Lens dislocation and subluxation (ectopia lentis) are general terms for conditions in which the lens is displaced from its normal position. When the lens is partially displaced but remains within the lens capsule, it is called subluxation; when it moves completely into the vitreous cavity or anterior chamber, it is called luxation/dislocation.
Both are caused by weakening or rupture of the zonules of Zinn (ciliary zonules). Congenital positional abnormalities are sometimes distinguished as ectopia lentis, while acquired ones are referred to as lens subluxation/dislocation.
Congenital lens displacement is almost always bilateral. It is often hereditary or associated with underlying diseases, including systemic conditions such as Marfan syndrome, homocystinuria, and Weill-Marchesani syndrome. In Marfan syndrome (MFS), approximately 60–80% of patients have lens displacement 1), making it the most common cause of hereditary lens displacement. The global prevalence of MFS is estimated to be about 1 in 3,000–5,000 people 6).
Among acquired causes, trauma is the most common. In traumatic lens dislocation, blunt trauma causes rapid expansion of the eyeball in the equatorial direction, leading to rupture of the zonules. Other causes include exfoliation syndrome, after vitreous surgery, high myopia, mature cataract, and uveitis.
Genetic analysis of congenital lens displacement has identified SUOX mutations in 0.76% of cases as a cause other than FBN1 4), indicating the presence of diverse genetic backgrounds.
QIs lens displacement always hereditary?
A
Congenital lens displacement is often associated with hereditary diseases, but in acquired cases, trauma is the most common cause and is unrelated to heredity. If lens displacement occurs despite minor trauma, the presence of an underlying disease that weakens the zonules should be considered.
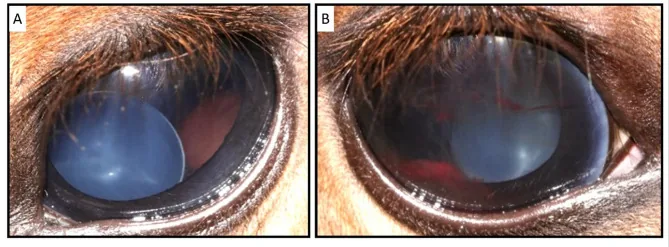
Esdaile E, et al. A de novo FBN1 variant likely causes congenital bilateral ectopia lentis in a crossbred horse. Sci Rep. 2025. Figure 1. PMCID: PMC12552744. License: CC BY.
Anterior segment photograph showing the lens displaced from its normal position within the pupil. This image directly shows a representative clinical finding of lens dislocation/subluxation.
Monocular diplopia: When the lens margin overlaps the pupillary area, the refractive difference between the phakic and aphakic portions causes this symptom.
Refractive fluctuation: Instability of the lens may cause diurnal variation.
Eye pain and sudden vision loss: Occurs abruptly in acute dislocation into the anterior chamber.
Dislocation into the anterior chamber can cause acute angle-closure glaucoma, requiring emergency management. Kondo et al. (2022) reported a case of a man in his 70s presenting with sudden vision loss and severe headache, diagnosed with acute angle-closure glaucoma due to lens dislocation5).
Even with minimal displacement, note that after an uneventful childhood, shallow anterior chamber may develop in adulthood and lead to acute angle closure.
Phacodonesis: Oscillation of the lens with eye movement. Important as an early sign of zonular weakness.
Iridodonesis: Vibration of the iris with rapid eye movement. Suggests posterior displacement.
Shallow anterior chamber / Asymmetry of anterior chamber depth: Uneven anterior chamber depth due to displaced lens. Suspect zonular weakness on the shallower side.
Iris shape abnormality: Complicated by iridodialysis, or iris deformation due to displaced lens.
Findings of Complete Dislocation
Anterior chamber dislocation: The lens prolapses into the anterior chamber, causing a rapid rise in intraocular pressure. Emergency management is required.
Vitreous drop: The lens falls into the vitreous cavity. On supine CT, it presents as a floating lens sign.
Phacocele: A rare finding where the lens dislocates under the conjunctiva or Tenon’s capsule due to scleral rupture.
When dislocated into the anterior chamber, attention should be paid to the following complications.
Pupillary block: The lens moves anterior to the pupil and blocks aqueous humor circulation. This can cause secondary angle-closure glaucoma.
Corneal endothelial damage: The lens directly contacts the cornea, causing Descemet membrane detachment and corneal edema (lens-endothelial touch).
Lens-induced uveitis: If the lens falls into the vitreous cavity, inflammation and increased intraocular pressure may occur due to the nucleus and cortex.
QWhat is lens phacodonesis?
A
When the zonules of Zinn are weak, the lens trembles slightly with eye movements. This can be observed with a slit lamp and is an important sign of zonular rupture. It occurs similarly in both traumatic and congenital cases.
Other related conditions include sulfite oxidase deficiency (ISOD), Ehlers–Danlos syndrome, and exfoliation syndrome.
LTBP2 mutation: Encodes a protein essential for the development of ciliary zonule microfibrils. LTBP2 deficiency leads to zonular rupture and lens dislocation3).
ISOD (Sulfite Oxidase Deficiency): A rare metabolic disease caused by SUOX mutation. It accounts for 0.76% of congenital EL cohorts4), and the direction of displacement is similar to Marfan syndrome (upward), making genetic testing useful for differentiation.
Trauma: The most common cause. Blunt trauma causes eyeball deformation, rupturing the zonules. Typical causes include sports injuries, fights, and traffic accidents. Often accompanied by iridodialysis.
After vitrectomy: Zonular weakness may progress during peripheral vitrectomy.
High myopia: May be associated with zonular weakness. Also be aware of the risk of nucleus drop.
Others: Mature cataract, uveitis, after laser iridotomy, idiopathic (sporadic in the elderly).
QWhy do Marfan syndrome and homocystinuria differ in the direction of displacement?
A
The difference in displacement direction is due to differences in the pattern of zonular damage. In Marfan syndrome, structural abnormalities of fibrillin-1 cause the zonules to weaken from above, leading to upward displacement. In homocystinuria, excess homocysteine damages the disulfide bonds of the zonules, and due to gravity, downward displacement is more common.
Slit-lamp examination is the most important. Under mydriasis, evaluate the degree and direction of lens displacement, and check for iridodonesis, phacodonesis, and vitreous prolapse. Systemic evaluation for cardiovascular and skeletal abnormalities should also be performed.
Observation before mydriasis: After mydriasis, relaxation of the ciliary muscle increases tension on the zonules of Zinn, which may mask phacodonesis. Pay attention to iridodonesis before dilation.
Observation under mydriasis: Evaluate the direction, degree, and tilt of lens displacement. In Marfan syndrome, upward displacement is typical; in homocystinuria, downward and nasal displacement are typical. The lens edge and ruptured zonules of Zinn can be observed.
Useful for confirming intra-vitreal dislocation. Also applicable when fundus is not visible due to hyphema.
Retinal tears or detachments were found in 37.7% of patients with traumatic lens dislocation/subluxation requiring vitrectomy, but only 8.9% were identified preoperatively. Thorough preoperative evaluation is important.
Mild cases are managed with refractive correction using glasses and followed up. Especially in children, early refractive correction is important for prevention of amblyopia; in cases with significant interocular difference, amblyopia treatment including occlusion of the healthy eye should be initiated early. As long as correction with glasses or contact lenses is possible, follow-up is continued; if there is a difference in visual acuity between eyes, amblyopia treatment such as occlusion of the healthy eye is added.
If pupillary block occurs, mydriatic agents are used (miotics are contraindicated). For pupillary blockglaucoma, laser iridotomy is considered. For anterior dislocation, temporarily lower intraocular pressure with acetazolamide and proceed to surgery.
Visual impairment difficult to correct due to lens displacement or deformation
Progression of lens displacement
Glaucoma attack
Complete dislocation into the vitreous cavity is not an active surgical indication unless complications such as glaucoma, endophthalmitis, or retinal edema are present.
Surgical indications in children are considered only when spectacle correction is insufficient, there is a strong interocular difference in visual acuity, or there is interference with school performance.
The surgical procedure varies depending on the extent of zonular rupture and the degree of displacement.
Phacoemulsification (PEA) + CTR: Indicated when zonular dialysis is localized. If the dialysis involves more than one quadrant, use of a capsular tension ring (CTR) is recommended. Irrigation flow should be set low, and hydrodissection should be minimized.
Intracapsular cataract extraction (ICCE): For cases with severe lens displacement making capsulorhexis difficult, or for anterior chamber dislocation. Adequate management of vitreous prolapse is necessary.
Pars plana vitrectomy (PPV) + lensectomy: For complete dislocation into the vitreous cavity. Another method involves using liquid perfluorocarbon (LPFC) to float the lens to the iris plane and then remove it via a transscleral or corneal approach.
IOL fixation: If the IOL cannot be fixated within the capsular bag, ciliary sulcus suturing or intrascleral fixation (e.g., sutureless Yamane technique) is performed. In young patients, high iris elasticity requires caution to avoid postoperative pupil capture.
Congenital lens displacement in children: Lensectomy and anterior vitrectomy (capsular bag is removed). Postoperative refractive correction with contact lenses or glasses and continued amblyopia therapy are required.
QIs it possible to observe without surgery?
A
In mild cases with little visual impairment, observation with spectacle correction is possible. However, if progression of displacement, glaucoma attack, or cataract occurs, surgery is indicated. In children, prevention of amblyopia is especially important, and regular ophthalmologic follow-up is essential.
The lens is supported by the zonules of Zinn (ciliary zonules). The zonules are composed of microfibrils primarily made of fibrillin-1, maintaining the correct position and accommodative function of the lens.
Fibrillin-1 is an extracellular matrix glycoprotein encoded by the FBN1 gene. In Marfan syndrome, FBN1 mutations cause degeneration of fibrillin microfibrils, leading to zonular weakness and structural abnormalities of the lens capsule1).
Vitale et al. (2025) reported that IGF-1 is an important regulator of fibrillin-1 synthesis and degradation 2). Signaling through the IGF-1 receptor is involved in fibrillin-1 production, and chronic GH/IGF-1 excess may promote dysfunction of the lens suspensory apparatus.
In homocystinuria, CBS deficiency leads to accumulation of homocysteine. The zonules of Zinn are composed of cysteine-rich microfibrils, and excess homocysteine abnormally modifies intramolecular disulfide bonds. This makes the zonules vulnerable to proteolytic degradation and rupture 4).
Mechanism of Isolated Sulfite Oxidase Deficiency (ISOD)
In sulfite oxidase deficiency due to SUOX mutations, sulfite and its metabolites accumulate. Sulfite reacts with disulfide bonds in the zonules in vivo to form S-sulfonates, impairing the structural integrity of the zonules and causing lens dislocation 4).
LTBP2 is an essential protein for the development of ciliary zonule microfibrils. LTBP2 deficiency leads to fragmentation of the zonules of Zinn and causes lens dislocation 3).
In traumatic lens dislocation due to blunt trauma, anteroposterior compressive forces on the cornea and anterior sclera cause rapid compensatory equatorial expansion of the globe. When this expansion force exceeds the resistance of the zonules of Zinn, rupture occurs. Partial rupture results in subluxation (lens tremors, iridodonesis, shallow anterior chamber), while complete circumferential rupture leads to total dislocation (into the anterior chamber or vitreous cavity).
It has been reported that 58.5% of eyes with zonular dehiscence of 6 clock hours or more had elevated intraocular pressure at initial examination, of which 54.2% presented with acute angle closure. The mechanisms of secondary glaucoma are as follows.
Pupillary block: Acute or chronic angle closure due to anterior subluxation.
Phacolytic glaucoma: Trabecular meshwork obstruction due to leakage of lens proteins
Vitreous prolapse into the anterior chamber: Mechanical obstruction of the trabecular meshwork
Lens-induced uveitis (LIU) occurs due to post-traumatic protein leakage and lens capsule rupture, usually within 14 days of trauma, but cases have been reported decades later. Corneal endothelial failure due to anterior subluxation is caused by lens-endothelial touch.
In exfoliation syndrome, exfoliative material deposits on the surface of the zonules of Zinn, promoting proteolysis over time and causing zonular weakness. Approximately 4% of individuals over 70 years of age have concomitant exfoliation glaucoma, and in this group, the risk of zonular damage during cataract surgery is significantly increased.
7. Latest research and future perspectives (reports at the research stage)
A systematic review by Adji et al. (2025) systematically organized the frequency, surgical outcomes, and complication risks of lens dislocation in MFS 6). In MFS, besides lens dislocation, the risks of glaucoma, cataract, and retinal detachment are high, and comprehensive ophthalmic management is recommended. For severe lens dislocation, PPV + lensectomy is often chosen.
Advances in genetic analysis using whole-exome sequencing
Cai et al. (2025) performed WES on cases of congenital lens dislocation and identified mutations in the COL2A1 gene in addition to FBN1 mutations 1). Clinical application of WES may reveal complex genotypes missed by single-gene testing.
Li et al. (2022) reviewed 35 families with SUOX mutations and reported that missense mutations (M+M type) correlated with late-onset and mild phenotypes, while nonsense/frameshift mutations (NF+NF type) resulted in severe ISOD in all cases 4). This finding is useful for prognosis prediction and genetic counseling.
Vitale et al. (2025) reported a case of a 71-year-old woman with idiopathic bilateral lens dislocation as an atypical presentation of acromegaly (GH: 93.22 μg/L) 2). It is suggested that chronic GH/IGF-1 excess may disrupt fibrillin-1, leading to weakening of the zonules.
Advances in IOL Fixation Techniques and Minimally Invasive Surgery
The widespread adoption of sutureless intrascleral fixation techniques (e.g., Yamane technique) has improved the safety and reproducibility of IOL fixation in cases where the capsular bag is unavailable. Application of femtosecond laser is expected to enhance the precision of capsulotomy in subluxated eyes. Toric multifocal IOLs with intrascleral fixation are also being attempted at some centers.
QWhen is genetic testing indicated?
A
Genetic testing is recommended for unexplained lens displacement, especially when it is non-traumatic and bilateral. Whole exome sequencing (WES) or panel-based NGS can comprehensively analyze causative genes such as FBN1, CBS, ADAMTSL4, LTBP2, and SUOX 1)4). Identifying the genotype directly aids in prognosis prediction and screening for systemic complications.
Cai X, Chen W, Xue J, Wang J, Bai Z, Qiang W, et al. Diagnosis of congenital ectopia lentis: a case report and review of the literature. Journal of medical case reports. 2025;19(1):288. doi:10.1186/s13256-025-05266-3. PMID:40542356; PMCID:PMC12181895.
Vitale L, Fatti LM, Bonomi M, et al. Case Report: Bilateral lens dislocation as an atypical presentation of acromegaly and review of the ocular effects of GH/IGF-1 excess. Front Endocrinol. 2025;16:1666425. doi:10.3389/fendo.2025.1666425.
Xu M, Li K, He W. Compound heterozygous mutations in the LTBP2 gene associated with microspherophakia in a Chinese patient: a case report and literature review. BMC Med Genomics. 2021;14:227. doi:10.1186/s12920-021-01080-0.
Li JT, Chen ZX, Chen XJ, Jiang YX. Mutation analysis of SUOX in isolated sulfite oxidase deficiency with ectopia lentis as the presenting feature: insights into genotype-phenotype correlation. Orphanet J Rare Dis. 2022;17(1):392. doi:10.1186/s13023-022-02544-x. PMID:36303223; PMCID:PMC9615255.
Kondo K, Isono H. A case of angle-closure glaucoma caused by spontaneous lens dislocation. Clinical case reports. 2022;10(12):e6670. doi:10.1002/ccr3.6670. PMID:36483875; PMCID:PMC9723378.
Adji AS, Billah A, Fadila F, Praja ET, Retno I, Puspitasari A, et al. A systematic review of case series of Marfan syndrome: ocular findings and complications. Rom Med J. 2025;72(1):75-83. doi:10.37897/RMJ.2025.1.11.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.