Drug-induced acute angle-closure glaucoma (drug-induced AACG) is an ophthalmic emergency in which acute angle closure is triggered by the use of topical or systemic medications 1). Delayed appropriate treatment can lead to permanent vision loss due to irreversible optic nerve damage.
Patients predisposed to acute angle closure have anatomical features such as hyperopia, short axial length, shallow anterior chamber, and narrow angle 1). The prevalence of narrow angles is reported to be approximately 3.8% in Caucasians and 8.5% in Asians 1). Other risk factors include older age, female sex, family history, and a history of AACG in the fellow eye 1).
The mechanisms of drug-induced AACG are broadly divided into pupillary block type and non-pupillary block type1). Pupillary block is the most common mechanism, but it is important to exclude secondary causes (e.g., plateau iris, lens-induced, retrolental) 3).
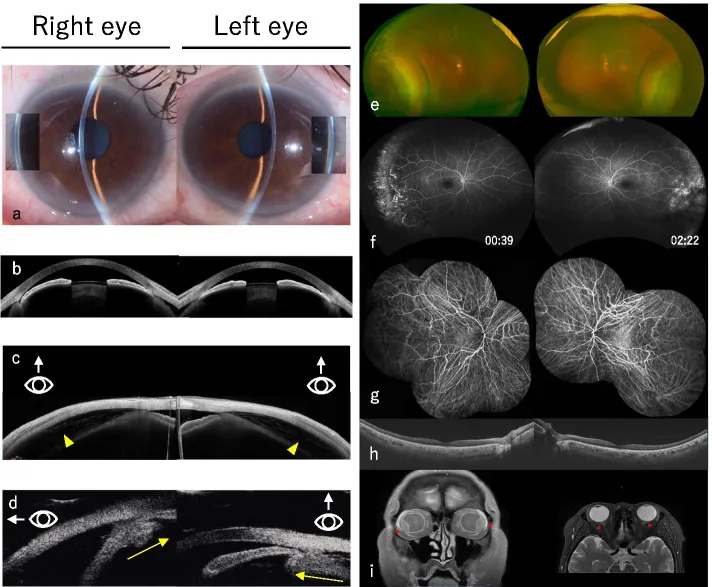
Takahashi S, et al. Multimodal imaging of indapamide-induced bilateral choroidal effusion: a case report. BMC Ophthalmol. 2021. Figure 1. PMCID: PMC8567550. License: CC BY.
a shows narrowing of the angle, b shows an extremely shallow anterior chamber, c shows choroidal detachment (yellow arrowhead), d shows anterior displacement of the lens and ciliary body edema (yellow arrow), and e shows a fundus image of choroidal detachment. This corresponds to the choroidal detachment discussed in the section “2. Main symptoms and clinical findings”.
Symptoms of an acute attack include sudden unilateral severe eye pain, redness, headache, nausea/vomiting, blurred vision, and halos around lights (rainbow vision) 2). Systemic symptoms such as severe headache, nausea, and vomiting may be prominent, sometimes leading to misdiagnosis as neurological or gastrointestinal diseases 2). Intraocular pressure may rise to 40–80 mmHg.
Gonioscopy reveals extensive iridotrabecular contact (ITC) 3). The contralateral eye typically also shows risk findings for angle closure on gonioscopy3). When corneal edema makes gonioscopy difficult, AS-OCT or ultrasound biomicroscopy is useful 2).
In a case of olanzapine-induced AAC, one week after starting the medication, the right eye showed IOP of 51 mmHg, microcystic corneal edema, moderate fixed mydriasis, and shallow anterior chamber with iris bombé 1). Ultrasound biomicroscopy confirmed 360-degree angle closure, and no choroidal effusion was observed 1).
Topiramate: Causes shallow anterior chamber due to ciliary body effusion, anterior rotation of the ciliary body, and lens swelling. Onset occurs within 2 weeks of starting treatment, and almost all cases are bilateral 2, 3)
Sulfonamides: Secondary shallowing of the anterior chamber due to lens swelling, retinal edema, and choroidal effusion
SSRIs (some): Escitalopram and venlafaxine have been reported to cause bilateral angle closure with uveal effusion 2)
Anticoagulants: Forward movement of the iris-lens diaphragm due to spontaneous choroidal hemorrhage
Drugs with mydriatic or cycloplegic effects can induce APACA in eyes with anatomical predispositions such as shallow anterior chamber and thick lens 2). This is because mydriasis enhances pupillary block and angle crowding 2). Specific drugs include SSRI antidepressants, tricyclic antidepressants, nasal decongestants (containing antihistamines), anticholinergics, sympathomimetics, and antiemetics 2).
Nebulized bronchodilators (ipratropium bromide, salbutamol) can also induce acute angle closure 3). Acute angle closure may also occur during or after general anesthesia 3).
QWhich drugs cause acute angle closure?
A
They are broadly divided into two mechanisms. In the pupillary block type, drugs with mydriatic effects (sympathomimetics, anticholinergics, tricyclic antidepressants, SSRIs, antipsychotics, benzodiazepines, bronchodilators) are causative. In the non-pupillary block type, topiramate and sulfonamides cause ciliary body edema and choroidal effusion, pushing the iris-lens diaphragm forward and inducing angle closure. In both cases, risk is higher in patients with anatomical predispositions (shallow anterior chamber, narrow angle, hyperopia).
Diagnosis of drug-induced AACG requires evaluation of clinical findings and a detailed medication history. Since a high proportion of acute angle closure is induced by topical or systemic drugs, a complete medication history including prescription and non-prescription drugs should be obtained 3).
Gonioscopy should be performed in both eyes2). Even if corneal edema makes gonioscopy of the affected eye difficult, findings in the fellow eye are useful for diagnosis2).
To differentiate secondary causes, caution is needed if the fellow eye shows an open angle and deep anterior chamber, the affected eye has relatively clear cornea, or iris neovascularization is present2).
Comprehensive evaluation of medication history, lens status, angle and iris anatomy, and laterality (unilateral/bilateral) of acute angle closure helps identify the cause. Bilateral acute angle closure is rare but suggests a drug-related mechanism such as topiramate or SSRIs2).
Treatment of drug-induced AACG prioritizes rapid intraocular pressure reduction and intervention based on the underlying mechanism2).
Medical Treatment
Acetazolamide: Immediate administration is recommended when IOP ≥40 mmHg. Intravenous injection (10 mg/kg) is preferable in cases of vomiting or when rapid effect is needed3).
Mannitol: Considered when response to acetazolamide is insufficient. Administer 0.5–1.5 g/kg as a 15–20% solution intravenously3).
Pilocarpine: Instill 1–2% eye drops. It is ineffective during sphincter ischemia; miosis may be achieved after IOP reduction3).
Steroid eye drops: Administer frequently (4–6 times daily) to reduce inflammation3).
Laser and Surgical Treatment
Laser peripheral iridotomy (LPI): Standard treatment for pupillary block. Performed once the cornea is sufficiently clear. Prophylactic LPI is also performed on the fellow eye1, 3).
Laser iridoplasty: Useful when corneal edema persists making LPI difficult, or when IOP does not decrease within 1–2 hours of medical therapy3).
Lens extraction: Considered when there is no response to medication or LPI3).
Topiramate-type treatment: Immediate discontinuation of the causative drug, cycloplegic eye drops, and steroid eye drops are basic. Laser iridotomy is ineffective1).
In a case of olanzapine-induced AAC, after administration of timolol 0.5% and brimonidine 0.15% eye drops, oral acetazolamide, and pilocarpine 2%, Nd:YAG laser iridotomy was performed, and the next day IOP decreased from 51 mmHg to 20 mmHg, and visual acuity improved from 6/200 to 20/301). Prophylactic laser iridotomy was also performed on the fellow eye1).
Systemic medications (acetazolamide, mannitol) require caution in elderly patients or those with comorbidities, as they can cause serious side effects ranging from paresthesia and confusion to pulmonary edema and acute renal failure2).
QHow is drug-induced acute angle-closure glaucoma treated?
A
Treatment varies depending on the underlying mechanism. In pupillary block type, first lower intraocular pressure with ocular hypotensive agents (intravenous acetazolamide, mannitol infusion), and perform laser iridotomy once the cornea becomes clear. Prophylactic laser iridotomy is also performed on the fellow eye. In non-pupillary block types such as topiramate, immediate discontinuation of the causative drug is most important, and cycloplegics and steroid eye drops are used. In all cases, identification and discontinuation of the causative drug, as well as coordination with the prescribing physician, are necessary.
6. Pathophysiology and detailed mechanism of onset
Pupillary block is the most common mechanism of drug-induced AACG3). When drugs with sympathomimetic or parasympatholytic effects induce mydriasis, the contact area between the iris and lens increases1). This increases resistance to trans-pupillary flow of aqueous humor from the posterior chamber to the anterior chamber, causing posterior chamber pressure to exceed anterior chamber pressure3).
Elevated posterior chamber pressure causes the iris to bulge forward (iris bombé), and the peripheral iris covers the trabecular meshwork, obstructing aqueous outflow and leading to a rapid rise in intraocular pressure3). Moderate mydriasis with co-activation of both the sphincter and dilator muscles carries the highest risk3).
In the olanzapine case, weak anticholinergic effects induced mydriasis, and pupillary block occurred in an anatomically predisposed eye1). Angle-closure glaucoma due to atypical antipsychotics is rare, with fewer reports compared to SSRIs and tricyclic antidepressants1).
Topiramate and sulfa drugs can cause ciliary body effusion due to idiosyncratic drug reactions 3). This leads to forward rotation of the ciliary body, relaxation of the zonules, and swelling of the lens, causing the entire iris-lens diaphragm to move forward and occlude the angle 2).
This mechanism can occur in patients with either open or narrow angles. Bilateral acute angle closure with uveal effusion caused by venlafaxine and escitalopram has also been reported 2).
Plateau iris configuration occurs when anteriorly positioned ciliary processes push the peripheral iris forward, directly occluding the angle upon dilation 3). If elevated intraocular pressure persists after relief of pupillary block, plateau iris should be suspected.
QWhat is the difference between pupillary block and non-pupillary block types?
A
In the pupillary block type, dilation increases contact between the iris and lens, obstructing aqueous humor flow from the posterior to anterior chamber, causing the iris to bulge forward and occlude the angle. Mydriatics, anticholinergics, and sympathomimetics are causes, and laser iridotomy is effective. In contrast, the non-pupillary block type is caused by ciliary body edema and choroidal effusion due to topiramate or sulfa drugs, pushing the entire iris-lens diaphragm forward. Iridotomy is ineffective in this type; discontinuation of the causative drug and cycloplegics are the mainstays of treatment. Bilateral involvement strongly suggests non-pupillary block.
In an international consensus published in 2025, the term APACA (acute primary angle closure attack) was proposed for acute primary angle closure attacks 2). This term emphasizes the acute and emergent nature of the condition and clarifies distinction from secondary causes 2). There was 100% agreement that rapid intraocular pressure reduction should take priority over accurate diagnosis 2).
The consensus statement confirmed with 88.24% agreement that drugs with mydriatic and cycloplegic effects can induce APACA in anatomically predisposed eyes 2). Caution is needed when prescribing such drugs to at-risk patients, and a detailed medication history is an important diagnostic clue 2).
Pharmacologic dilation for diagnostic purposes is safe in the general population, and the risk of missing fundus disease due to insufficient dilation far outweighs the risk of inducing angle closure 3). In patients with a history of angle closure who have received appropriate prophylactic treatment (laser iridotomy), dilation is usually safe 3). Prophylactic constriction with pilocarpine after dilation should be avoided because it can cause pupillary fixation in a mid-dilated position and increase the risk of angle closure 3).
Alarfaj MA, Almater AI. Olanzapine-Induced Acute Angle Closure. The American journal of case reports. 2021;22:e934432. doi:10.12659/AJCR.934432. PMID:34803156; PMCID:PMC8628565.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.