Lacrimal intubation (lacrimal tube insertion) is a surgical procedure in which a silicone tube is placed to reopen and maintain the patency of the lacrimal pathway for obstruction or stenosis of the punctum, canaliculus, common canaliculus, or nasolacrimal duct. The technique varies greatly depending on the site of obstruction, and there are appropriate surgical approaches for each.
In daily ophthalmic practice, many patients complaining of epiphora have lacrimal duct stenosis or obstruction. If slit-lamp examination reveals a high tear meniscus and delayed clearance of fluorescein staining, lacrimal obstruction is likely, and a lacrimal irrigation test confirms the diagnosis.
The main purpose of lacrimal tube intubation is to place a silicone tube in the obstructed lacrimal passage for a certain period to achieve canal patency and promote natural mucosal regeneration. It is not a radical procedure, and outcomes vary depending on the site and severity of obstruction.
For nasolacrimal duct obstruction, DCR (dacryocystorhinostomy) is a radical treatment with a success rate of 90–99% 3), but tube intubation is a less invasive option that may be positioned as a bridge treatment before radical surgery. It is necessary to explain to the patient preoperatively that the results of tube placement for nasolacrimal duct obstruction are not favorable.
Introduction of lacrimal endoscopy and advances in technique
With the development of lacrimal endoscopy (fiber scope with outer diameter 0.7–0.9 mm, 6,000–10,000 pixels), it has become possible to directly observe the obstructed site and perform perforation and tube insertion 1). Perforation methods such as DEP (direct endoscopic probing) and SEP (sheath-guided endoscopic probing), and tube insertion methods such as SGI (sheath-guided intubation) and G-SGI have become widespread, reducing the risk of submucosal misinsertion 1).
QIn what cases is lacrimal tube intubation performed?
A
It is performed when epiphora and discharge persist due to obstruction or stenosis of the punctum, canaliculus, or nasolacrimal duct. A silicone tube is placed in the obstructed area to reopen and maintain the lacrimal passage. For nasolacrimal duct obstruction, DCR (dacryocystorhinostomy) has a success rate of 90–99%, but tube intubation is a less invasive option. The procedure is selected based on the site of obstruction, patient condition, and preference.
2. Classification and symptoms of lacrimal obstruction
Punctal obstruction is mainly caused by scarring from chronic inflammation such as burns, chemical corrosion, Stevens-Johnson syndrome (SJS), and ocular pemphigoid. Drug-induced causes such as glaucoma eye drops (timolol, dorzolamide, etc.) and TS-1 (tegafur, gimeracil, oteracil potassium) are also important.
Canalicular and common canalicular obstruction result from inflammatory scarring and postoperative adhesions. Severity is assessed using the Yabe-Suzuki classification (grades 1-3), and treatment difficulty varies greatly.
Nasolacrimal duct obstruction is an obstruction from the lacrimal sac to the opening of the inferior nasal meatus, with obstruction at the entrance of the nasolacrimal duct being the most common. It is known as an acquired lacrimal disease that is more common in elderly individuals and women.
Yabe-Suzuki Classification of Canalicular Obstruction
The Yabe-Suzuki classification is used to assess the severity of canalicular obstruction1). The difficulty of treatment varies greatly depending on the degree and location of the obstruction, making accurate preoperative classification important.
Grade
Definition
Treatment Difficulty
Grade 1
Bougie can be inserted ≥11 mm, communication between upper and lower puncta present (common canalicular obstruction)
Standard
Grade 2
No communication between upper and lower puncta, bougie can be inserted ≥7–8 mm
Lacrimal duct obstruction occurring during anticancer treatment with TS-1 (tegafur/gimeracil/oteracil potassium combination) or 5-FU (fluorouracil) tends to become severe. Punctal and canalicular involvement accounts for approximately 60% of cases1), and early tube intubation is recommended. Since removal of the tube during anticancer therapy often leads to re-obstruction, it is desirable to maintain tube placement during continued treatment1). Anticancer drug-related lacrimal duct obstruction is often bilateral and involves both upper and lower canaliculi simultaneously, making it particularly refractory2).
Acquired nasolacrimal duct obstruction is a major cause of adult epiphora and occurs predominantly in women and the elderly. Age-related fibrosis and inflammatory changes of the lacrimal drainage system are considered the main underlying factors.
Congenital nasolacrimal duct obstruction is commonly observed in neonates and infants, but more than 90% resolve spontaneously by 1 year of age, so observation is the basic approach. For cases persisting beyond 1 year or those with recurrent dacryocystitis, probing or endoscopic lacrimal surgery may be considered1).
Drug-induced lacrimal duct obstruction due to anticancer agents such as TS-1 and 5-FU occurs with a certain frequency, and once obstruction progresses, it tends to become refractory2). It is recommended to observe epiphora symptoms from the early stage of administration and to promptly perform tube intubation once obstruction is confirmed1).
Lacrimal irrigation test (syringing) is the most basic diagnostic method; in nasolacrimal duct obstruction, reflux of mucus from the punctum is observed. It is minimally invasive and can be performed in an outpatient setting.
Dacryocystography shows contrast medium interruption at or beyond the nasolacrimal duct entrance and dilatation of the lacrimal sac. It is useful for estimating the level of obstruction, but the concordance rate with endoscopic findings is about 70% 1).
Lacrimal endoscopy is a method that directly visualizes the lacrimal passage lumen using a fiberscope with an outer diameter of 0.7–0.9 mm, and was covered by insurance in 2018 1). It is useful for accurate identification of the obstruction site (differentiating common canalicular obstruction from nasolacrimal duct obstruction), assessment of fibrosis degree and mucosal inflammation, and detection of intralacrimal masses. The concordance rate between obstruction site estimation by irrigation and lacrimal endoscopic findings is about 70%, highlighting the importance of direct endoscopic observation 1).
Preoperative CT (orbital and sinus) is performed in surgical candidates to evaluate the shape of the lacrimal sac fossa and nasal cavity, and the presence of sinusitis.
QWhat is lacrimal endoscopy?
A
It is a device that directly visualizes the lacrimal passage lumen using an ultra-thin fiberscope with an outer diameter of 0.7–0.9 mm. It allows accurate identification of the obstruction site and endoscopic perforation and tube insertion. The concordance rate with irrigation test is about 70%, and lacrimal endoscopy provides a more accurate diagnosis. It was covered by insurance in 2018 and is particularly useful for evaluating the degree of fibrosis, mucosal inflammation, and intralacrimal masses at the obstruction site.
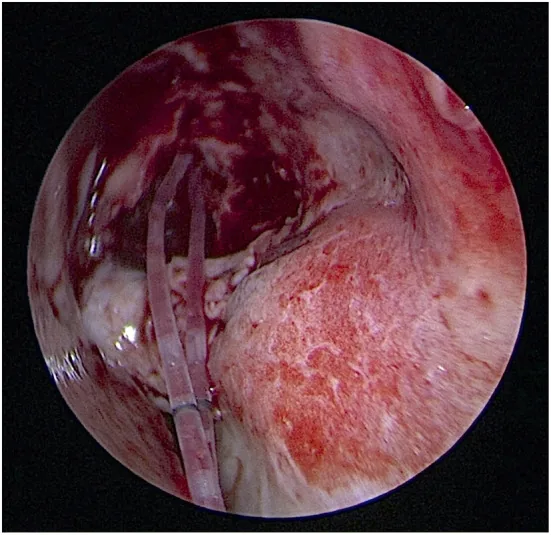
Lee W, et al. Endoscopic dacryocystorhinostomy with short-term, pushed-type bicanalicular intubation vs. pulled-type monocanalicular intubation for primary acquired nasolacrimal duct obstruction. Front Med (Lausanne). 2022;9:946083. Figure 2. PMCID: PMC9367212. License: CC BY.
Intraoperative photograph showing the Nunchaku-type bicanalicular silicone stent being pushed from both the upper and lower puncta toward the nasal cavity. This corresponds to the bicanalicular (double-tube) insertion method and the formation of a nasal loop of the silicone tube discussed in the section “Standard Treatment (Surgical Techniques).”
Treatment is selected according to the obstruction site, severity, and the patient’s condition and wishes.
Under topical anesthesia, the punctum is incised and dilated using a punctal dilator or a sharp blade. After placing a punctal plug for 2–4 weeks, it is removed. If reocclusion is observed, the punctum is re-incised, and a silicone tube is placed in the canaliculus for 1–2 months and then removed. The success rate 3–12 months after tube removal is reported to be 81.8–100% 1).
Treatment of Canalicular and Common Canalicular Obstruction
After performing intracanalicular anesthesia with 4% lidocaine hydrochloride, the canaliculus is sufficiently dilated with a punctal dilator. A nunchaku-type or catheter-type silicone tube is inserted from the punctum. The tip of the tube should be advanced gradually while carefully feeling the resistance at the obstruction site; do not force it. Metal bougies carry a risk of false passage and must be handled with particular caution. The basic indwelling period is 1–2 months.
Treatment under dacryoendoscopy involves perforating the obstruction with DEP or SEP and inserting a tube using SGI/G-SGI 1). For Grade 1 (common canalicular obstruction), a patency rate of 94% after 878 days has been reported 1). For Grades 2 and 3, the difficulty is significantly higher, and if perforation is difficult, it may be necessary to decide to discontinue the procedure.
For common canalicular obstruction where a trans-punctal approach is not possible, a skin incision approach is used. A 15–20 mm skin incision is made along the anterior lacrimal crest, the lacrimal sac is incised, and under microscopic direct visualization, the common punctum is identified and the obstruction is perforated. The height of the medial canthal tendon serves as a landmark for the location of the common punctum.
Before surgery, thoroughly explain to the patient that the outcomes of tube insertion for nasolacrimal duct obstruction are not favorable. The reocclusion rate is high (45–80%) when complicated by chronic dacryocystitis. In cases with acute dacryocystitis, plan surgery after incision and drainage and anti-inflammatory treatment with antibiotics.
The obstruction is perforated using DEP or SEP, and a tube is guided into the nasal cavity and inserted using SGI/G-SGI. The tube indwelling period is 2–12 months. The success rate at 1 year after removal is 70–87% 1), and the patency rate at 3,000 days after tube removal is 64%, indicating a long-term risk of recurrence 1). Risk factors for recurrence include a history of dacryocystitis, long disease duration, long obstruction length, and male sex 1).
Technique: The dacryoendoscopy probe itself is used as a bougie to directly perforate the obstruction.
Features: Simple technique. Allows simultaneous observation and perforation, but since no sheath is used, tube insertion requires a separate SGI method.
Indications: Cases where the obstruction site is clear and the direction of perforation can be ensured.
SEP (sheath-guided endoscopic probing)
Procedure: A Teflon lacrimal sheath is attached as an outer tube, and the tip of the sheath is used to perforate the obstruction.
Features: Perforation is possible while observing the lumen. After perforation, the procedure can be directly transitioned to tube insertion using SGI.
Indications: Cases where careful confirmation of the perforation direction is necessary. It can reduce the risk of submucosal misinsertion.
SGI (sheath-guided intubation) is a method in which a sheath is placed in the lacrimal duct, the tube is connected inside the sheath, and then the sheath is pulled out from the nasal cavity to guide the tube into the nasal cavity. Direct tube insertion (DSI) has been reported to have a 22% rate of submucosal misinsertion 1), so the SGI method is recommended.
G-SGI is a modification of SGI that does not require intranasal manipulation. The sheath has a slit line that allows it to be removed from the punctum side, reducing pain and complication risks associated with inserting instruments into the nasal cavity.
When inserting the endoscope, be aware of the structures such as the vertical and horizontal parts of the canaliculus. By pulling the eyelid outward to straighten the canaliculus, you can reach the lacrimal sac almost linearly from the superior punctum. Infuse irrigation fluid slowly; avoid rapid infusion pressure as it may induce pain.
QHow long is the tube left in place?
A
It depends on the site of obstruction. For punctum or canalicular obstruction, tube placement of 1–2 months has been reported; for nasolacrimal duct obstruction, 2–12 months. Long-term placement (9 months or more) increases the risk of cheese-wiring (punctal laceration) and granulation formation, so timely removal is important. Determining the optimal removal time based on lacrimal endoscopic findings is expected in the future.
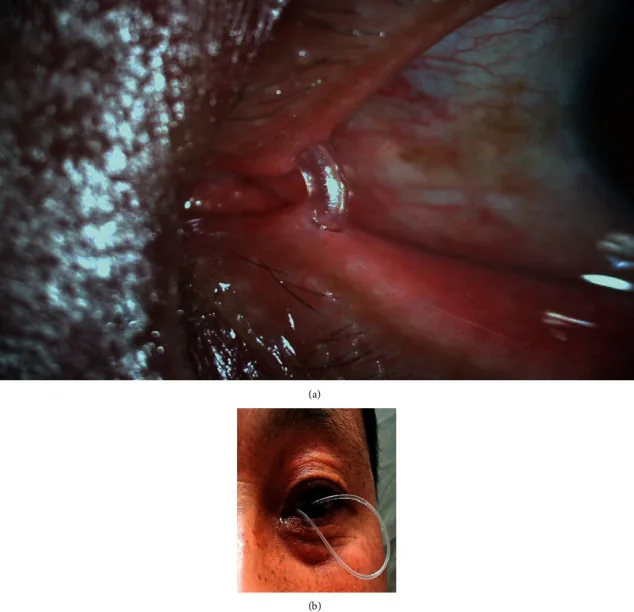
Zhang J, et al. Repositioning of the Severe Prolapsed Silicone Tubes after Bicanalicular Nasal Intubation: A Novel Technique. J Ophthalmol. 2021;2021:6669717. Figure 1. PMCID: PMC7960063. License: CC BY.
Clinical photograph of a silicone tube that has prolapsed in a large loop from the inner canthus to the anterior corneal surface after lacrimal tube intubation. This corresponds to the management of complications during tube placement such as tube prolapse and cheese-wiring, discussed in the section “Complications and Postoperative Management.”
The main complications associated with lacrimal endoscopic surgery and tube intubation are listed below1).
Complication
Timing of Occurrence
Management
Mucosal tear formation
Intraoperative
Confirm subcutaneous edema and discontinue surgery
Mucosal laceration is the most important intraoperative complication to be aware of during lacrimal endoscopy. If subcutaneous edema (eyelid swelling) occurs, surgery should be stopped immediately.
Submucosal misinsertion commonly occurs on the nasal side of the lower lacrimal sac. It can cause postoperative epistaxis or orbital cellulitis. The incidence can be reduced by the SGI/G-SGI method, but if it occurs, tube removal and reoperation are often required.
Cheese wiring is a complication in which the punctum is slit-like torn toward the horizontal portion of the canaliculus. Excessive punctal incision or dilation is a trigger. It has been reported that it occurred in all 3 cases with long-term indwelling of 9 months or more 1), and removal within an appropriate period is essential.
Granulation formation occurs at the site of contact with the tube. It is managed with steroid eye drops and often disappears within one month after removal.
Dacryocystitis / infectious keratitis is caused by bacterial proliferation (Moraxella lacunata, Streptococcus, Pseudomonas aeruginosa, etc.) due to long-term indwelling. In addition to antibiotic administration, tube removal may be necessary.
Orbital cellulitis-like skin swelling occurs when bacteria from the lacrimal sac spread into the orbit due to submucosal misinsertion. Intravenous antibiotics and immediate tube removal are necessary.
After tube removal, patency is confirmed by regular lacrimal irrigation. For nasolacrimal duct obstruction, there is a risk of reocclusion over the long term, so follow-up should continue to monitor for recurrence of tearing symptoms. In case of reocclusion, consider tube reinsertion or conversion to DCR.
QWhat is the success rate of tube insertion surgery?
A
It varies greatly depending on the site of obstruction. For punctual obstruction, success rates are 81.8–100%; for canalicular obstruction grade 1, 94% at 878 days. For nasolacrimal duct obstruction, rates are 70–87% at 1 year after tube removal, but decrease to 64% at 3,000 days. In cases with chronic dacryocystitis, the reocclusion rate is high at 45–80%, and it is important to explain the difference in outcomes compared to definitive surgery (DCR) to patients.
Tears are drained from the punctum through the canaliculi (superior and inferior) → common canaliculus → lacrimal sac → nasolacrimal duct → opening in the inferior meatus (Hasner’s valve) into the nasal cavity. Obstruction at any site leads to tearing and discharge.
The canaliculus transitions from the punctum to a vertical portion (about 2 mm) and then a horizontal portion (about 8 mm); the superior and inferior canaliculi join to form the common canaliculus. Understanding this structure is fundamental to endoscopic procedures.
Punctal and canalicular obstruction is mainly caused by mucosal scar formation due to Stevens-Johnson syndrome, ocular pemphigoid, chronic inflammation, or post-traumatic adhesions. Anticancer drugs such as TS-1 and 5-FU cause obstruction by directly damaging the canalicular epithelium and inducing inflammation. These drug-induced obstructions primarily involve the canaliculi and are frequently bilateral and affect both upper and lower canaliculi simultaneously2).
Nasolacrimal duct obstruction results from multifactorial causes including age-related fibrosis, chronic inflammation, infection, trauma, and sinus disease, but is often idiopathic. Anatomical narrowing at the entrance of the nasolacrimal duct is thought to contribute. Obstruction leads to accumulation of tears and mucus in the lacrimal sac, promoting bacterial overgrowth (Moraxella lacunata, Streptococcus, Pseudomonas aeruginosa, etc.) and progression to chronic dacryocystitis.
Canalicular obstruction may recur even after successful recanalization. Prognosis depends on the degree of obstruction, cause of inflammation, and disease activity. Risk factors for recurrence include history of dacryocystitis, long disease duration, long obstruction segment, and male sex1).
With the spread of G-SGI (a modified SGI that does not require intranasal manipulation), the pain and complication risks associated with inserting instruments into the nasal cavity are being reduced 1).
Improvements in lacrimal endoscope pixel count (from 6,000 to 10,000 pixels) and depth of focus (1.5–7 mm) have enabled detailed observation of obstruction sites and postoperative monitoring 1). Optimal timing for tube removal based on lacrimal endoscopic findings is expected in the future 1).
For refractory cases where both upper and lower canaliculi cannot be opened, Jones tube (CDCR) or conjunctivodacryocystorhinostomy (lacrimal sac transposition) are being considered as options 1). Conjunctivodacryocystorhinostomy has been reported to improve epiphora in all cases at one year postoperatively 1).
Optimizing the indwelling period for chemotherapy-related lacrimal duct obstruction is also a challenge; it is recommended not to remove the tube during ongoing treatment to prevent re-obstruction 2).
Sobel RK, Aakalu VK, Wladis EJ, Bilyk JR, Yen MT, Mawn LA. A Comparison of Endonasal Dacryocystorhinostomy and External Dacryocystorhinostomy: A Report by the American Academy of Ophthalmology. Ophthalmology. 2019;126(11):1580-1585. doi:10.1016/j.ophtha.2019.06.009.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.