Lens-induced glaucoma is a general term for secondary glaucoma in which abnormal lens position, volume changes, or protein leakage cause elevated intraocular pressure. It is classified into angle-closure type and open-angle type based on the mechanism of angle closure 1)2).
Cases where the lens is the direct cause of angle closure account for approximately 5% of all angle-closure glaucoma1). Intumescent cataract and anterior displacement due to lens subluxation are representative conditions 1).
In the 5th edition of the Glaucoma Clinical Practice Guidelines, lens-induced glaucoma is positioned as secondary glaucoma as follows 2).
Secondary open-angle glaucoma: When the main site of aqueous outflow resistance is in the trabecular meshwork, such as obstruction by lens material
Secondary angle-closure glaucoma: Due to pupillary block from intumescent lens or lens dislocation, and direct angle closure from intumescent lens or lens dislocation via mechanisms other than pupillary block
This disease is classified into the following five types.
1. Lens-induced secondary angle-closure glaucoma
Phacomorphic glaucoma: Lens swelling due to progression of cataract
Glaucoma due to lens displacement: Pupillary block caused by subluxation or dislocation of the lens
Glaucoma due to spherophakia: Pupillary block caused by abnormal lens shape
2. Lens-induced secondary open-angle glaucoma
Phacolytic glaucoma: Protein leakage from hypermature cataract
Lens-particle glaucoma: Release of lens material after surgery or trauma
Phacoanaphylactic glaucoma: Immune reaction to lens proteins
The EGS 6th edition classifies lens-induced open-angle glaucoma into three types: phacolytic glaucoma, glaucoma due to traumatic lens injury, and phacoanaphylactic glaucoma3).
QWhat is the difference between phacomorphic glaucoma and phacoanaphylactic glaucoma?
A
Phacomorphic glaucoma is an angle-closure type in which the lens swells due to progression of cataract, pushing the iris forward and causing angle closure. In contrast, phacoanaphylactic glaucoma is an open-angle type in which, after the lens capsule is damaged by surgery or trauma, a granulomatous inflammatory reaction to lens proteins obstructs the trabecular meshwork. In the former, the physical size of the lens is the problem; in the latter, an immune reaction is the cause.
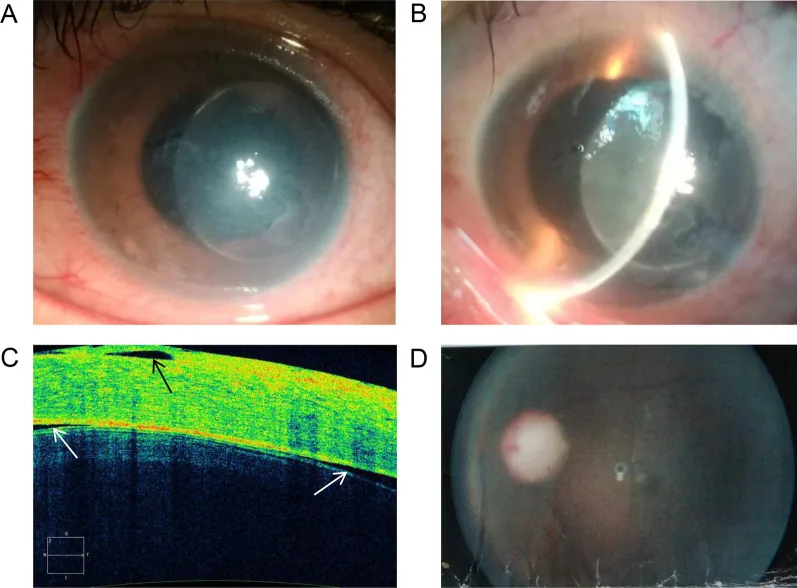
Manhua Xu; Kaiming Li; Weimin He. Compound heterozygous mutations in the LTBP2 gene associated with microspherophakia in a Chinese patient: a case report and literature review. BMC Med Genomics. 2021 Sep 17;14:227. Figure 3. PMCID: PMC8449461. License: CC BY.
This figure summarizes clinical findings including anterior segment changes and corneal edema associated with cataract. It shows findings of shallow anterior chamber and corneal opacity due to swollen or leaking lens.
Subjective symptoms of lens-induced glaucoma vary depending on the disease type.
Angle-closure type (swelling/displacement): Presents with symptoms similar to acute glaucoma attack. Accompanied by sudden eye pain, vision loss, redness, headache, nausea, and vomiting 2)
Phacolytic glaucoma: Presents with sudden eye pain, redness, and high intraocular pressure with corneal edema. Characterized by deep anterior chamber and presence of hypermature cataract.
Lens particle glaucoma: Develops after cataract surgery, trauma, or YAG laser capsulotomy. High intraocular pressure is observed for days to weeks, but is often transient.
Phacoanaphylactic glaucoma: Develops 1 to 14 days after surgery or trauma, presenting with ciliary injection and blurred vision.
Redness is perceived in various secondary glaucomas including phacolytic glaucoma2). In open-angle type, blurred vision and photophobia may also be present 3).
Clinical findings (findings confirmed by physician examination)
Findings in glaucoma due to lens dislocation: Uneven peripheral anterior chamber depth, iridodonesis (iris trembling due to loss of lens support), and phacodonesis. Under mydriasis, lens displacement, tilt, and uneven curvature of the lens capsule are observed. Among hereditary disorders, Marfan syndrome often shows superotemporal displacement, while homocystinuria and Weil-Marchesani syndrome frequently show inferior displacement. In posterior lens dislocation (fall into the vitreous), pupillary block by the vitreous can cause a rapid increase in intraocular pressure.
Findings in phacomorphic glaucoma: The affected eye shows mature cataract and shallow anterior chamber. The contralateral eye often has normal anterior chamber depth, which is an important distinguishing point from primary angle-closure glaucoma. Myopic shift (change in refractive value) with cataract progression is also a useful finding for differentiation. Age-related cases gradually close the angle, but in young or traumatic cases, it may progress rapidly.
Findings in phacolytic glaucoma: The anterior chamber is deep, accompanied by hypermature cataract. Scintillating opacity is observed in the anterior chamber. The absence of keratic precipitates (KP) is important for differentiation from phacoanaphylactic glaucoma. Pseudohypopyon (layered lens protein in the inferior anterior chamber) may also be seen. However, if granulomatous anterior uveitis with mutton-fat KP is present, differentiation from phacoanaphylactic glaucoma becomes difficult.
Findings in lens cortex glaucoma: Characteristically, relatively large white particles float in the anterior chamber. Onset is often days to weeks after the trigger (surgery or trauma), but may occur months later.
Findings in phacoanaphylactic glaucoma: Ciliary injection, mutton-fat KP, and anterior chamber cells/flare are observed, presenting findings of persistent granulomatous anterior uveitis.
Lens swelling: As cataracts progress, the lens becomes liquefied and swollen, increasing its anteroposterior diameter. This mechanically pushes the iris forward, causing pupillary block. The mechanism of relative pupillary block is also involved.
Lens dislocation: Pupillary block caused by a subluxated or dislocated lens or prolapsed vitreous leads to increased intraocular pressure. In traumatic dislocation, angle damage may also contribute. If the lens falls into the vitreous cavity, pupillary block by the vitreous can occur.
Spherophakia: The lens becomes thicker, causing pupillary block. Weakness of the zonules of Zinn also contributes to angle closure due to anterior displacement.
Causes of Open-Angle Glaucoma
Phacolytic glaucoma: Spontaneous capsular rupture of a hypermature cataract leads to leakage of lens material 1). Macrophages that have phagocytosed lens cortex and high-molecular-weight soluble proteins obstruct the trabecular meshwork3).
Retained lens material: After cataract surgery or trauma, lens material may be released and obstruct the trabecular meshwork3). The increase in intraocular pressure is proportional to the amount of retained lens fragments.
Phacoanaphylaxis: Granulomatous inflammation due to type III allergy (Arthus immune complex reaction) to lens proteins obstructs the trabecular meshwork3).
The following are representative genetic disorders that cause lens dislocation. All are due to abnormalities of the zonules of Zinn, and subluxation or dislocation of the lens increases the risk of secondary angle-closure glaucoma.
Marfan syndrome: Mutation in the FBN1 gene (fibrillin-1). Characteristically, the lens is displaced superotemporally.
ADAMTSL4 gene mutation: Recessive mutations have been identified as a cause of isolated ectopia lentis. ADAMTSL4 promotes the biosynthesis of fibrillin-1 microfibrils and is involved in the formation of the zonules of Zinn 6).
Lens abnormalities associated with glaucoma include abnormalities in lens size or shape (e.g., intumescent lens, spherophakia) and abnormalities in lens position (e.g., dislocation, subluxation). Abnormalities in lens position may involve abnormalities of the ciliary zonules (congenital, traumatic, exfoliation glaucoma, etc.) 2).
QWhy does the lens become dislocated in Marfan syndrome?
A
Marfan syndrome is caused by mutations in the FBN1 gene (encoding fibrillin-1). Fibrillin-1 is a major structural protein of the zonules of Zinn; mutations lead to weakening and rupture of the zonules, resulting in lens dislocation. In Marfan syndrome, dislocation is typically upward and temporally. Anterior dislocation of the lens can cause pupillary block and lead to secondary angle-closure glaucoma.
Evaluate the lens condition (intumescent, hypermature, dislocated, spherophakia), anterior chamber depth, cells and flare in the anterior chamber, and presence of keratic precipitates (KP) 2). Assessment of peripheral anterior chamber depth using the van Herick method is useful for screening angle closure 2). In spherophakia, note the steep anterior curvature of the lens; diagnosis is made by observing a small, spherical lens after dilation.
This examination is essential for differentiating between angle-closure and open-angle types. In phacomorphic glaucoma, extensive angle closure is observed, and the difference in angle opening between the two eyes is useful for diagnosis. In open-angle types, the angle is open but may show deposition of lens material or macrophages on the trabecular meshwork.
Anterior segment OCT and ultrasound biomicroscopy (UBM) are useful for detailed assessment of the lens and angle. In phacomorphic glaucoma, the mass effect of the lens on the iris can be observed. In spherophakia, abnormal lens shape can be evaluated. Lens vault (LV) is one of the parameters used in anterior segment imaging assessment 2).
For posterior dislocation of the lens (into the vitreous cavity), B-mode ultrasound can confirm the dislocated lens.
Differentiation between phacomorphic glaucoma and primary angle-closure glaucoma: The presence of intumescent cataract, anterior chamber depth of the contralateral eye (normal in phacomorphic, shallow in primary angle closure), and myopic shift with cataract progression (change in refractive value) are important differentiating points.
Differentiation between phacolytic glaucoma and phacoanaphylactic glaucoma: In phacolytic glaucoma, the anterior chamber is deep, hypermature cataract is present, and no keratic precipitates are seen. In phacoanaphylactic glaucoma, granulomatous anterior uveitis with mutton-fat keratic precipitates is observed.
Initial medical treatment: Instill cycloplegics (e.g., atropine) to move the lens posteriorly and relieve pupillary block. Lower intraocular pressure with beta-blockers (e.g., 0.5% timolol maleate) and carbonic anhydrase inhibitors (e.g., 1% brinzolamide eye drops, or acetazolamide 10 mg/kg IV or oral 2)).
Hyperosmotic agents2): Intravenous infusion of 20% mannitol 1.0–2.0 g/kgBW over 30–60 minutes (minimum IOP reached 60–90 minutes after start, effect lasts 4–6 hours). Intravenous infusion of glycerol 300–500 mL over 45–90 minutes (minimum IOP reached 30–135 minutes after start, effect lasts about 5 hours).
Miotics are contraindicated: They contract the ciliary muscle, relax the zonules, and promote forward movement of the lens, so they must not be used.
Definitive surgery: For intumescent cataract, perform phacoemulsification (PEA) with intraocular lens (IOL) implantation. For lens subluxation, perform intracapsular or extracapsular extraction. For spherophakia, intracapsular extraction is necessary due to zonular weakness.
Treatment of Open-Angle Type
Preoperative drug therapy: Anti-inflammatory treatment with steroid eye drops and cycloplegics, and lowering intraocular pressure with beta-blocker eye drops and carbonic anhydrase inhibitors (eye drops or oral) 1)
Phacolytic glaucoma: Removal of the lens (cataract surgery) is essential. The EGS 6th edition also recommends removal of the lens or lens fragments 3)
Lens particle glaucoma: If anti-inflammatory and intraocular pressure-lowering drugs are ineffective, perform anterior chamber irrigation to completely remove residual lens cortex.
Phacoanaphylactic glaucoma: If anti-inflammatory and intraocular pressure-lowering drugs are ineffective, perform surgical removal of residual lens material. Vitrectomy may be combined as needed 3)
Treatment of secondary glaucoma should prioritize treatment of the underlying cause whenever possible, and select treatment based on the mechanism of intraocular pressure elevation 2). Phacolytic glaucoma and angle-closure glaucoma due to intumescent cataract are surgical indications aimed at treating lens-related complications.
Caution regarding laser iridotomy (LI) for intumescent cataract: If the anterior capsule is perforated during LI, phacolysis may occur, leading to inflammatory intraocular pressure elevation. For intumescent cataract, it is preferable to directly choose lens reconstruction surgery.
Management of posterior lens dislocation: A lens that has fallen into the vitreous cavity can be observed conservatively as long as it does not undergo phacolysis. If rapid intraocular pressure elevation occurs, consider vitrectomy.
Precautions for using hyperosmotic agents2): Mannitol carries a risk of acute renal failure in patients with renal impairment. Glycerol produces glucose during metabolism, so caution is needed in diabetic patients. Both increase circulating plasma volume systemically, posing a risk of pulmonary edema in patients with heart failure or pulmonary congestion.
QWhy are miotics contraindicated in lens-induced glaucoma?
A
In angle-closure lens-induced glaucoma, miotics contract the ciliary muscle, relaxing the zonules and causing the lens to move further forward, worsening pupillary block. Conversely, cycloplegics (e.g., atropine) relax the ciliary muscle, tightening the zonules and moving the lens backward, helping to relieve pupillary block.
6. Pathophysiology and Detailed Mechanism of Onset
In lens-induced angle-closure glaucoma, changes in the position or volume of the lens cause angle closure. The mechanism of pupillary block is primarily involved 2).
Mechanism due to lens swelling (phacomorphic glaucoma): As cataract progresses, the lens cortex becomes liquefied and the lens swells. The increase in anteroposterior diameter mechanically pushes the iris forward, and the mechanism of relative pupillary block also contributes to angle-closure glaucoma. Age-related cases gradually close the angle, but in young or traumatic cases, it progresses rapidly. Abnormal lens position or increased lens thickness due to cataract progression can cause angle closure 2).
Mechanism due to lens displacement: Displaced lens (subluxation, dislocation) or prolapsed vitreous causes pupillary block, leading to acute or chronic angle-closure glaucoma. In traumatic displacement, angle damage from trauma can also cause elevated intraocular pressure. In posterior dislocation of the lens (fall into the vitreous), pupillary block by the vitreous can cause a rapid rise in intraocular pressure. Forward movement of the lens-iris diaphragm causes angle closure 1).
Mechanism due to spherophakia: In spherophakia, the lens thickness increases, causing pupillary block. In eyes with spherophakia, the zonules are also fragile, and the mechanism of angle closure due to forward displacement of the lens is also involved.
In lens-induced open-angle glaucoma, the outflow pathway of the trabecular meshwork is obstructed by lens particles and/or inflammatory cells 3).
Phacolytic glaucoma: Lens material leaks through the capsule from mature or hypermature cataracts 3). The main mechanism is obstruction of the trabecular meshwork by macrophages that have phagocytosed lens cortex, but high-molecular-weight soluble proteins themselves can also cause obstruction. Mature or hypermature cataracts may be accompanied by leakage of lens material and complicated by phacolytic glaucoma2).
Lens-particle glaucoma: After cataract surgery, trauma, or YAG laser posterior capsulotomy, lens material is released and obstructs the trabecular meshwork, causing elevated intraocular pressure. It develops within days after surgery or trauma. The rise in intraocular pressure is proportional to the amount of lens fragments remaining in the anterior chamber.
Phacoanaphylactic glaucoma: After damage to the lens capsule due to surgery or trauma, a type III allergic reaction (Arthus-type immune complex reaction) to lens proteins causes granulomatous inflammation 3). It is a granulomatous uveitis that develops weeks after trauma, cataract surgery, or spontaneous rupture of the capsule in hypermature cataracts, when lens proteins leak into the aqueous humor and break immune tolerance. Pathologically, macrophages and neutrophils accumulate around residual lens cortex, and if inflammation persists, a cyclitic membrane forms.
Details of the mechanism by which miotics are contraindicated
The pharmacological mechanism in angle-closure type is as follows.
Cycloplegics: Relaxation of ciliary muscle → Tension of zonules → Posterior movement of lens → Release of pupillary block
Miotics: Contraction of ciliary muscle → Relaxation of zonules → Anterior movement of lens → Worsening of pupillary block
This mechanism differs from drug selection during acute attack treatment in primary angle-closure glaucoma and is a unique consideration for lens-induced glaucoma, where changes in lens position are central to the pathology.
In familial ectopia lentis, dislocation of intraocular lenses can be a recurrent complication.
Scleral fixation using a sutureless Carlevale lens has been reported for recurrent intraocular lens dislocation in patients with familial ectopia lentis4). In young patients, zonular fragility is a long-term issue, so sutureless fixation is expected to reduce postoperative complications.
Cataract surgery using a portable femtosecond laser under general anesthesia has been performed in children with spherophakia and ectopia lentis5). The femtosecond laser can create a precise capsulotomy without excessive traction on fragile zonules, resulting in high capsular preservation rates. It may be a useful technique for cataract surgery in children with ectopia lentis.
Recessive mutations in the ADAMTSL4 gene have been reported to cause craniosynostosis and ectopia lentis6). ADAMTSL4 is a protein that promotes the biosynthesis of fibrillin-1 microfibrils, and its loss of function is proposed to simultaneously cause zonular disruption (ectopia lentis) and abnormal TGFβ signaling (craniosynostosis). Elucidation of the molecular mechanism of ectopia lentis may contribute to the development of future gene therapies.
Early Lens Extraction After Acute Angle-Closure Attack
According to the consensus statement of the Asia Pacific Glaucoma Society (APGS), laser iridotomy (LPI) alone for acute primary angle-closure attack (APACA) results in long-term intraocular pressure elevation in up to 58% of cases, progressing to chronic angle-closure glaucoma. Therefore, early lens extraction, which is more curative, is recommended 7). When lens thickening is the main cause of angle closure, this finding can also be applied to the management of lens-induced glaucoma. A safe surgical window is considered to be 1–3 months after the attack subsides 7).
QWhat is the prognosis of lens-induced glaucoma?
A
If the lens is removed at the appropriate time, good intraocular pressure control can be achieved in many cases. However, if glaucomatous optic neuropathy has progressed due to prolonged high intraocular pressure or inflammation, recovery of visual function is difficult. Phacolytic glaucoma and lens-induced glaucoma due to lens swelling are considered to have relatively good prognoses, but hereditary diseases with lens dislocation may require repeated surgeries. Glaucoma due to retained lens material is often transient.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Wilczyński TK, Niewiem A, Leszczyński R, Michalska-Malecka K. Recurrent Intraocular Lens Dislocation in a Patient with Familial Ectopia Lentis. Int J Environ Res Public Health. 2021;18(9):4545.
Kalra N, Agarwal R, Agarwal T, Sinha R. Portable femtosecond laser assisted cataract surgery in a child with bilateral ectopia lentis with microspherophakia. Am J Ophthalmol Case Rep. 2022;26:101442.
Gustafson J, Bjork M, van Ravenswaaij-Arts CMA, Cunningham ML. Mechanism of Disease: Recessive ADAMTSL4 Mutations and Craniosynostosis with Ectopia Lentis. Case reports in genetics. 2022;2022:3239260. doi:10.1155/2022/3239260. PMID:35378950; PMCID:PMC8976637.