Traumatic glaucoma is secondary glaucoma caused by ocular trauma. It can occur from blunt (non-penetrating) trauma, penetrating trauma, chemical trauma, or radiation trauma. Both open-angle and closed-angle mechanisms are involved 2). Particularly after blunt trauma, intraocular pressure elevation occurs through various mechanisms such as hyphema, angle recession, ghost cell glaucoma, and pupillary block due to lens dislocation.
In the acute phase, aqueous humor production is often affected, so intraocular pressure may not necessarily rise even if the outflow pathway is damaged. Additionally, multiple factors such as hyphema, inflammation, and lens damage are simultaneously involved in the acute phase of intraocular pressure elevation. Furthermore, it can develop late, from several years to over a decade after injury, making long-term follow-up essential 2)3).
The concept of angle recession was first reported by Collins in 1892. In 1949, D’Ombrain pointed out the association between trauma and unilateral glaucoma, and in 1962, Wolf and Zimmer first systematically demonstrated the chain of trauma, angle recession, and glaucoma onset in six cases. Subsequent research established angle recessionglaucoma as a representative type of secondary open-angle glaucoma.
In Girkin et al.’s analysis of the US Eye Injury Registry, the incidence of traumatic glaucoma 6 months after blunt trauma was approximately 3.4%6).
In a 10-year prospective study of 31 eyes by Kaufman and Tolpin, approximately 6% of angle recession cases progressed to glaucoma in the long term 7).
With extensive angle recession of 180 degrees or more, glaucoma develops in 6–20% of cases within 10 years.
Onset ranges from a few days to several years, with reports of onset up to 50 years later.
Approximately 50% of ARG patients develop open-angle glaucoma in the contralateral eye, suggesting a constitutional predisposition5).
Common causes of injury include sports (ball trauma, punches, rackets, etc.), martial arts, assault, traffic accidents, and occupational injuries. In children, domestic impacts and abuse should also be considered in the differential diagnosis. In infants and children, if hyphema persists for more than two weeks, there is a risk of deprivation amblyopia, requiring earlier active intervention than in adults. Closed-globe injury from blunt trauma is recognized as a series of conditions including hyphema, iridodialysis, angle recession, lens dislocation, commotio retinae, and contusion of the fundus.
Many studies report a male predominance, reflecting the mechanisms of injury (sports and assault are more common in males). Age distribution is more common in young to middle-aged individuals, but due to late onset, there is often a significant gap between the age at injury and the age at onset.
QHow long after an eye contusion does glaucoma develop?
A
It often develops immediately to several years after injury, but there are reports of onset up to 50 years later. The incidence of traumatic glaucoma 6 months after blunt trauma is approximately 3.4%6), and about 6% of eyes with angle recession progress to glaucoma in the long term7). Especially with extensive angle recession of 180 degrees or more, 6–20% develop glaucoma within 10 years. If there is a history of ocular trauma, regular follow-up of intraocular pressure, angle, and optic disc is important even without symptoms.
In the acute phase of elevated intraocular pressure, patients experience blurred vision due to corneal edema, eye pain, and nausea. Hyphema may cause decreased vision and photophobia. Rapid elevation of intraocular pressure can cause headache and vomiting, which may be mistaken for acute angle-closure glaucoma attack. Chronic elevated intraocular pressure progresses asymptomatically and is often discovered after visual field defects have advanced.
Hyphema: The most common complication of blunt trauma. In mild cases, only a small amount of blood is seen in the anterior chamber under slit-lamp microscopy; in moderate cases, a horizontal level (niveau) is present. In severe cases, the anterior chamber is filled with blood clots, changing from bright red to dark red or black. When the anterior chamber is completely filled with dark brown blood, it is called an 8-ball hyphema (black ball hyphema), and if persistent, early surgical intervention is necessary.
The severity of hyphema is generally classified as Grade I (less than 1/3 of the anterior chamber), Grade II (1/3 to 1/2), Grade III (more than 1/2), and Grade IV (total, 8-ball). Higher grades are associated with increased frequency of secondary hemorrhage, elevated intraocular pressure, and corneal blood staining. The height of the hyphema is recorded daily to objectively assess changes in bleeding volume. On inspection, fresh bleeding appears bright red, changes to dark red and blackish-brown over time, and is eventually observed as a yellowish-orange fibrin clot.
Angle recession: Observed on gonioscopy as widening of the ciliary body band. The distance from the iris root to the scleral spur increases, and the ciliary body appears as a broad, dark gray band. It results from a tear between the longitudinal and circular muscles of the ciliary body.
Corneal blood staining: When severe hyphema is accompanied by persistent elevated intraocular pressure, the posterior cornea becomes stained with blood. Since it can cause lasting visual impairment even after the hemorrhage resolves, early anterior chamber washout is necessary.
Ghost cells: One to four weeks after vitreous hemorrhage, degenerated red blood cells appear in the anterior chamber as khaki-colored vesicles. In large numbers, they can form a pseudohypopyon.
Cyclodialysis: A condition in which the ciliary body detaches from the sclera. Aqueous humor flows into the suprachoroidal space, leading to persistent hypotony. Prolonged hypotony can cause hypotony maculopathy.
Iridodialysis: Detachment of the iris root from the scleral spur. On slit-lamp examination, it appears as a crescent- or half-moon-shaped gap. If the tear is extensive and causes pupillary deviation, it can lead to decreased vision or monocular diplopia. It is often accompanied by vitreous prolapse due to zonular rupture.
Traumatic mydriasis: The pupil dilates due to rupture of the pupillary sphincter from blunt force. Both the light reflex and near reflex are diminished or absent. There is no response or a diminished response to 1% pilocarpine hydrochloride eye drops. Slit-lamp examination reveals notched irregularities at the pupillary margin. Differentiation from oculomotor nerve palsy due to head trauma is important; check for ptosis and ocular motility disorders.
Lens abnormalities: May include subluxation recognized as phacodonesis, complete dislocation, or traumatic cataract. Lens dislocation can cause pupillary block or phacolytic glaucoma.
Biphasic intraocular pressure: Immediately after injury, intraocular pressure may be mildly decreased due to reduced aqueous production by the ciliary body. Subsequently, blood components from disrupted ciliary vessels obstruct the trabecular meshwork due to angle recession, causing a sharp rise in intraocular pressure. A characteristic feature of this condition is that intraocular pressure can be low, normal, or high during the post-injury course.
The basic diagnosis is made by gonioscopy, which reveals widening of the ciliary band. The distance from the iris root to the scleral spur increases, and the ciliary band is observed as a broad, dark gray band. Since some eyes have a physiologically wide ciliary band, comparison with the contralateral healthy eye is essential. Ultrasound biomicroscopy (UBM) and anterior segment OCT are also used as adjuncts. However, gonioscopy should be avoided until the hyphema resolves, as there is a risk of rebleeding while blood remains in the anterior chamber.
In chemical injuries caused by alkalis or strong acids, inflammation-induced pupillary block, peripheral anterior synechiae, and inflammation/scarring of the trabecular meshwork itself can lead to elevated intraocular pressure. Alkali injuries in particular have high penetrance into the deep eye, often causing severe anterior segment damage and secondary glaucoma. Radiation injuries can cause neovascular glaucoma due to retinal ischemia.
Factors that increase the risk of progression from angle recession after blunt trauma to glaucoma include:
Extent of recession: 180 degrees or more (some authors suggest 240 degrees or more)
Increased pigment deposition in the angle
Elevated baseline intraocular pressure
Lens dislocation
Glaucoma findings in the contralateral eye: Approximately 50% of patients with angle recessionglaucoma also develop open-angle glaucoma in the fellow eye, suggesting that trauma may accelerate the process in eyes predisposed to glaucoma5)
QDoes angle recession always lead to glaucoma?
A
Not all cases of angle recession develop glaucoma. It is reported that approximately 6% of angle recession cases progress to glaucoma7). However, extensive recession of 180 degrees or more, increased pigmentation, and elevated baseline intraocular pressure increase the risk. Since it may develop late, several to more than ten years after injury, long-term intraocular pressure monitoring is essential 2)3).
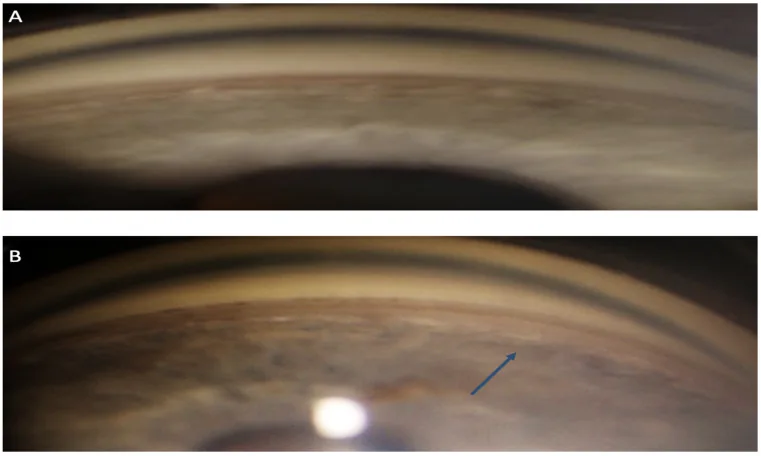
Life (Basel). 2023 Aug 27;13(9):1814. Figure 2. PMCID: PMC10532958. License: CC BY.
Gonioscopic photographs showing the superior and inferior angles side by side. The abnormal widening of the inferior angle is indicated by an arrow, allowing specific understanding of the diagnostic findings of angle recession.
History taking includes the mechanism of injury (direction, force, time of injury), past medical history, medication history (use of anticoagulants), and systemic diseases (family history of sickle cell disease, bleeding diathesis).
Basic examinations include visual acuity testing, pupillary light reflex testing, intraocular pressure measurement using non-contact or applanation tonometry, and slit-lamp microscopy. Assess the amount of hyphema, lens dislocation, iris dialysis, and the degree of inflammatory cells and flare in the anterior chamber. If hyphema is massive, also check the consensual light reflex of the fellow eye. Perform Seidel test (observation of corneal wound leakage under fluorescein) to rule out corneal perforation.
Gonioscopy is the gold standard for diagnosing angle recession. Confirm widening of the ciliary body band and increased distance from the iris root to the scleral spur. Comparison with the fellow eye (uninjured eye) is essential 4). Since the ciliary body band can be wide even in normal eyes, pathological widening can only be confirmed by side-by-side observation with the healthy eye.
In routine practice, indirect gonioscopy (Goldmann gonioscope, Zeiss four-mirror lens) is used. The Shaffer-Kanski classification, Scheie classification, and Spaeth classification are used to evaluate the angle opening. In the Shaffer-Kanski classification, the angle opening is graded from 0 to 4, with grade 4 (35–45 degrees) indicating maximum opening with no possibility of angle closure, and grade 0 (not visible) indicating closure. Direct gonioscopy (Koeppe, Swan-Jacob, etc.) is used during surgery or for examining infants.
In gonioscopy, in addition to the degree of angle opening and pigmentation, findings such as peripheral anterior synechia (PAS), Sampaolesi line, angle neovascularization, residual silicone oil, angle nodules, hyphema, angle recession, angle dysgenesis, and angle changes after glaucoma surgery are also recorded in detail. In traumatic eyes, increased pigmentation of the angle is often observed, which is considered one of the risk factors for glaucoma.
While hyphema persists, gonioscopy should be avoided for 1–2 weeks after injury due to the risk of rebleeding. Detailed angle evaluation should be performed after the hemorrhage has resolved.
UBM can visualize fine structures from the iris root to the ciliary body, making it useful for evaluating cyclodialysis and angle recession. Anterior segment OCT is non-contact, non-invasive, and has excellent resolution, but visualization of the ciliary body is difficult.
The 5th edition of the Glaucoma Practice Guidelines lists trauma, uveitis, lens material, intraocular foreign bodies, etc. as causes of secondary open-angle glaucoma where the main resistance to aqueous outflow is in the trabecular meshwork4). The guidelines state that gonioscopy reveals “traumatic changes such as cyclodialysis or widening of the ciliary band (angle recession)”, emphasizing the importance of gonioscopy4).
Diagnosis of this condition requires identification of the mechanism of intraocular pressure elevation and the underlying cause, and treatment of the cause is the first step in the treatment strategy. Since multiple mechanisms often coexist, it is necessary to comprehensively evaluate traumatic changes throughout the eye, including hyphema, iritis, lens abnormalities, retinal contusion, and choroidal rupture.
For patients with a history of blunt ocular trauma, it is recommended to continue intraocular pressure measurement, gonioscopy, optic disc evaluation, and visual field testing at least once a year after injury. Particularly in cases with angle recession of 180 degrees or more, lifelong follow-up is desirable. Attention should also be paid to intraocular pressure and optic nerve changes in the contralateral eye.
Measurement of retinal nerve fiber layer (RNFL) thickness and peripapillary ganglion cell complex (GCC) thickness using optical coherence tomography (OCT) is useful for long-term follow-up, as it can detect glaucomatous optic neuropathy before early visual field abnormalities appear. Standard visual field testing is Humphrey 24-2 or 30-2 SITA Standard, performed 1-2 times per year. Since a single intraocular pressure measurement at the time of examination does not reflect diurnal variation, diurnal variation measurement should be performed in cases with abnormal values or suspected progression.
Traumatic hyphema is managed primarily with rest and medication. The patient should rest in a sitting position or with the head of the bed elevated 30-45 degrees. Strenuous exercise is prohibited, and hospitalization is desirable for children or cases where the hyphema level exceeds one-third to one-half of the anterior chamber.
Acute-phase pharmacotherapy is based on the following regimen.
Mydriatics: Atropine ophthalmic solution (1%) once daily at bedtime (for anti-inflammatory effect and to reduce stress on the angle)
Steroid eye drops: Betamethasone (0.1% Rinderon) 4 times daily
Hemostatic agents: Carbazochrome (Adona tablets 30 mg) 3 tablets divided into 3 doses after each meal
Intraocular pressure-lowering drugs (when IOP is elevated):
Hyperosmotic agents: Mannitol infusion for acute intraocular pressure elevation
Pilocarpine hydrochloride is absolutely contraindicated. It not only exacerbates inflammation but also widens the angle, increasing bleeding and rebleeding, and may induce malignant glaucoma. Prostaglandin analogs should also be avoided in the acute phase as they may enhance acute inflammation.
The purpose of using mydriatics (atropine) is to reduce pain by paralyzing the ciliary muscle, reduce mechanical stress on the angle, and prevent posterior synechiae. Atropine is the first choice over other strong mydriatics to avoid narrowing of the peripheral angle due to excessive dilation.
Topical corticosteroids (e.g., betamethasone) help calm iritis, suppress inflammation of the trabecular meshwork, and prevent rebleeding. However, in steroid responders, intraocular pressure may rise, so frequent pressure checks are needed after initiation. If pressure elevation occurs, consider switching to a weaker steroid such as loteprednol or fluorometholone.
Guidelines for Tolerable Intraocular Pressure Duration
In healthy young patients, an intraocular pressure of 50 mmHg is tolerable for 5 days, and 35 mmHg for 7 days without significant risk to the optic nerve. If glaucomatous optic neuropathy is already present, if hyphema is severe, or if there is a risk of corneal blood staining, perform anterior chamber washout promptly without waiting for the above durations.
Indications and Timing for Anterior Chamber Washout
The optimal timing for anterior chamber washout is around day 4 after injury, when the risk of rebleeding is lower and the clot has partially separated from ocular tissues. The procedure involves using an anterior chamber irrigation needle (Simcoe needle) through a corneal side port. If the clot is large and firm, it can be removed with forceps or cut and aspirated with a vitreous cutter.
Rebleeding tends to occur 3–7 days after injury, with a reported incidence of 5–10%2). Rebleeding is often more severe than the initial bleeding and increases the risk of complications. Although antifibrinolytic agents (e.g., tranexamic acid) have been reported to be effective in preventing rebleeding, their impact on visual prognosis is unclear2).
Elevated intraocular pressure after the resolution of post-traumatic inflammation involves trabecular meshwork scarring and peripheral anterior synechiae. Surgery is indicated when pressure is poorly controlled with multiple medications3).
Medication Therapy
Aqueous suppressants: Beta-blockers, carbonic anhydrase inhibitors, and alpha-2 agonists are effective.
Prostaglandin analogs: Can be used after acute inflammation subsides. They increase uveoscleral outflow and bypass the dysfunctional trabecular meshwork2).
Contraindications: Pilocarpine (miotic) is contraindicated as it worsens angle recession.
Laser Therapy
Argon laser trabeculoplasty (ALT): Some reports indicate failure in long-term intraocular pressure reduction.
Selective laser trabeculoplasty (SLT): Analysis of 560 patients from the IRIS registry showed a failure rate of 48% at 18 months, higher than the general rate (41%)5).
Surgical Therapy
Trabeculectomy (with MMC): Successful in lowering intraocular pressure in some cases, but with a high risk of bleb failure.
Glaucoma drainage devices: Ahmed valve and Baerveldt implant are options1)3).
Due to conjunctival adhesion and scarring from trauma or repeated surgeries, filtering surgery is often difficult. Tube shunt surgery, such as Ahmed glaucoma valve or Baerveldt glaucoma implant, may be the first choice in some cases3). In refractory cases, cyclodestructive procedures (transscleral cyclophotocoagulation, endoscopic cyclophotocoagulation) are also options.
In ghost cell glaucoma, it is desirable to remove ghost cells by anterior chamber irrigation and vitrectomy in addition to intraocular pressure-lowering medications 2). If lens dislocation or damage is present, lens extraction is necessary. If there is pupillary block, laser iridotomy or lens extraction should be performed concurrently.
In traumatic eyes, scarring of the conjunctiva and Tenon’s capsule and anatomical changes in the anterior segment are often present, making surgery more difficult than general glaucoma surgery. Preoperative assessment of conjunctival mobility, evaluation of iris, lens, and ciliary body structure, and understanding of existing wounds and intraocular lens fixation status are important in the planning stage. Flexible selection of surgical techniques according to intraoperative findings and ensuring long-term postoperative management affect the prognosis.
For persistent hypotony due to cyclodialysis cleft, conservative medical therapy is first performed.
Atropine ophthalmic solution (1%) once daily at bedtime
Fluorometholone ophthalmic solution (0.1% Flumetholon) 4 times daily
If medical therapy does not improve the condition, surgical treatment is considered. Options include argon laser photocoagulation of the cleft, cyclodiathermy, transscleral cryocoagulation, scleral buckling, direct suturing of the cyclodialysis cleft, and anterior vitrectomy. If hypotony maculopathy persists, prompt surgical intervention improves visual prognosis.
Small (1-2 clock hour) cyclodialysis clefts may resolve spontaneously or with medical therapy, but extensive clefts are difficult to heal with passive observation alone. Recently, minimally invasive techniques such as anterior vitrectomy combined with gas tamponade, direct closure by suturing, and endoscopic laser photocoagulation from inside have been reported. The choice of treatment is determined considering the extent of the cleft, intraocular status, and corneal clarity.
QWhen is rebleeding of hyphema likely to occur?
A
Rebleeding is most likely to occur 3 to 7 days after injury, with an incidence reported at 5-10% 2). This coincides with the time when the initial clot begins to retract and dissolve. Rebleeding is often more severe than the initial bleeding and increases the risk of complications. Maintaining rest, administering mydriatics, and considering discontinuation of anticoagulants are important. In children or when hyphema occupies more than 1/3 to 1/2 of the anterior chamber, hospitalization is recommended.
6. Pathophysiology and Detailed Mechanism of Onset
During blunt trauma, the eyeball wall deforms, exerting stretching forces or forces that peel the iris and ciliary body inward. Microtissue damage disrupts the blood-aqueous barrier, causing inflammatory cells to migrate into the anterior chamber. Damage to the pupillary sphincter results in traumatic mydriasis.
The most vulnerable area is the thin part where the iris attaches to the ciliary body. A tear here causes iridodialysis, displacing the pupil. A fissure slightly more scleral within the ciliary body leads to angle recession, and further scleral detachment of the ciliary body from the sclera results in cyclodialysis. These lesions are particularly prone to hyphema.
When blunt force causes a rapid rise in anterior chamber pressure, the limbus stretches and aqueous humor moves posteriorly and into the angle. This exerts traction on the iris root, causing a tear between the longitudinal (Brücke) and circular (Müller) muscles of the ciliary body. Angle recession is a condition where the ciliary body moves posteriorly with the iris, also called angle cleavage.
If the force is sufficiently large, the ciliary artery ruptures, causing hyphema. The high incidence of angle recession (60–100%) in traumatic hyphema is due to this common mechanism. That is, angle recession and hyphema are not independent lesions but are understood as continuous tissue damage from the same force. Rupture of an artery within the ciliary body causes rapid bleeding into the anterior chamber, and a short-term rise in intraocular pressure can cause secondary damage to the contralateral corneal endothelium.
Histologically, the injury site shows the following features. The circular muscle (Müller) of the ciliary body is located medially (lens side), and the longitudinal muscle (Brücke) is located laterally (scleral side). Between the two muscles lies a connective tissue layer, which is mechanically the weakest point. Blunt force causes anteroposterior shortening of the eyeball and subsequent equatorial expansion, applying strong shear forces to the ciliary body, resulting in a fissure in this connective tissue layer.
Chronic increase in aqueous outflow resistance due to scarring and fibrosis of the trabecular meshwork and Schlemm’s canal
Narrowing of Schlemm’s canal due to loss of ciliary muscle tension on the scleral spur
Proliferation of a glassy membrane covering the trabecular meshwork
Secondary angle closure due to peripheral anterior synechiae
The EGS Guidelines list trabecular meshwork damage, scarring, inflammation, obstruction by red blood cells and debris, angle recession, and lens-induced glaucoma as secondary open-angle glaucomas due to blunt trauma 2). It is emphasized that intraocular pressure elevation can occur after a very long period following trauma 2). Histologically, discontinuous glassy membrane-like material is observed proliferating in the trabecular meshwork of angle recession cases, and this structure is thought to increase aqueous humor outflow resistance over the long term.
Scarring of the trabecular meshwork progresses gradually after injury, and aqueous humor outflow function, which was normal immediately after injury, declines over several years to decades. Therefore, even if intraocular pressure is normal immediately after injury, future development of glaucoma cannot be ruled out. Regular measurement of intraocular pressure and evaluation of the optic nerve and visual field are essential for long-term management.
After vitreous hemorrhage, if red blood cells remain in the vitreous for several weeks, most of the cellular contents are absorbed, leaving hollow cell bodies (ghost cells) containing only denatured hemoglobin (Heinz bodies). Ghost cells have reduced deformability compared to normal red blood cells and cannot pass through the trabecular meshwork, causing obstruction 2). Ghost cells move into the anterior chamber when the anterior vitreous face is disrupted and there is communication between the vitreous and anterior chamber. Due to the high oxygen tension and rapid circulation in the anterior chamber, ghost cells are less likely to form from anterior chamber hemorrhage alone 2).
When the lens capsule is damaged by trauma, leakage of lens material can deposit in the trabecular meshwork and increase intraocular pressure (phacolytic glaucoma). The main mechanism is trabecular meshwork obstruction by macrophages that have phagocytosed lens cortex. A type III allergic reaction to lens proteins (phacoanaphylactic glaucoma) can also occur.
Epithelial downgrowth occurs when epithelial cells that enter the anterior chamber through a penetrating wound cover the trabecular meshwork, corneal endothelium, and anterior iris surface, obstructing aqueous humor outflow. Treatment is extremely difficult, and resection of affected tissue with cryotherapy may be chosen, but the prognosis is poor.
Fibrous downgrowth is a condition in which fibroblasts proliferate into the anterior chamber through a penetrating wound. Its progression is slower than epithelial downgrowth, but it is similarly refractory to treatment.
Siderosis bulbi is a full-thickness condition in which iron ions eluted from iron-containing intraocular foreign bodies exert toxicity on cells such as trabecular meshwork cells, lens epithelium, and retinal pigment epithelium. In particular, deposition in the trabecular meshwork causes chronic impairment of aqueous humor outflow. Electroretinography (ERG) shows early reduction of b-wave amplitude, serving as an indicator of full-thickness damage. Early removal of the intraocular foreign body is important for prevention.
In cyclodialysis, an aqueous humor drainage pathway from the ciliary body to the suprachoroidal space (a collateral route of the uveoscleral outflow pathway) is formed, leading to persistent hypotony. Prolonged hypotony induces retinochoroidal folds and macular edema, resulting in visual impairment as hypotony maculopathy. Closure of the dialysis requires surgical treatments such as ciliary body suturing, diathermy coagulation, or vitrectomy.
The pathogenesis of hypotony maculopathy involves deformation of the ocular wall due to low intraocular pressure, leading to subretinal fluid shift, choroidal folds, and optic disc edema, which impair photoreceptor function in the macula. If intraocular pressure remains below 6 mmHg for several weeks, irreversible visual loss may occur, making early diagnosis and treatment crucial. The goal of treatment is to restore intraocular pressure to 10 mmHg or higher and halt the progression of anatomical changes.
Traumatic glaucoma involves multiple mechanisms, requiring identification of the cause of intraocular pressure elevation and treatment strategies tailored to each case2). Recently, a technique for inserting the tube of the Ahmed glaucoma valve (AGV) into the ciliary sulcus has been reported to have the advantage of less corneal endothelial cell loss compared to anterior chamber insertion1). However, with conventional simple insertion, according to Asaoka et al., 46% of attempts were unsuccessful on the first try, and in 4.4% of cases, ciliary sulcus insertion itself was impossible1).
Nitta et al. (2023) reported a 4-0 nylon guide method using a reliable guide channel created with a 23G needle1). Compared to the 21G/23G needle guide method, this technique has a lower risk of iris interference due to horizontal insertion and eliminates the risk of misdirection into the vitreous cavity. It enables accurate ciliary sulcus insertion even in eyes with poor dilation or intraocular lens instability1).
Case report (Nitta et al. 2023)1): This procedure was performed on an 88-year-old female with angle recessionglaucoma. She had pseudoexfoliation syndrome with poor pupillary dilation (maximum pupil diameter 3.5 mm) and mild IOL instability. Preoperative IOP was 40 mmHg, but at 1 month postoperatively, IOP was 10 mmHg (without eye drops), and no decrease in corneal endothelial cell density was observed.
Nitta K, Akiyama H. A New Technique Using a 4-0 Nylon Thread as a Guide for Easy and Precise Tube Insertion of Ahmed Glaucoma Valve Implant Into Ciliary Sulcus. Cureus. 2023;15(2):e34854. doi:10.7759/cureus.34854.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Girkin CA, McGwin G Jr, Long C, Morris R, Kuhn F. Glaucoma after ocular contusion: a cohort study of the United States Eye Injury Registry. Journal of glaucoma. 2005;14(6):470-3. doi:10.1097/01.ijg.0000185437.92803.d7. PMID:16276279.
Kaufman JH, Tolpin DW. Glaucoma after traumatic angle recession. A ten-year prospective study. Am J Ophthalmol. 1974;78(4):648-654.
Wiggins RE Jr, Vaphiades M, Crouch ER Jr. Sickle cell trait and secondary glaucoma following ocular trauma. J Ocul Pharmacol Ther. 1995;11(2):201-205.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.