Ophthalmic emergencies are a group of highly urgent eye diseases in which delay in appropriate treatment can lead to irreversible visual impairment or blindness. The eye is composed of delicate neural tissue and has extremely low tolerance to ischemia, trauma, and sudden elevation of intraocular pressure.
A particularly important aspect of ophthalmic emergencies is that several diseases involve a “race against time.” In central retinal artery occlusion (CRAO), retinal ganglion cells are thought to undergo irreversible necrosis within 90 to 240 minutes of onset 1), establishing the concept of “time is vision,” analogous to “time is brain” in cerebral infarction. In acute angle-closure glaucoma attacks, intraocular pressure can reach 60–80 mmHg, and without prompt treatment, optic nerve damage becomes irreversible 2). Chemical injuries (especially alkali) have strong penetrating ability, and copious irrigation immediately after injury determines the prognosis 3). In retinal detachment, visual prognosis improves significantly with surgery before macular detachment (macula-on), so early recognition of prodromal symptoms is essential 4).
On the other hand, conditions such as anterior ischemic optic neuropathy, optic neuritis, and corneal ulcers are semi-urgent diseases that can be managed with treatment within the same day or the next day. Accurate distinction of urgency is the first step in protecting the patient’s vision.
QWhat should I do if I suddenly lose vision in one eye?
A
Sudden painless vision loss in one eye may indicate central retinal artery occlusion (CRAO). In CRAO, irreversible necrosis of retinal ganglion cells is thought to begin within 90 to 240 minutes of onset 1), so immediate emergency ophthalmic care is necessary. CRAO is also closely associated with cerebral infarction, and about 25% of cases have ipsilateral carotid artery stenosis 5), so it may be advisable to choose emergency transport (call 119). Never “wait and see” — seek care promptly.
2. Most Urgent Symptoms and Diseases (Seek Care Immediately)
Mahmoud A, Abid F, Khairallah M, et al. Case Report: Central retinal artery occlusion following sildenafil intake. F1000Research. 2022;11:600. Figure 1. PMCID: PMC9490277. doi:10.12688/f1000research.122087.1. License: CC BY 4.0.
Typical fundus findings of CRAO: the entire retina is whitened except for the area supplied by the cilioretinal artery (black arrow), and the relative redness of the fovea stands out. This corresponds to the cherry-red spot of central retinal artery occlusion (CRAO) discussed in the section “2. Most Urgent Symptoms and Diseases.”
The following diseases are the most urgent conditions where treatment within “hours” greatly affects visual prognosis.
Reason for urgency: The retina is supplied by end arteries and has extremely low ischemic tolerance. Retinal ganglion cells undergo irreversible necrosis within 90–240 minutes of onset 1). It is referred to as “retinal stroke” 5).
Treatment: Ocular massage, anterior chamber paracentesis, intra-arterial thrombolysis (tPA, within 4.5 hours of onset) 1). Collaboration with neurology is necessary to evaluate for concurrent cerebral infarction.
② Acute Angle-Closure Glaucoma Attack
Symptoms: Severe eye pain, headache, nausea/vomiting, blurred vision due to corneal edema, redness. Intraocular pressure rises rapidly to 60–80 mmHg 2).
Reason for urgency: High intraocular pressure causes rapid progression of optic nerve ischemia, and delayed treatment leads to irreversible optic nerve damage 2). Be aware of the risk of misdiagnosis as gastrointestinal or cerebrovascular disease due to vomiting and headache 2).
Symptoms (sequence of prodromal symptoms): Photopsia (flashes of light) → sudden increase in floaters → visual field defect (“curtain coming down”) 4).
Reason for urgency: Once the macula detaches, visual recovery becomes limited. Surgery before macular detachment (macula-on) significantly improves visual prognosis 4). Risk increases with high myopia, post-cataract surgery, and trauma 4).
Treatment: Closure of retinal breaks (laser, cryopexy), scleral buckling, vitrectomy4).
④ Ocular Trauma / Chemical Injury
Symptoms: Exposure to chemicals, foreign body penetration, blunt trauma to the eye. Severe pain, tearing, photophobia, decreased vision.
Basis for urgency: In alkali injuries, saponification of fats allows penetration deep into tissues, reaching the corneal stroma, anterior chamber, and lens 3). Acid injuries tend to penetrate less deeply than alkali due to self-limiting protein coagulation 3).
Initial management: Immediate copious irrigation at the injury site (tap water acceptable). Continuous irrigation for at least 30 minutes 3). Severity assessment using the Roper-Hall classification or Dua classification 3).
Basis for urgency: Most commonly spreads from sinusitis, and is more frequent in children 6). Progression to cavernous sinus thrombosis is a life-threatening emergency 6).
Treatment: Intravenous broad-spectrum antibiotics (inpatient management). Surgical drainage if abscess forms 6).
3. Semi-urgent symptoms and conditions (within the same day to the next day)
The following conditions are semi-urgent, requiring an ophthalmology visit within the same day or the next day. They are not as imminent as the most urgent conditions, but if left untreated, they carry a risk of irreversible damage.
AION: Acute onset in individuals aged 50 years or older. Inferior altitudinal defect is common 7). In arteritic AION (giant cell arteritis [GCA]-related), exclusion of temporal arteritis is urgent, requiring ESR and CRP measurement and prompt corticosteroid administration 7). Emergency management is needed due to the risk of progression to the fellow eye.
Optic neuritis: More common in young women. Acute vision loss with pain on eye movement. Association with multiple sclerosis (MS) is important, and MRI to search for central nervous system lesions is necessary 8).
Oculomotor nerve palsy with pupillary dilation suggests compression by a posterior communicating artery aneurysm before rupture. Urgent search for aneurysm using head MRI/MRA and CTA is mandatory 9).
Diabetic oculomotor nerve palsy often spares the pupil, which is useful for differentiating from aneurysm 9).
University hospitals and general hospitals with ophthalmology emergency departments are suitable facilities that can provide 24-hour care. If you have a regular eye doctor, it is advisable to check their emergency contact information in advance. If CRAO (sudden painless vision loss) or chemical exposure to the eye is suspected at night or on holidays, it is important to choose emergency transport via 119 without waiting for the eye clinic to open. Using local emergency medical information (such as #7119) to find the nearest available facility is also effective.
In ophthalmic emergencies, appropriate initial management immediately after injury can greatly affect the final visual prognosis. Accurate knowledge of first aid is essential for patients, their families, and non-ophthalmic medical personnel.
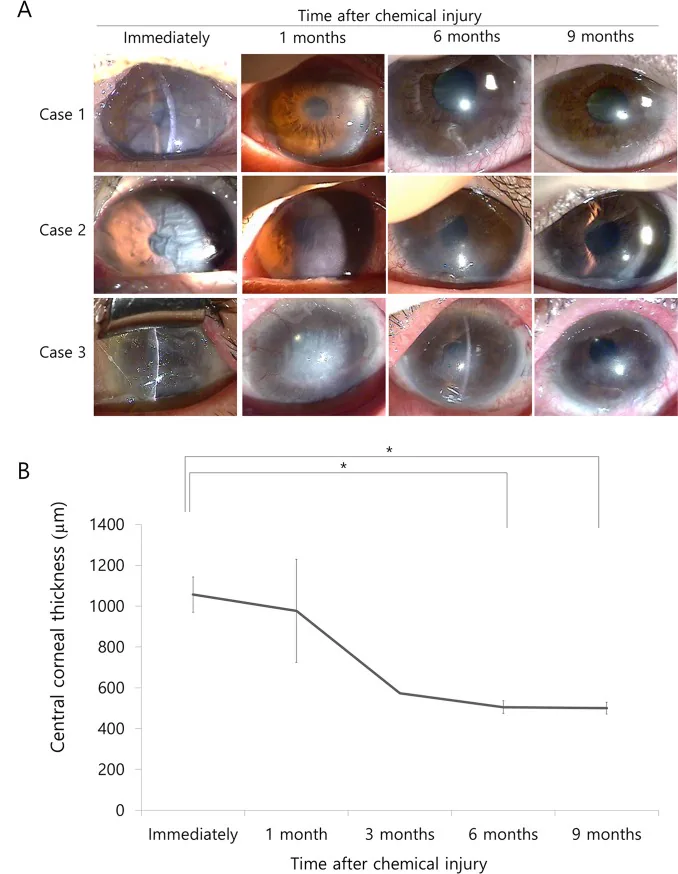
Choi SO, Jeon HS, Hyon JY, et al. Recovery of Corneal Endothelial Cells from Periphery after Injury. PLoS One. 2015;10(9):e0138076. Figure 1. PMID: 26378928; PMCID: PMC4574742; DOI: 10.1371/journal.pone.0138076. License: CC BY 4.0.
Slit-lamp photographs and central corneal thickness (CCT) data showing the course of severe corneal edema and Descemet’s folds immediately after chemical injury, progressing to clearing at 6 months post-injury. This corresponds to the purpose and prognosis of initial management for chemical injury discussed in section “5. Basics of First Aid.”
The time from injury to the start of irrigation is directly related to the rate of pH recovery on the ocular surface and the final prognosis 3).
Immediately start irrigating the eye with copious tap water at the site of injury (tap water is acceptable even if no specialized irrigation solution is available).
Irrigate with the eye open (if possible, evert the eyelids).
Perform continuous irrigation for at least 30 minutes.
Seek emergency care while irrigating (do not wait until irrigation is complete).
Inform the medical staff of the identity of the chemical involved (alkali or acid, product name) at the time of consultation.
Check pH after irrigation (target: pH 7.0–7.4) 3).
Penetrating trauma (puncture by sharp object): Do not press on the eyeball. Cover the eye with a clean cup or protective shield and transport without applying pressure11). Do not instill eye drops or press with gauze.
Blunt trauma (contusion): Cool and rest. If there are signs of globe rupture such as low intraocular pressure, hyphema, or vitreous prolapse, transport urgently11).
Ocular surface foreign body: Rinse with artificial tears or clean water. Do not forcibly remove deeply embedded foreign bodies11).
Emergency management of acute angle-closure glaucoma
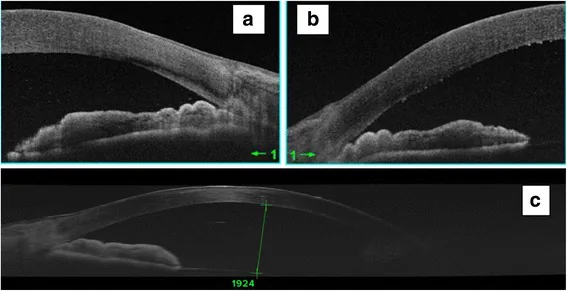
Mahmoud A, Abid F, Ksiaa I, et al. Bilateral acute angle-closure glaucoma following tramadol subcutaneous administration. BMC Ophthalmol. 2018;18:50. Figure 2. PMCID: PMC5816554. doi:10.1186/s12886-018-0715-4. License: CC BY 4.0.
Anterior segment OCT (AS-OCT) performed in the acute phase shows bilateral angle closure (a, b) and marked shallowing of the anterior chamber (c). This corresponds to the mechanism of aqueous outflow obstruction in acute angle-closure glaucoma discussed in section “6. Pathophysiology”.
Do not lie flat; maintain a sitting or semi-sitting position
Avoid dark environments (pupil dilation in darkness worsens symptoms)
Seek emergency ophthalmological care promptly
Miotic agents (pilocarpine) should be administered by an ophthalmologist after examination; do not attempt self-administration
QWhat should be done first if a chemical substance enters the eye?
A
Immediately start rinsing the eye with a large amount of tap water as the top priority3). Even if no specialized eyewash solution is available, tap water or bottled water is acceptable. Continuously rinse with the eye open for at least 30 minutes. Seek emergency care while rinsing. Alkaline chemicals (e.g., lime, cement, mold remover, bleach) are particularly dangerous and require more aggressive action. Inform the medical staff of the product name when visiting the hospital.
The retina is supplied by end arteries (with poor anastomoses between arteries) and has lower tolerance to ischemia than the brain 1). Retinal ganglion cells undergo irreversible necrosis 90–240 minutes after the onset of ischemia 1). Due to this biological characteristic, it is called a “retinal stroke” 5), and hyperacute management similar to that for cerebral infarction is required. Approximately 25% of CRAO cases have ipsilateral internal carotid artery stenosis, and there is a risk of concurrent or sequential cerebral infarction, making collaboration with neurology essential 5).
Inside the eye, aqueous humor is produced by the ciliary body and drains through the angle (the junction of the iris and cornea) to maintain intraocular pressure. In acute angle-closure glaucoma, the pathway is: pupillary block (adhesion between the posterior iris and anterior lens) → increased posterior chamber pressure → forward bulging of the iris (iris bombé) → rapid closure of the peripheral angle → inability of aqueous humor to drain → sharp rise in intraocular pressure (60–80 mmHg) 2). High intraocular pressure impairs blood circulation to the optic nerve head, and damage due to optic nerve ischemia becomes irreversible if treatment is delayed 2).
Alkali injuries (lime, cement, mold removers, etc.): Hydroxide ions (OH⁻) cause saponification of fats, dissolving cell membranes and penetrating deep into tissues. They can reach the corneal stroma, anterior chamber, lens, and ciliary body. Because penetration continues, the prognosis is particularly poor 3).
Acid injuries (sulfuric acid, hydrochloric acid, etc.): Hydrogen ions (H⁺) coagulate proteins, and the formed coagulation layer provides a self-limiting effect that partially blocks further penetration. Penetration is shallower compared to alkalis 3).
Returning the pH to 7.0–7.4 by irrigation is the first step to stop the progression of tissue damage 3).
In rhegmatogenous retinal detachment, fluid produced by liquefaction of the vitreous enters the subretinal space through a tear, and the detachment spreads between the sensory retina and the retinal pigment epithelium (RPE) 4). The macula (the posterior pole including the fovea) is the most vision-critical area of the retina; when it detaches, irreversible damage to photoreceptor cells begins. While many cases of surgery before macular detachment (macula-on surgery) achieve postoperative visual acuity of 1.0 or better, visual recovery is often limited after macular detachment (macula-off) 4).
Regarding the efficacy of intra-arterial thrombolytic therapy (tissue plasminogen activator: tPA) for CRAO, visual improvement has been reported when administered within 4.5 hours of onset 1). However, evaluation of complications including bleeding risk is necessary, and large-scale randomized controlled trials are ongoing to verify efficacy and safety. Application of acute management protocols similar to those for cerebral infarction to the ophthalmology field is being considered 5).
Development of remote fundus photography and tele-triage systems using smartphones and tablets is progressing 12). Systems are in the demonstration trial stage, where fundus images taken by non-ophthalmologists in regions or during nighttime hours without ophthalmologists are interpreted in real time by ophthalmologists to determine urgency.
Simple self-check of visual acuity and visual field using smartphones
Development of simple measurement tools for visual acuity and visual field using smartphone apps is active 12). They are expected to be applied for early detection of retinal detachment and daily monitoring of visual field defects, but further verification of accuracy comparable to specialized equipment is needed.
Automated detection of ophthalmic emergencies using AI image diagnosis
AI fundus image analysis using deep learning is being applied not only to diabetic retinopathy but also to automated detection of glaucoma, AMD, CRAO, and retinal detachment12). Using it for screening in emergency departments and primary care may streamline appropriate triage to ophthalmologists.
Hayreh SS, Zimmerman MB. Central retinal artery occlusion: visual outcome. Am J Ophthalmol. 2005;140(3):376-391. doi:10.1016/j.ajo.2005.03.038.
Lam DS, Tham CC, Lai JS, et al. Current approaches to the management of acute primary angle closure. Curr Opin Ophthalmol. 2007;18(2):104-109. doi:10.1097/icu.0b013e32808374c9.
Eslani M, Baradaran-Rafii A, Movahedan A, et al. The ocular surface chemical burns. J Ophthalmol. 2014;2014:196827. doi:10.1155/2014/196827.
Feltgen N, Walter P. Rhegmatogenous retinal detachment—an ophthalmologic emergency. Deutsches Arzteblatt international. 2014;111(1-2):12-21; quiz 22. doi:10.3238/arztebl.2014.0012. PMID:24565273; PMCID:PMC3948016.
Biousse V, Nahab F, Newman NJ. Management of acute retinal ischemia: follow the guidelines! Ophthalmology. 2018;125(10):1597-1607.
Nageswaran S, Woods CR, Benjamin DK Jr, et al. Orbital cellulitis in children. Pediatr Infect Dis J. 2006;25(8):695-699. doi:10.1097/01.inf.0000227820.36036.f1.
Hayreh SS. Ischemic optic neuropathies — where are we now? Graefes Arch Clin Exp Ophthalmol. 2013;251(8):1873-1884.
Beck RW, Cleary PA, Anderson MM Jr, et al. A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group. N Engl J Med. 1992;326(9):581-588. doi:10.1056/nejm199202273260901.
Fang C, Leavitt JA, Hodge DO, Holmes JM, Mohney BG, Chen JJ. Incidence and Etiologies of Acquired Third Nerve Palsy Using a Population-Based Method. JAMA ophthalmology. 2017;135(1):23-28. doi:10.1001/jamaophthalmol.2016.4456. PMID:27893002; PMCID:PMC5462106.
Austin A, Lietman T, Rose-Nussbaumer J. Update on the Management of Infectious Keratitis. Ophthalmology. 2017;124(11):1678-1689. doi:10.1016/j.ophtha.2017.05.012. PMID:28942073; PMCID:PMC5710829.
Kuhn F, Morris R, Witherspoon CD, et al. A standardized classification of ocular trauma. Ophthalmology. 1996;103(2):240-243.
Salongcay RP, Silva PS. The role of teleophthalmology in the management of diabetic retinopathy. Asia Pac J Ophthalmol (Phila). 2018;7(1):17-21. doi:10.22608/apo.2017479.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.