Posterior capsule opacification (PCO) is a disease in which residual lens epithelial cells (LECs) after cataract surgery proliferate, migrate, and differentiate, causing secondary opacification of the preserved posterior capsule. It is also called “secondary cataract.”
The broad term “after cataract” refers to all tissue reactions occurring within the lens capsule after cataract surgery, including Elschnig pearls, posterior capsule fibrosis, and liquefied after-cataract. Among these, the condition that affects the pupillary area and impairs visual function is clinically called “posterior capsule opacification (PCO).”
It occurs in 11.8% at 1 year, 20.7% at 3 years, and 28.4% at 5 years postoperatively, making it the most frequent complication after cataract surgery. Advances in modern surgical techniques and intraocular lens designs have reduced its prevalence, and the rate of Nd:YAG laser capsulotomy varies widely from less than 5% to 54% depending on reports 1). Nevertheless, it still imposes a significant burden on patients and healthcare systems.
In children and infants, the incidence is remarkably high and the onset is early. The incidence of posterior capsule opacification in children can reach up to 100%, and early management of associated amblyopia risk is essential.
QMy vision has decreased some time after cataract surgery. Has the cataract recurred?
A
Cataracts themselves do not recur. The removed lens opacity does not return; posterior capsule opacification is one of the most likely causes. If blurring or vision loss occurs months to years after surgery, posterior capsule opacification should be suspected, and it is important to see an ophthalmologist.
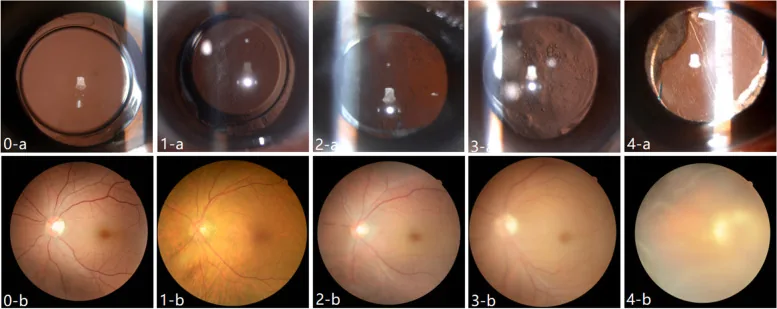
Zhou Y, et al. Objective quantification of posterior capsule opacification after cataract surgery with swept-source optical coherence tomography. BMC Ophthalmol. 2023. Figure 1. PMCID: PMC10324270. License: CC BY.
The upper row shows slit-lamp retroillumination images of posterior capsule opacification behind the intraocular lens, with progressively worsening posterior capsule opacification. The lower row shows decreasing fundus visibility as opacification progresses, confirming clinical findings of blurring and vision loss.
Many patients present months to years after an uncomplicated cataract surgery. Visual dysfunction progresses in the order of “decreased contrast sensitivity under glare conditions → decreased contrast sensitivity → decreased visual acuity,” so early evaluation of contrast sensitivity is important. Typical complaints are as follows.
Blurred vision and decreased visual acuity: Occurs when Elschnig pearls extend into the pupillary area. If there is a complaint of blurring but no decrease in visual acuity, measuring contrast sensitivity can detect a decrease.
Glare and light sensitivity: Caused by light scattering. In eyes with multifocal IOLs, even mild posterior capsule opacification has a greater impact than in eyes with monofocal IOLs.
Halos around lights
Difficulty reading and decreased contrast sensitivity: Early signs.
Pathophysiology: Lens epithelial cells transform into myofibroblast-like cells and produce extracellular matrix mainly composed of collagen. It spreads from the area where the anterior and posterior capsules adhere onto the posterior capsule.
Impact on symptoms: Visual impairment is relatively mild due to backward scattering. In severe cases, it can cause decreased contrast sensitivity and shrinkage of the anterior capsulotomy opening (anterior capsule contraction).
Pearl-Type Posterior Capsule Opacification (Elschnig Pearl Type)
Retroillumination findings: Small granular proliferations (Elschnig pearls) with relatively clear borders. They scatter light anteriorly, causing severe visual impairment.
Pathology: Caused by incomplete differentiation of lens epithelial cells lining the lens equator into lens fibers. Swollen and opacified bladder cells (Wedl cells) accumulate on the posterior capsule.
Impact on symptoms: Accumulation on the visual axis causes significant vision loss. If layered Elschnig pearls are present, vision loss is often already present.
Soemmerring ring: Caused by incomplete differentiation of lens epithelial cells into lens fibers. Years after surgery, the area surrounded by the anterior and posterior capsules in the periphery becomes donut-shaped and swollen. It rarely causes clinical problems. If it dislocates into the pupillary area due to zonular weakness or trauma, it can cause serious complications such as secondary glaucoma and corneal edema.
Liquefied after-cataract: A cloudy fluid accumulates between the IOL and the posterior capsule. It can be diagnosed by oblique illumination with a slit lamp. Elschnig pearls are often also present.
Elschnig pearls show dynamic changes, appearing and disappearing. It has been reported that formation and disappearance can occur within one week, and even in the same patient, different morphological patterns can be seen between the right and left eyes. Cases have been reported where pearls on the visual axis regressed spontaneously, improving vision. Proposed mechanisms of spontaneous regression include apoptosis, shedding into the vitreous cavity, and phagocytosis by macrophages.
In cataract surgery, a part of the anterior capsule is incised (continuous curvilinear capsulorhexis: CCC), the opacified lens tissue is removed, and an IOL is implanted. Posterior capsule opacification occurs due to proliferation, migration, and differentiation of residual lens epithelial cells on the anterior capsule.
Fibrosis may begin early after surgery, but usually opacification becomes severe after a long postoperative period. Involved cytokines and growth factors include TGF-β, FGF-2, hepatocyte growth factor (HGF), and matrix metalloproteinases (MMPs).
The diagnosis of posterior capsule opacification is based on medical history and slit-lamp examination. The diagnostic procedure is as follows.
Observation without dilation: If posterior capsule opacification is suspected, proceed to dilation.
Slit-lamp examination under dilation: Evaluate the type and degree of opacity by retroillumination of the posterior capsule. Elschnig pearls can be identified as well-defined small granular proliferations, and fibrosis as poorly defined multiple folds.
Retroillumination: Fibrous PCO is diagnosed by oblique illumination. Elschnig pearls are transparent and may be missed on routine observation.
Check fundus visibility with a 90D lens, etc.: Used to determine the indication for posterior capsulotomy.
Judgment based solely on visual acuity may be difficult. If there is a complaint of blurring but no decrease in visual acuity, measure contrast sensitivity. Since contrast sensitivity under glare, contrast sensitivity, and visual acuity are impaired in that order, evaluation of contrast sensitivity is important for early posterior capsule opacification.
After excluding other causes of vision loss (macular disease, optic nerve disease), determine the indication for posterior capsulotomy.
Indications for Nd:YAG laser posterior capsulotomy are as follows1):
When visual dysfunction due to PCO has decreased to a level that does not meet the patient’s functional needs
When fundus visualization is difficult and interferes with management of posterior segment disease
Prophylactic posterior capsulotomy is not performed
Perform after inflammation has subsided and the IOL is stable
QIs special equipment necessary for diagnosing posterior capsule opacification?
A
Basic diagnosis is possible with a slit lamp microscope and retroillumination. After dilation, retroillumination of the posterior capsule allows easy differentiation between Elschnig pearls and fibrosis. Fundus visibility with a 90D lens is also helpful. Elschnig pearls are transparent, so they may be missed with normal observation without retroillumination.
This is the first-line treatment for posterior capsule opacification affecting visual function. It is a non-invasive, rapid, and effective treatment, and surgical posterior capsulotomy is rarely performed.
Preoperative preparation: To prevent intraocular pressure elevation, instill apraclonidine hydrochloride eye drops 1 hour before and immediately after the procedure. Perform dilation before the procedure.
Incision method:
Method
Characteristics
Cruciate incision
Posterior capsule fragments are less likely to float; fewer laser shots required. Pits or cracks may occur near the visual axis.
Circular incision
Avoids the visual axis, providing higher safety. May cause floaters or inflammation due to posterior capsule fragments.
Fibrous opacification: Since the posterior capsule is hardened, increase laser power or use burst mode. Make radial incisions (usually 4 sites) in the opacified anterior capsulotomy edge to release capsular contraction.
Elschnig pearls: Irradiate to split the posterior capsule in a cruciate pattern.
Liquefied after-cataract: Only a small opening is made in the posterior capsule, allowing the liquefied material to diffuse into the vitreous.
Incision window size: Aim for a diameter of 4–5 mm or larger, exceeding the pupillary area.
Precautions for eyes with multifocal IOL: Even if slit-lamp examination appears normal, fine Elschnig pearls may be detected by retroillumination. Set the posterior capsulotomy window larger. Since PCO has a greater functional impact under low-contrast and glare conditions, earlier posterior capsulotomy may be indicated than usual 1).
Cases with strong astigmatism or irregular astigmatism: Making the posterior capsulotomy slightly smaller can maximize visual function and satisfaction through the pinhole effect.
In young children, Nd:YAG laser posterior capsulotomy cannot be performed safely; therefore, pars plana vitrectomy and capsulectomy are performed for visual axis opacification due to after-cataract. Early intervention is particularly important to prevent associated amblyopia.
In standard phacoemulsification, residual lens epithelial cells on the anterior capsule are activated postoperatively. These lens epithelial cells cause the following three phenomena, leading to posterior capsule opacification.
Proliferation: Residual lens epithelial cells continue to divide on the posterior capsule.
Migration: Proliferated lens epithelial cells migrate to the visual axis of the posterior capsule.
Differentiation: Lens epithelial cells undergo normal or abnormal differentiation, transforming into fibroblast-like cells (fibrous type) or lens fiber-like cells (pearl type).
In fibrous PCO, lens epithelial cells undergo epithelial-mesenchymal transition (EMT) into myofibroblastic cells and produce extracellular matrix (ECM) such as collagen. In pearl-type PCO, residual lens epithelial cells incompletely differentiate into lens fibers and accumulate on the posterior capsule as bladder cells (Wedl cells).
IOLs with a square-edge optic design have a lower rate of PCO compared to IOLs with rounded edges 1). A continuous curvilinear capsulorhexis slightly smaller than the IOL optic diameter creates a “shrink-wrap effect” where the anterior capsule edge rides onto the IOL surface, isolating the optic from the capsular aqueous humor and suppressing PCO development 1). When the anterior capsulotomy completely covers the entire optic, the PCO rate is lower 1).
Regarding IOL material, a 2013 meta-analysis (9 RCTs and multiple longitudinal studies) showed that hydrophobic sharp-edge IOLs have lower PCO rates and Nd:YAG capsulotomy rates compared to hydrophilic sharp-edge IOLs 1). However, a 12-year follow-up RCT suggested that the protective effect of sharp-edge hydrophobic lenses may only “delay” PCO onset 1).
Effect of anterior capsule polishing: Anterior capsule polishing shows inconsistent effects on PCO development. Some reports indicate that it may prevent tight adhesion between the posterior capsule and the sharp edge around the IOL optic, potentially promoting PCO and increasing the early need for Nd:YAG laser 1).
7. Latest research and future perspectives (research-stage reports)
Antimetabolites, anti-inflammatory agents, hypotonic drugs, and immunological preparations are being studied with the aim of removing residual lens epithelial cells or suppressing their regeneration without causing toxic side effects on surrounding intraocular tissues.
Two studies using immunotoxin (MDX-A) have observed a reduction in the rate of posterior capsule opacification, but there is still no definitive in vivo evidence that other drugs have a significant effect on the development of posterior capsule opacification. Techniques such as the “aqueous flush” at the end of surgery, which selectively damages lens epithelial cells, are also being explored.
Accommodating IOLs depend on the function of a flexible and intact posterior capsule, so prevention of posterior capsule opacification is a particularly important issue for these devices. Since opacification of the posterior capsule impairs accommodative function, the development of more aggressive preventive measures for posterior capsule opacification is required.
Miller KM, Oetting TA, Tweeten JP, Carter K, Lee BS, Lin S, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID:34780842.
Zhang Z, Jiang H, Zhou H, Zhou F. Comparative efficacy between trifocal and bifocal intraocular lens among patients undergoing cataract surgery: a systematic review and meta-analysis. Front Med (Lausanne). 2021;8:647268. doi:10.3389/fmed.2021.647268. PMID:34660614; PMCID:PMC8514957.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.