Traumatic cataract is lens opacification caused by trauma. It is more common in younger individuals compared to age-related cataract. When unilateral cataract is found in a young patient without underlying disease, traumatic cataract should be suspected first. The lifetime prevalence of ocular trauma in the general population is about 14%, with a higher incidence in children and young males. Of ocular trauma cases, 27–65% develop cataract, and most require surgery due to significant visual impairment 3).
Traumatic cataract is often accompanied by damage to other ocular tissues and frequently occurs in younger age groups, posing a significant public health burden. Even in the absence of cataract that severely affects visual function, zonular damage may cause lens subluxation, sometimes requiring surgical intervention.
Mechanism of Cataract Formation
Rapid opacification: Rupture of the lens capsule allows aqueous humor to enter the lens fibers.
Delayed opacification: Even without capsular rupture, trauma can damage lens fibers, leading to cataract formation months to years later.
Typical appearance: Rosette-shaped or stellate opacities.
Characteristics of Traumatic Cataract
Commonly affected: Children and young males.
Associated ocular injuries: Iris damage, zonular damage, vitreous prolapse, etc.
Urgency: Capsular rupture or elevated intraocular pressure requires emergency extraction.
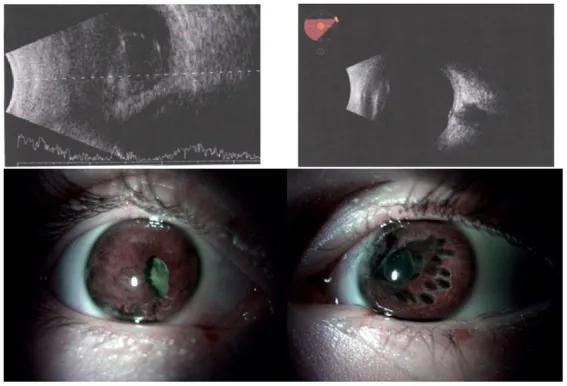
Nowomiejska K, et al. Case report: Bilateral eye injuries in members of one family due to a cluster munition in Ukraine. Front Med (Lausanne). 2023. Figure 3. PMCID: PMC10232851. License: CC BY.
The upper row shows preoperative B-mode ultrasound images (left: retinal detachment of the right eye, right: traumatic cataract of the left eye), and the lower row shows postoperative anterior segment images (A: right eye, B: left eye with iris cauterization for pupil centration). These correspond to the traumatic cataract discussed in the section “2. Main Symptoms and Clinical Findings.”
Preoperative visual acuity is useful for predicting the best-corrected postoperative visual acuity. As for intraocular pressure, asymmetrically low pressure suggests open globe injury or cyclodialysis cleft. Elevated intraocular pressure may reflect lens-induced glaucoma, hyphema, or angle recessionglaucoma.
Opacity location, anterior capsule rupture, subluxation, Vossius ring
Vossius ring: When blunt force presses the iris against the lens, iris pigment deposits in a ring shape on the anterior capsule surface corresponding to the pupillary margin. This is a characteristic finding of blunt trauma and serves as evidence of trauma to the lens capsule.
Size of the injuring object and opacity pattern:
Objects that enter the orbit (e.g., badminton shuttlecock): Posterior subcapsular opacity may occur immediately after injury.
Objects that do not fit into the orbit (softball, baseball, etc.): Posterior subcapsular opacity often followed by anterior subcapsular opacity.
Diagnostic System
The Birmingham Eye Trauma Terminology (BETT) system is used to record trauma.
Imaging Tests
B-mode ultrasound: Evaluation of intraocular foreign bodies, retinal detachment, and vitreous opacity when the posterior segment is difficult to observe.
CT scan: Exclusion of intraocular and orbital foreign bodies and abnormal eye shape (foreign body search in perforating trauma).
Ultrasound biomicroscopy (UBM): Evaluation of the posterior capsule, lens position, angle, and zonular integrity.
QCan cataracts develop immediately after trauma or take time?
A
Yes. In perforating trauma, the lens capsule is damaged and aqueous humor enters, causing rapid opacification immediately after injury. Small wounds (e.g., from a needle) may result in localized anterior subcapsular opacity, but large wounds (e.g., from a cutter) lead to rapid spread of opacity. In blunt trauma, even without capsular rupture, metabolic disturbances and osmotic changes due to external force can cause gradual opacification over months to years after injury.
The diagnosis of traumatic cataract itself is straightforward, but it is important to determine that the cause is trauma. Cataract surgery for traumatic cataract is more likely to be a difficult case compared to routine cataract surgery, so thorough preoperative evaluation is essential.
History of trauma (patients may forget blunt trauma)
Integrity of the anterior capsule (presence of rupture)
Integrity of the zonules (dislocation, phacodonesis)
Intraocular pressure (presence and type of glaucoma)
X-ray/CT (search for foreign bodies in penetrating trauma)
General condition and indication for emergency surgery
As a differential diagnosis, if unilateral posterior synechiae, anterior capsule opacity, or localized cortical opacity is observed, traumatic cataract should be suspected.
Extraction of traumatic cataract is broadly divided into “primary extraction” immediately after open globe injury and “secondary extraction” several weeks to months after injury.
Primary repair of open globe injury is desirable within 24 hours, and the risk of endophthalmitis is significantly lower in the group repaired within 24 hours (OR 0.39, 95% CI 0.19-0.79)1).
Surgical indications are determined similarly to routine cataract.
Posterior synechiae (small pupil, pupil deviation): Inject viscoelastic and bluntly release synechiae with a needle. 360-degree release possible via bilateral side ports.
Anterior capsule fibrosis: If fibrosis crosses the planned capsulotomy site, cut the fibrotic part with scissors and proceed.
Zonular weakness/dehiscence: Set phaco machine to low irrigation and low aspiration, use capsule expander and CTR.
Assessment of anterior capsule integrity: Use trypan blue intraoperatively to identify anterior capsule tears and visualize the capsule even in white cataracts. If a capsular tear is suspected, perform hydrodissection gently and cautiously.
Routine follow-up is performed on postoperative day 1, week 1, and month 1. Complete the course of topical antibiotics and steroid eye drops. If complications occur, monitor more frequently and adjust steroids or administer intraocular pressure-lowering medications.
QHow is traumatic cataract surgery different from routine cataract surgery?
A
Traumatic cataract surgery is more challenging than routine cataract surgery. Many intraoperative difficulties are anticipated, such as possible anterior capsule rupture, lens instability due to zonular damage, difficulty in dilating the pupil due to posterior synechiae, anterior capsule fibrosis, and high risk of posterior capsule rupture. It is important to utilize auxiliary tools such as trypan blue, CTR, and Malyugin ring, and to carefully plan the surgery according to the cataract morphology and associated injuries. Adequate preparation of instruments preoperatively is also essential.
Children are disproportionately affected by ocular trauma and require special management.
Preoperative considerations
In children, the threshold for determining significant visual impact is lower than in adults. If there is opacity greater than 3 mm on the visual axis, removal should be considered; delay increases the risk of amblyopia, so primary removal as an emergency procedure is recommended.
In penetrating trauma, promptly remove the lens and insert an IOL if possible. In blunt trauma, perform surgery based on the progression of the cataract.
Intraoperative considerations
In children under 2 years of age, cataract extraction is often combined with pars plana vitrectomy. In this age group, IOL insertion is deferred and performed as a secondary procedure.
Young patients have a strong inflammatory response and risk of fibrinous uveitis, requiring aggressive perioperative steroid management.
QHow soon should a child's traumatic cataract be operated on?
A
In children, due to the risk of amblyopia, more aggressive early intervention is required than in adults. Opacities larger than 3 mm on the central visual axis are indications for extraction, and urgent primary extraction is recommended. Delay in surgery increases the risk of amblyopia and may lead to permanent vision loss. Postoperatively, active amblyopia treatment such as occlusion of the healthy eye is necessary.
Regarding the superiority of primary versus secondary extraction, conflicting data still exist and no consensus has been reached 4). A report indicates that primary repair of open globe injury within 24 hours is associated with reduced risk of endophthalmitis (OR 0.39), supporting early intervention 1).
For scleral-fixated IOLs, sutureless fixation such as the Yamane technique is also an option. In cases without capsular support, the fixation method is chosen based on associated injuries and surgeon experience 6).
McMaster D, Bapty J, Bush L, Serra G, Kempapidis T, McClellan SF, et al. Early versus Delayed Timing of Primary Repair after Open-Globe Injury: A Systematic Review and Meta-analysis. Ophthalmology. 2025;132(4):431-441. doi:10.1016/j.ophtha.2024.08.030. PMID:39218161.
Kuhn F, Maisiak R, Mann L, Mester V, Morris R, Witherspoon CD. The Ocular Trauma Score (OTS). Ophthalmology clinics of North America. 2002;15(2):163-5, vi. doi:10.1016/s0896-1549(02)00007-x. PMID:12229231.
Mehul A Shah, Shreya M Shah, Shashank B Shah, Chintan G Patel, Utsav A Patel. Morphology of traumatic cataract: does it play a role in final visual outcome?. BMJ Open. 2011;1(1):e000060. doi:10.1136/bmjopen-2011-000060.
Rumelt S, Rehany U. The influence of surgery and intraocular lens implantation timing on visual outcome in traumatic cataract. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2010;248(9):1293-7. doi:10.1007/s00417-010-1378-x. PMID:20585800.
Ram J, Verma N, Gupta N, Chaudhary M. Effect of penetrating and blunt ocular trauma on the outcome of traumatic cataract in children in northern India. The journal of trauma and acute care surgery. 2012;73(3):726-30. doi:10.1097/TA.0b013e31825eeac9. PMID:22929502.
Morikawa S, Okamoto F, Okamoto Y, Mitamura Y, Ishikawa H, Harimoto K, et al. Clinical characteristics and visual outcomes of work-related open globe injuries in Japanese patients. Scientific reports. 2020;10(1):1208. doi:10.1038/s41598-020-57568-9. PMID:31988287; PMCID:PMC6985116.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.