Wang M, Gao Y, Li R, et al. Monocular lens dislocation due to vomiting-a case report. BMC Ophthalmol. 2018;18(1):3. Figure 1. PMID: 29310625; PMCID: PMC5759281; DOI: 10.1186/s12886-017-0651-8. License: CC BY.
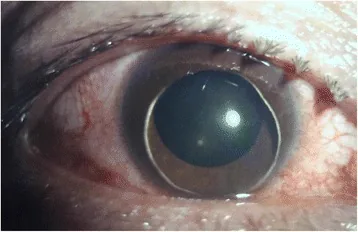
Anterior segment photograph of the right eye showing the lens completely dislocated into the anterior chamber due to circumferential zonular rupture, with marked conjunctival injection. This corresponds to the anterior chamber luxation type of lens dislocation discussed in section “1. What is Traumatic Lens Dislocation?”.
When the support of the zonules of Zinn is lost, it is called lens luxation; when some support remains, it is called lens subluxation. Traumatic lens dislocation and subluxation are general terms for conditions in which the zonules are ruptured by blunt external force, causing displacement of the lens.
They are classified into the following three stages according to severity:
Lens Subluxation
Partial zonular rupture: Some zonules remain intact, and the lens is displaced or tilted but remains within the eye.
Range of symptoms: If the displacement is mild, only refractive error occurs; as it progresses, monocular diplopia and high hyperopia develop.
Phacodonesis: A condition in which the lens shakes during eye movement due to weakness of the zonules of Zinn.
Lens luxation
Complete rupture of the zonules of Zinn: The zonules of Zinn are torn all around, and the lens falls into the vitreous cavity or dislocates into the anterior chamber.
Urgency: In cases of anterior chamber dislocation, it causes a rapid increase in intraocular pressure due to impaired aqueous humor circulation and corneal endothelial damage, requiring emergency treatment.
Vitreous cavity drop: The lens falls into the vitreous cavity due to gravity, and contact with the retina carries a risk of retinal damage.
Traumatic lens dislocation is relatively common as a complication of blunt ocular trauma, and in children it can cause amblyopia. It is differentiated from congenital or systemic disease-related dislocation by history of injury, ocular findings, and systemic findings.
Yang Y, Luo X, Zhong J, Xu X, Zhang H, Cheng B. Traumatic lens subluxation with iridodialysis: a retrospective case series. BMC Ophthalmol. 2024 Feb 14;24:66. Figure 2. PMCID: PMC10865630. License: CC BY.
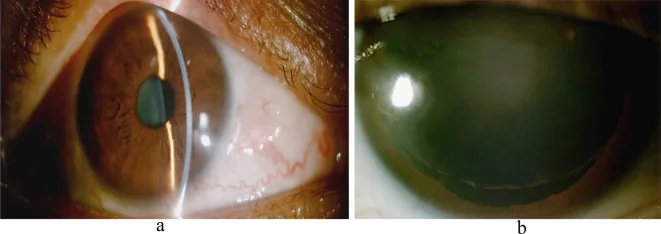
Left anterior segment photograph. Panel a shows an area of iridodialysis inferiorly, and panel b shows that after mydriasis, the zonules are severed from 1 to 10 o’clock and the lens is partially dislocated. This corresponds to iridodonesis and the hallmark of phacodonesis (exposure of the lens edge under mydriasis) discussed in the section “2. Main symptoms and clinical findings.”
If the degree of displacement is mild, only refractive error occurs, but as it progresses, monocular diplopia and high hyperopia due to the absence of the lens develop.
Visual impairment/refractive error: Displacement of the lens causes irregular astigmatism, myopia, or hyperopia.
Monocular diplopia: Caused by tilting of the lens. It is characterized by diplopia remaining even in one eye on the cover test.
High hyperopia: When subluxation progresses and the lens functionally disappears, marked hyperopia occurs.
Acute eye pain and increased intraocular pressure: This occurs when aqueous humor circulation is impaired due to lens prolapse into the anterior chamber or vitreous incarceration.
When the zonules of Zinn are weak, lens tremors (phacodonesis) may be observed during eye movements. Additionally, unstable lens can cause iridodonesis and abnormal iris shape due to lens displacement. If the anterior chamber depth differs between the two eyes, weakness of the zonules of Zinn on the shallower side should be suspected.
If prolapsed vitreous becomes incarcerated and the lens dislocates into the anterior chamber, aqueous humor circulation may be impaired, leading to a rapid increase in intraocular pressure and pain.
Iridodonesis: Trembling of the iris during eye movements due to loss of lens support
Asymmetry of anterior chamber depth: Shallower side indicates weakness of the zonules of Zinn
Vitreous prolapse: Incarceration of vitreous fibers into the anterior chamber
QWhat happens if the lens comes into the anterior chamber?
A
Lens prolapse into the anterior chamber impairs aqueous humor circulation, causing a rapid increase in intraocular pressure and severe pain. If the lens contacts the corneal endothelium, the risk of corneal endothelial damage also increases. Prompt lens removal is necessary; delayed treatment may lead to irreversible visual impairment.
Blunt trauma from balls in sports such as baseball, soccer, and tennis, or from blows in fights, can cause lens subluxation. This occurs because the external force deforms the eyeball, and it is often accompanied by iris dialysis.
When the history of trauma is unclear or when the condition is bilateral, it is important to differentiate from lens dislocation associated with systemic diseases.
Elderly; exfoliative material on corneal endothelium
In traumatic cases, in addition to confirming the history of injury, associated findings of traumatic changes such as iridodialysis, hyphema, and angle recession are helpful for differentiation.
QWhat is the difference between traumatic lens dislocation and Marfan syndrome?
A
Traumatic cases have a clear history of injury and are often accompanied by traumatic findings such as iridodialysis, hyphema, and angle recession. Marfan syndrome is bilateral, often with upward displacement, and is associated with systemic findings such as tall stature, arachnodactyly, and heart valve disease (especially aortic regurgitation). Even if diagnosed after trauma, if bilateral, family history, or skeletal abnormalities are present, evaluation for Marfan syndrome should be performed.
Slit-lamp microscopy under mydriasis is the basic examination. The location and extent of zonular rupture are identified using retroillumination, which aids in surgical planning.
Examination
Purpose
Slit-lamp examination under mydriasis
Confirmation of lens displacement, tilt, phacodonesis, and iridodonesis
Retroillumination
Identification of zonular rupture site and remaining area
As long as correction with glasses or contact lenses is possible, observation is performed. If there is a difference in visual acuity between eyes, amblyopia treatment such as patching of the better eye is performed.
The CTR supports the area of zonular dialysis and maintains the capsular bag in a circular shape, thereby equalizing tension on the remaining zonules. In cases of extensive zonular dialysis, scleral fixation using a modified CTR with scleral hooks (e.g., Cionni ring) is selected. 4)
In vitrectomy for complete dislocation, liquid perfluorocarbon (LPFC) is first injected into the vitreous cavity to float the lens anteriorly, and then the lens is removed via a transscleral or transcorneal approach. 2)
QIs surgery necessary if the lens is only slightly displaced?
A
For mild subluxation where visual acuity can be corrected with glasses or contact lenses, observation is possible. However, subluxation may gradually progress. If irregular astigmatism, monocular diplopia, or high hyperopia occurs, or if zonular dialysis becomes extensive, surgical indications should be considered. Regular slit-lamp examination to assess the extent of dialysis is important.
QCan the intraocular lens (IOL) dislocate after surgery?
A
Because zonular weakness persists, postoperative IOL decentration or dislocation can occur. Although stability has improved with CTR or intrascleral fixation (e.g., Yamane technique), reports indicate that even scleral-fixated IOLs may develop tilt or decentration over the long term. 1) Long-term follow-up with regular anterior segment OCT and slit-lamp examination is necessary.
The zonules of Zinn (ciliary zonules) are fiber bundles that run from the non-pigmented epithelium of the ciliary body to the equator of the lens. They hold the lens on the visual axis and transmit relaxation and contraction of the ciliary muscle to the lens, enabling accommodation.
When blunt force is applied to the eye, the globe temporarily deforms. This sudden deformation places excessive tension on the zonules, causing them to rupture.
Partial rupture: Lens concussion or subluxation. The remaining zonules hold the lens, so it remains within the eye.
Complete circumferential rupture: Complete dislocation. Gravity causes the lens to fall into the vitreous cavity or dislocate into the anterior chamber.
Mechanism of anterior chamber prolapse: Prolapse into the anterior chamber occurs with forward movement of the vitreous. The dislocated lens, iris, and vitreous block the flow of aqueous humor, leading to a rapid increase in intraocular pressure.
During trauma, the impact of ocular deformation is transmitted to the ciliary body and angle. Shearing forces at the angle (attachment of the ciliary ring muscle) cause the iris root to tear. This is iridodialysis, a finding frequently associated with traumatic lens subluxation.
Anterior lens dislocation type: Pupillary block prevents aqueous humor from flowing into the anterior chamber, resulting in a condition similar to acute angle-closure glaucoma.
Vitreous incarceration type: Vitreous prolapsed into the anterior chamber blocks the trabecular meshwork, impairing aqueous humor outflow.
The Yamane technique is a sutureless method that uses a double-needle technique to fixate IOL haptics to the sclera, and is less invasive than conventional suturing methods. 1) Its application is advancing in cases with extensive zonular damage, and reports of postoperative IOL stability are accumulating.
Standard CTR is used to maintain the capsular bag in a circular shape in cases with localized zonular weakness. When the defect is extensive, consider scleral suturing with a modified CTR (Cionni ring) that has scleral hooks 4,6). Outcomes after CTR use depend on case selection and whether the posterior capsule is preserved, so individualized judgment based on intraoperative findings is necessary.
In a study of traumatic lens dislocation and subluxation surgery by Hapca et al. (2023), postoperative visual acuity improved in many cases, while poor preoperative visual acuity, retinal detachment, and iridodonesis were associated with poor prognosis 3). Bhatt et al. (2019) also examined visual outcomes of traumatic lens dislocation, emphasizing the importance of assessing concomitant injuries and preoperative visual function for prognosis 5).
Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K.. Flanged Intrascleral Intraocular Lens Fixation with Double-Needle Technique. Ophthalmology. 2017;124(8):1136-1142. doi:10.1016/j.ophtha.2017.03.036. PMID:28457613.
Richard S. Hoffman, Michael E. Snyder, Uday Devgan, Quentin B. Allen, Ronald Yeoh, Rosa Braga-Mele. Management of the subluxated crystalline lens. Journal of Cataract and Refractive Surgery. 2013;39(12):1904-1915. doi:10.1016/j.jcrs.2013.09.005.
Hapca M, Muntean G, Nemeș-Drăgan I, Vesa Ș, Nicoară S.. Visual Outcomes of Traumatic Lens Dislocations and Subluxations Managed by Pars Plana Vitrectomy and Lensectomy. J Clin Med. 2023;12(22). PMCID:PMC10671993.
Chee SP, Jap A. Management of severely subluxated cataracts using a modified capsule tension ring approach. Am J Ophthalmol. 2007;143(3):409-416.
Bhatt P, Bhatt C, Modi R, Lad M. Traumatic lens dislocation: Clinical features and visual outcome. Indian J Ophthalmol. 2019;67(10):1645-1649.
Cionni RJ, Osher RH.. Management of profound zonular dialysis or weakness with a new endocapsular ring designed for scleral fixation. J Cataract Refract Surg. 1998;24(10):1299-1306. doi:10.1016/s0886-3350(98)80218-6. PMID:9795841.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.