Ocular diseases associated with atopic dermatitis (AD) are collectively called “atopic eye disease.” The three major complications are cataract, retinal detachment, and keratoconus, with long-term eye rubbing and tapping being the main mechanisms of onset.
AD is a chronic inflammatory skin disease with an immunological background, and the risk of ocular complications is particularly high when skin lesions on the eyelids and face are severe. According to a survey by the Ministry of Education, Culture, Sports, Science and Technology (2004–2006), the prevalence rate is 5.5% on average among elementary, junior high, and high school students, and approximately 2–3% of adults are also affected.
Corneal shape abnormality in approximately 7–30% of AD patients
Mechanical deformation and weakening of the corneal stroma due to eye rubbing
The key findings for diagnosing AD are: (1) itching, (2) skin rash (distribution and characteristics of eczematous lesions), (3) course (chronic relapsing), and (4) atopic predisposition (family history and associated allergic diseases).
Regarding the incidence of cataracts in patients with a habit of eye rubbing or tapping, a study of 101 cases at the Mayo Clinic (Brunsting report) reported approximately 10% 6). Rapid vision loss in young individuals (teens to 30s) is characteristic, showing a clinical picture different from age-related cataracts.
QIf I have atopic dermatitis, am I more likely to develop eye diseases?
A
Yes. The risk of cataracts, retinal detachment, and keratoconus is increased. The risk is especially high when there is severe dermatitis on the face and eyelids, and when there is a habit of rubbing or hitting the eyes. Early ophthalmologic follow-up is important.
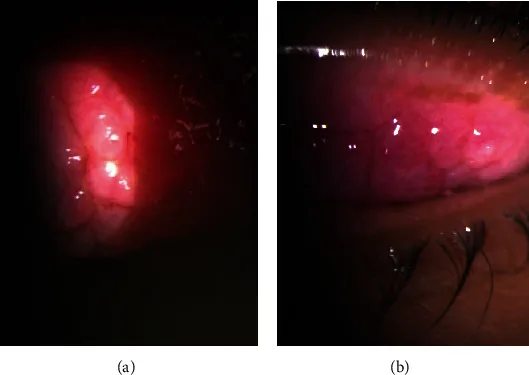
Annisa DN, Suharko H, Lumban Gaol H, Viona V. Combined papillectomy and autologous conjunctival membrane graft as management of giant papillae for severe, refractory palpebral vernal keratoconjunctivitis—A case report. Case Rep Ophthalmol Med. 2024;2024:9973441. Figure 2. PMCID: PMC11319060. License: CC BY 4.0.
Dense giant papillae (cobblestone papillae) are seen on the everted upper tarsal conjunctiva in both eyes (a: right eye, b: left eye). This corresponds to the giant papilla formation in atopic keratoconjunctivitis (AKC) discussed in section “2. Main symptoms and clinical findings.”
Atopic cataract
Age of onset: Commonly occurs in young people in their teens to thirties. Rapid vision loss.
Characteristics of opacity: “Star-shaped,” “asteroid,” or “crack-like linear opacities” under the anterior capsule. The morphology resembles traumatic (contusion) cataract, and differentiation from steroid-induced cataract with posterior subcapsular opacity is important.
Progression: Often rapidly progressive, reaching severe opacity within weeks to months.
Symptoms: Acute floaters, photopsia, visual field defect. May occur acutely after eye rubbing.
Features: Commonly occurs in young people and may be bilateral. In cases with Zinn zonule damage, it may occur simultaneously with cataract.
Keratoconus
Pathology: Progressive corneal protrusion and thinning.
Symptoms: Decreased visual acuity and glare due to irregular astigmatism. Visual acuity that cannot be fully corrected with glasses occurs.
Association: Mechanical stimulation from eye rubbing is a modifying factor in the onset and progression. It is more frequent in cases of atopic dermatitis complicated by allergic conjunctivitis9).
Blepharitis / Allergic Conjunctivitis
Findings: Eyelid swelling, itching, eye discharge, papillary reaction of the conjunctiva.
Characteristics: In patients with severe atopic dermatitis, it takes a chronic course and, by inducing eye rubbing behavior, further increases the risk of developing cataracts, retinal detachment, and keratoconus.
Complications: Corneal epithelial damage and keratitis due to repeated anterior segment inflammation may occur.
Slit-lamp examination reveals the morphology of anterior subcapsular opacities (star-shaped, stellate, or cracked-ice appearance). This morphology is clearly different from steroid-induced cataracts (posterior subcapsular opacity) and closely resembles traumatic cataract, which is a key diagnostic point. Fundus examination with dilated pupils carefully evaluates peripheral retinal tears and detachments.
QHow is atopic cataract different from ordinary cataract?
A
It occurs in young individuals (teens to 30s) and presents characteristic star-shaped or stellate opacities in the anterior subcapsular region of the lens. Physical stimulation from habitual eye rubbing or tapping is involved in its onset, and it differs from age-related posterior subcapsular opacity in morphology, age of onset, and mechanism.
Eye rubbing and tapping behavior is the greatest modifying factor for atopic eye disease. Itching due to blepharitis triggers this behavior, and long-term physical stimulation to the eyeball causes ocular complications through the following pathways:
Direct blunt trauma to the lens → anterior subcapsular opacity (same mechanism as traumatic cataract)
Disruption of the blood-ocular barrier → influx of eosinophil granule proteins (ECP, MBP, etc.) into the eye → lens protein denaturation
Repeated mechanical stress on the zonules of Zinn → micro-tears → lens subluxation / phacodonesis
The involvement of topical steroids in the development of atopic cataract is considered unlikely. Atopic cataracts were reported before the clinical introduction of steroids (before the 1950s)6), and no significant change in cataract incidence has been observed before and after the introduction of steroids. However, caution is needed because steroid eye ointment can enter the conjunctival sac and cause elevated intraocular pressure.
The more severe the dermatitis on the face and eyelids, the stronger the urge to scratch the eyes, increasing the risk of ocular complications. Serum TARC levels, serum LDH levels, peripheral blood eosinophil count, and serum total IgE levels are indicators of AD severity and are also used as indirect indicators of ocular complication risk.
Population-based cohort studies have shown that AD patients have a significantly higher risk of cataract, glaucoma, and retinal detachment compared to non-AD individuals12).
Eosinophil activation due to enhanced type 2 immune responses (IL-4, IL-13, IL-31) also occurs locally in the eye. Allergic inflammation is triggered in the conjunctiva, which can lead to goblet cell proliferation, giant papilla formation, and corneal epithelial damage2)3).
The diagnosis centers on morphological confirmation of anterior subcapsular opacity using slit-lamp microscopy. Characteristic findings include “star-shaped,” “asteroid,” or “crack-like linear opacities,” which can be differentiated morphologically from steroid-induced cataract that presents with posterior subcapsular opacity. This type of cataract often occurs in younger patients with relatively soft nuclei, making preoperative assessment of nuclear hardness important. Lens mobility and the state of the zonules of Zinn are evaluated preoperatively using ultrasound biomicroscopy (UBM) or anterior segment OCT.
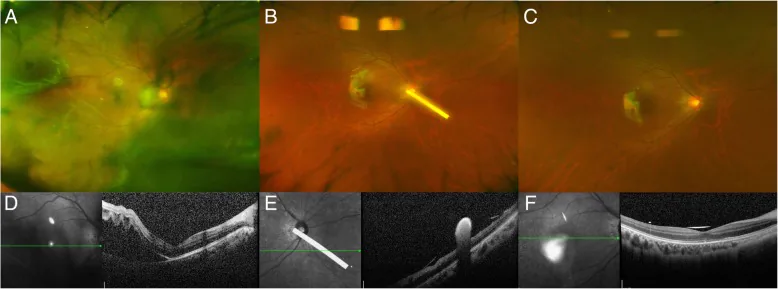
Cho AR, Yoon YH. Adjunctive dexamethasone implant in patients with atopic dermatitis and retinal detachment undergoing vitrectomy and silicone oil tamponade: an interventional case series. BMC Ophthalmol. 2019;19:86. doi: 10.1186/s12886-019-1094-1. Figure 1. PMCID: PMC6448232. License: CC BY 4.0.
Wide-angle fundus photograph (a) shows inferotemporal retinal detachment and vitreous opacity; retinal reattachment is confirmed at postoperative day 3 (b) and week 4 (c). The lower OCT images (d–f) show pre- and postoperative changes of detachment involving the macula. This corresponds to the dilated fundus evaluation of atopic dermatitis-related retinal detachment discussed in section “4. Diagnosis and Examination Methods.”
Thorough examination of the peripheral fundus under mydriasis is essential. AD patients have a higher frequency of juvenile lattice degeneration and tears compared to non-AD patients 8). Acute onset of floaters or photopsia requires urgent fundus examination.
QHow often should the eyes of a child with atopic dermatitis be checked?
A
If there is severe dermatitis on the face or eyelids, at least annual ophthalmologic examination is recommended. More frequent checks are desirable if the child has a habit of rubbing or hitting the eyes. If decreased vision, floaters, or photopsia are noticed, seek medical attention promptly.
Phacoemulsification (PEA) is performed and an intraocular lens is inserted. The procedure is basically the same as for age-related cataract, but the following points require attention.
Risk of Zinn zonule rupture: If rupture is suspected on preoperative evaluation, consider using a capsular tension ring (CTR). In cases of severe rupture, consider a sutured intraocular lens.
Check for concurrent retinal detachment or tears: Perform dilated fundus examination preoperatively to check for tears or degeneration, and perform laser photocoagulation preoperatively if necessary.
Softness of the nucleus: The lens nucleus in young patients is soft, making phacoemulsification relatively easy, but careful capsular management is required.
Since eyelid and periorbital dermatitis directly cause eye scratching, active control in collaboration with a dermatologist is important.
Mild cases: Apply moisturizers such as white petrolatum ophthalmic ointment. Maintaining skin barrier function is the basis of long-term management.
Moderate to severe cases: Use steroid ophthalmic ointment.
Prescription example: Prednisolone ophthalmic ointment, apply appropriate amount twice daily, adjust according to symptoms.
Steroid ophthalmic ointments are all classified as weak in pharmacological potency. Be careful as they may cause increased intraocular pressure if they enter the conjunctival sac.
If no improvement with steroid ophthalmic ointment: After consulting a dermatologist, use 0.03% or 0.1% Protopic ointment (tacrolimus hydrate).
Prescription example: Protopic ointment, apply once or twice daily.
After improvement, do not discontinue abruptly; proactive therapy with application once daily on about two days per week reduces the frequency of relapse 1).
Controlling eye scratching and tapping behavior is fundamental to preventing all ocular complications. Ophthalmologists need to work with dermatologists to actively treat facial AD and blepharitis. With the widespread use of tacrolimus ointment, control of blepharitis has improved, and a decrease in the incidence of atopic cataracts is expected.
QIs it safe to apply steroid ointment around the eyes?
A
Ophthalmic steroid ointments (such as prednisolone ophthalmic ointment) can be used around the eyes, but their pharmacological potency is weak. Since they may increase intraocular pressure if they enter the conjunctival sac, be careful not to get them into the eye when applying. Regular intraocular pressure checks are recommended during long-term use.
The development of ocular diseases associated with AD results from physical stimuli starting with eye rubbing and hitting behaviors, which damage ocular tissues through multiple pathways.
Repeated blunt force to the eyeball → direct damage to the anterior lens capsule (same mechanism as traumatic cataract)
Disruption of the blood-ocular barrier → influx of eosinophil granule proteins (ECP, MBP, etc.) into the eye → induction of aggregation and denaturation of lens crystallin (α-crystallin)
These combined effects lead to the formation of anterior subcapsular opacities. The morphology resembling traumatic cataract (star-shaped, stellate, or cracked-ice pattern) reflects this mechanism4)7)
In AD, enhanced type 2 immune responses (overproduction of IL-4, IL-13, IL-31) activate eosinophils, which release inflammatory mediators locally in the eye. Th2-type allergic inflammation also occurs in the conjunctiva, leading to goblet cell proliferation, giant papilla formation, and corneal epithelial damage3).
The following evidence supports that topical steroids are not the main cause of atopic cataract development: ① Cataracts were reported before the clinical introduction of steroids in the 1950s6); ② No significant change in cataract incidence was observed before and after the introduction of steroids. This suggests that atopic cataract is essentially caused by physical stimuli such as eye rubbing and tapping, as well as immunological mechanisms.
With the advent of tacrolimus ointment (Protopic), control of blepharitis and periorbital AD is expected to be better than with conventional topical steroid therapy. A virtuous cycle is anticipated: control of blepharitis → reduction of itching → reduction of eye rubbing → decreased incidence of atopic cataract, retinal detachment, and keratoconus1). Multiple reports have accumulated on the efficacy and safety of topical tacrolimus therapy for atopic blepharitis1).
Dupilumab (anti-IL-4 receptor alpha antibody) has been approved and widely used as a first-line biologic for moderate to severe AD. However, conjunctivitis has been reported in approximately 10-30% of patients during use5)10), and cases of anterior uveitis have also been reported. The exact mechanism of dupilumab-induced conjunctivitis is still under investigation, and many details of the pathology remain unclear. Ophthalmic monitoring is recommended during dupilumab use.
For management of conjunctivitis, artificial tears, low-concentration steroid eye drops, and cyclosporine eye drops are used, but discontinuation of dupilumab may be necessary in some cases5).
JAK inhibitors such as baricitinib, upadacitinib, and abrocitinib have been approved in Japan for moderate to severe AD. Ocular complications (especially increased risk of herpetic eye infections) are under ongoing investigation.
Regarding the inhibitory effect of corneal cross-linking (CXL) on the progression of AD-related keratoconus, reports of efficacy in young patients with AD as an underlying disease have been accumulating 11). It is thought that performing CXL after improvement in control of eye rubbing behavior leads to better long-term outcomes, but evidence on long-term outcomes is still being accumulated.
Epidemiological quantification of ocular complication risk
Population-based cohort studies have statistically quantified the association between AD and ocular complications (cataract, glaucoma, retinal detachment) 12). Future challenges include refining risk factors through larger prospective studies and elucidating the causal pathway linking AD severity, eye rubbing behavior, and the development of ocular complications.
Takahashi Y, Ichinose A, Kakizaki H. Topical tacrolimus (FK506) for atopic blepharitis: risk factors for corneal complications. Ophthalmology. 2012;119(11):2200-2203.
Garrity JA, Liesegang TJ.. Ocular complications of atopic dermatitis. Can J Ophthalmol. 1984;19(1):21-24. PMID:6713265.
Rich LF, Hanifin JM. Ocular complications of atopic dermatitis and other eczemas. International ophthalmology clinics. 1985;25(1):61-76. doi:10.1097/00004397-198502510-00005. PMID:3972488.
Taniguchi H, Ohki M, Isogai N, et al. Atopic cataract: a morphological study. Graefes Arch Clin Exp Ophthalmol. 1999;237(7):559-566.
Akinlade B, Guttman-Yassky E, de Bruin-Weller M, Simpson EL, Blauvelt A, Cork MJ, et al. Conjunctivitis in dupilumab clinical trials. The British journal of dermatology. 2019;181(3):459-473. doi:10.1111/bjd.17869. PMID:30851191; PMCID:PMC6850316.
BRUNSTING LA, REED WB, BAIR HL. Occurrence of cataracts and keratoconus with atopic dermatitis. A.M.A. archives of dermatology. 1955;72(3):237-41. doi:10.1001/archderm.1955.03730330017003. PMID:13248240.
Matsuo T, Saito H, Matsuo N. Cataract and aqueous flare levels in patients with atopic dermatitis. American journal of ophthalmology. 1997;124(1):36-9. doi:10.1016/s0002-9394(14)71641-1. PMID:9222230.
Hida T, Tano Y, Okinami S, Ogino N, Inoue M. Multicenter retrospective study of retinal detachment associated with atopic dermatitis. Japanese journal of ophthalmology. 2000;44(4):407-18. doi:10.1016/s0021-5155(00)00174-x. PMID:10974298.
Liberman P, Shifera AS, Berkenstock M. Dupilumab-Associated Conjunctivitis in Patients With Atopic Dermatitis. Cornea. 2020;39(6):784-786. doi:10.1097/ICO.0000000000002262. PMID:31985517.
Wollenberg A, Barbarot S, Bieber T, Christen-Zaech S, Deleuran M, Fink-Wagner A, Gieler U, Girolomoni G, Lau S, Muraro A, Czarnecka-Operacz M, Schäfer T, Schmid-Grendelmeier P, Simon D, Szalai Z, Szepietowski JC, Taïeb A, Torrelo A, Werfel T, Ring J, European Dermatology Forum (EDF), the European Academy of Dermatology and Venereology (EADV), the European Academy of Allergy and Clinical Immunology (EAACI), the European Task Force on Atopic Dermatitis (ETFAD), European Federation of Allergy and Airways Diseases Patients’ Associations (EFA), the European Society for Dermatology and Psychiatry (ESDaP), the European Society of Pediatric Dermatology (ESPD), Global Allergy and Asthma European Network (GA2LEN) and the European Union of Medical Specialists (UEMS). Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part II. J Eur Acad Dermatol Venereol. 2018;32(6):850-878. doi:10.1111/jdv.14888. PMID:29878606.
Nguyen KD, Lee EE, Yue H, et al. Atopic dermatitis and risk of cataract, glaucoma, and retinal detachment: a population-based cohort study. Am J Ophthalmol. 2022;236:245-253.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.