, mucosal inflammation, and intralacrimal masses. CT or MRI is used when extralacrimal lesions are suspected.
Dacryocystography can be ambiguous in determining whether contrast reaches the obstruction site 1), and it mainly serves as a complement to direct observation with lacrimal endoscopy.
Lacrimal hypersecretion (reflex due to dry eye): Differentiated by BUT and Schirmer test
Reflex epiphora due to conjunctivitis/keratitis: Differentiated by slit-lamp findings
Canaliculitis: Often associated with canalicular stones
Dacryocystitis (secondary infection): Swelling, tenderness, and fever over the lacrimal sac area
Intralacrimal tumors: Reports of malignant melanoma, papilloma, and granuloma
QIs lacrimal duct obstruction the only cause of watery eyes (epiphora)?
A
The causes of epiphora are broadly divided into “lacrimal passage obstruction (normal tear production but impaired drainage)” and “lacrimal hypersecretion (increased tearing due to irritation).” Lacrimal duct obstruction is the most common cause, but reflex epiphora due to dry eye, conjunctivitis, and keratitis can also cause tearing. Differentiation is made by evaluating tear secretion with BUT measurement and Schirmer test, and checking for passage obstruction with lacrimal irrigation.
QIs lacrimal endoscopy covered by insurance?
A
It was covered by insurance in 2018. Dacryoendoscopy allows direct visualization of the obstruction site and is useful for diagnosing the degree of fibrosis, mucosal inflammation, and intralacrimal tumors. It is particularly helpful for detailed classification of obstruction sites that are difficult to estimate with irrigation tests (e.g., differentiating common canalicular obstruction from nasolacrimal duct obstruction, and distinguishing between lacrimal sac-nasolacrimal duct junction obstruction and lower membranous nasolacrimal duct obstruction).
The following are performed as acute phase/initial management.
Observation with steroid eye drops, antibiotic eye drops, and lacrimal sac massage
When acute dacryocystitis is present: incision and drainage plus intravenous/oral antibiotics, followed by surgical planning after inflammation subsides
Under topical anesthesia, the punctum is incised and dilated using a punctal dilator or sharp blade. A punctal plug is placed for 2–4 weeks and then removed; if reocclusion occurs, a silicone tube is placed in the canaliculus for 1–2 months and then removed.
Gradual punctal dilation (from small to large) followed by lacrimal tube placement can prevent reocclusion. The indwelling period is 1–7 months, and the success rate 3–12 months after tube removal is reported to be 81.8–100%1).
After intralacrimal anesthesia with 4% lidocaine hydrochloride solution, the canaliculus is sufficiently dilated with a punctal dilator. A bicanalicular or catheter-type silicone tube is carefully inserted from the punctum while feeling the resistance at the obstruction site, left in place for 1–2 months, and then removed.
Endoscopic Treatment for Yabe-Suzuki Classification Grade 1
The obstruction is perforated using DEP (direct endoscopic probing) or SEP (sheath-guided endoscopic probing)1).
DEP: The dacryoendoscope probe itself is used as a bougie.
SEP: A Teflon lacrimal sheath is attached as an outer tube, and the tip of the sheath is used to perforate the obstruction. Perforation can be performed while observing the lumen.
The tube is left in place for 2 to 10 months. The patency rate by Kaplan-Meier method at 878 days postoperatively is reported to be 94% 1).
The difficulty level is significantly higher. If perforation is difficult with DEP/SEP, a thin metal bougie may be used to attempt perforation 1). If both the upper and lower canaliculi cannot be opened, CDCR (conjunctivodacryocystorhinostomy) is considered.
Jones tube: 87% of patients experience benefit, but lifelong placement is required (use is restricted as it is not approved domestically).
Conjunctival pedicle flap CDCR: Success rate 75%. Abduction impairment has been reported.
Conjunctivodacryocystostomy (lacrimal sac transposition): All cases showed improvement in epiphora at 1 year postoperatively 1).
The obstruction is perforated using DEP or SEP, and a tube is inserted via SGI (sheath-guided intubation) or G-SGI 1).
SGI: The sheath is placed in the lacrimal passage, the tube is connected inside the sheath, and then the sheath is pulled out from the nasal cavity to guide the tube into the nasal cavity.
G-SGI: A modified SGI that does not require intranasal manipulation.
Direct tube insertion has a reported 22% rate of submucosal misinsertion 1), so the SGI/G-SGI method is recommended. The tube is left in place for 2 to 12 months. The surgical success rate at 1 year after tube removal is 70–87% 1). The success rate of DSI (direct silicone intubation) is low at approximately 52.5% (8–30 months after tube removal) 1), and the patency rate at 3,000 days after tube removal is 64%, with long-term recurrence risk reported 1). Risk factors for recurrence include a history of dacryocystitis, long disease duration, long obstruction length, and male sex 1).
This is indicated for patients with long-standing symptoms of epiphora and discharge who desire surgery. In acute dacryocystitis, surgical planning is made after incision and drainage and anti-inflammatory treatment. For patients who do not wish for radical surgery, bougie or tube placement can delay surgery, but it should be fully explained in advance that the outcomes of tube placement for nasolacrimal duct obstruction are not favorable.
Anesthesia: Mix Bosmin® and 2% Xylocaine® in a 1:1 ratio, soak in gauze, and insert into the nasal mucosa at the osteotomy site using ENT forceps.
Skin incision: Make an incision with a round knife along the anterior lacrimal crest from the upper edge of the medial canthal tendon to the entrance of the nasolacrimal duct.
Osteotomy: Create a bone window approximately 1×1 cm in the lacrimal sac fossa. Use a flat chisel, round chisel, and mallet, or an electric drill.
Stent placement: Place a silicone tube and silicone pod in the bone window. Concurrent use of Beskitchin® is useful for maintaining the bone window space and hemostasis.
Postoperative management: Remove Beskitchin® at 1 week, the silicone pod at 1 month, and the silicone tube at 2 months after surgery.
The success rate of external DCR is 90–99% 1), and many reports indicate a reocclusion rate of less than 10%. Some reports suggest that the endoscopic (intranasal) DCR has slightly inferior outcomes due to the smaller bone window.
The main complications associated with dacryoendoscopic surgery and lacrimal tube intubation are listed below1).
Mucosal laceration / submucosal tube misinsertion: The most common intraoperative complication. Can be avoided with SGI/G-SGI technique.
Cheese-wiring (slit-like laceration of the punctum): Risk increases with excessive punctal incision/dilation or long-term intubation (≥9 months).
Intracanalicular granulation: Caused by tube contact/friction. Treated with corticosteroid eye drops, usually resolves within 1 month after tube removal.
Dacryocystitis/infectious keratitis: Bacterial overgrowth (Moraxella lacunata, S. mitis, Pseudomonas aeruginosa, alpha-hemolytic streptococci, etc.) due to long-term tube placement.
Orbital cellulitis: Spread of lacrimal sac bacteria into the orbit due to submucosal misinsertion of the tube. Requires intravenous antibiotics and immediate tube removal.
QWhat surgical options are available for nasolacrimal duct obstruction?
A
There are two main types: “endoscopic dacryoplasty with tube intubation” and “DCR (dacryocystorhinostomy).” Tube intubation is less invasive, with a 1-year success rate of 70–87% after removal, but carries a long-term recurrence risk. External DCR is curative with a high success rate of 90–99% and a reocclusion rate below 10%. The choice depends on symptom severity, disease duration, and patient preference.
QI have persistent tearing due to side effects of the anticancer drug S-1. Can it be treated?
A
S-1 (TS-1®)-induced lacrimal duct obstruction often involves the punctum and canaliculi and tends to be severe, so early silicone tube intubation is recommended. Removing the tube during anticancer therapy often leads to reocclusion, so it is advisable to maintain tube placement while treatment continues. If you notice symptoms, consult an ophthalmologist promptly.
QWhen will the tube be removed after surgery?
A
It depends on the site of obstruction and the surgical technique. Typical durations are: punctal tube placement 1–7 months, canalicular endoscopic treatment (DEP/SEP) 2–10 months, and nasolacrimal duct tube intubation 2–12 months. Optimal timing for tube removal based on endoscopic findings is expected to be established in the future.
Obstruction at the entrance of the nasolacrimal duct is most common. Chronic inflammation, age-related changes, and anatomical narrowing are involved in a complex manner.
When obstruction occurs, tears and secretions accumulate proximal to the blockage (lacrimal sac side). The accumulated mucus serves as a culture medium for bacteria, leading to overgrowth of Moraxella lacunata, S. mitis, Pseudomonas aeruginosa, alpha-hemolytic streptococci, etc., and progression to chronic dacryocystitis1). Reduced tear clearance also contributes to chronic corneal and conjunctival changes.
A report analyzing lacrimal duct morphology using cone-beam CT dacryocystography found that the angle between the superior orbital rim, internal common punctum, and nasolacrimal duct opening was anteriorly flexed in 92% of cases 3), and this morphological characteristic is thought to affect the difficulty of instrument insertion into the nasolacrimal duct and the formation of obstructions.
Lacrimal duct endoscopes come in two types: a specification with an outer diameter of 0.9 mm and 10,000 observation pixels (2012 improved model), and an operability-priority type with an outer diameter of 0.7 mm and 3,000 pixels 1). In 2020, the depth of focus was improved to accommodate observation distances of 1.5 to 7 mm. A bent type with a 27° upward bend at the distal 10 mm is mainly used, and straight and double-bent types are selected according to the case 1).
Lacrimal sac stones form due to chronic inflammation and secretion retention 4). Intralacrimal duct tumors are sometimes discovered by lacrimal duct endoscopy, with reports of malignant melanoma, papilloma, and granuloma 1). Since malignant tumors are found in approximately 1.0% (69% of all tumors) of pathological examinations during DCR, histopathological examination of surgical specimens is recommended 5).
Lacrimal duct endoscopy was developed by Suzuki et al. in 2002 2) and was covered by insurance in 2018 1). SGI and G-SGI are also discussed in the guidelines as methods to avoid submucosal misinsertion, and standardization of lacrimal duct endoscopic tube insertion is progressing 1).
Lacrimal duct endoscopic probing for congenital nasolacrimal duct obstruction has a high cure rate of 92.3–100% 1) and is considered one of the treatment options.
Determination of the optimal timing for lacrimal tube removal based on lacrimal duct endoscopic findings (degree of fibrosis at the obstruction site, mucosal inflammation) is expected in the future 1).
Conjunctivodacryocystostomy (lacrimal sac transposition) is attracting attention as a new surgical technique for Grade 2 and 3 canalicular obstructions, with improvement in epiphora reported in all cases at one year postoperatively 1).
Diagnosis and treatment of nasolacrimal duct obstruction using lacrimal duct endoscopy is a field where Japan leads the world, and standardization is progressing based on the guidelines for lacrimal duct endoscopic practice 1).
Nakamura J, Kamao T, Mitani A, Mizuki N, Shiraishi A. Analysis of Lacrimal Duct Morphology from Cone-Beam Computed Tomography Dacryocystography in a Japanese Population. Clin Ophthalmol. 2022;16:2057-2067. doi:10.2147/OPTH.S370800. PMID:35770249. PMCID:PMC9235895.
Koturović Z, Knežević M, Rašić DM. Clinical significance of routine lacrimal sac biopsy during dacryocystorhinostomy: A comprehensive review of literature. Bosn J Basic Med Sci. 2017;17(1):1-8. doi:10.17305/bjbms.2016.1424. PMID:27754826. PMCID:PMC5341772.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.