Biometry is a general term for measurement methods that apply mathematics to biology. In ophthalmology, it refers to precise measurement of ocular dimensions for intraocular lens (IOL) power calculation in cataract surgery.
The refractive power of the eye is mainly determined by the cornea, lens, ocular media, and axial length (AL). In cataract surgery, the cloudy natural lens is removed and replaced with an IOL, so accurate preoperative IOL power calculation is necessary to achieve the target postoperative refraction.
When Harold Ridley performed the first IOL implantation in 1949, the patient experienced a refractive surprise of about 20 D. Subsequently, in the late 1960s, IOL power estimation using the vergence formula was introduced, marking the starting point of modern calculation methods. In the 1970s, A-mode ultrasound biometry was established, and formulas have since become more refined.
QWhat is measured in biometry?
A
Axial length, corneal power (K value), anterior chamber depth (ACD), lens thickness (LT), and corneal diameter (white-to-white, WTW) are measured. From these parameters, the effective lens position (ELP) is predicted, and the required IOL power is calculated.
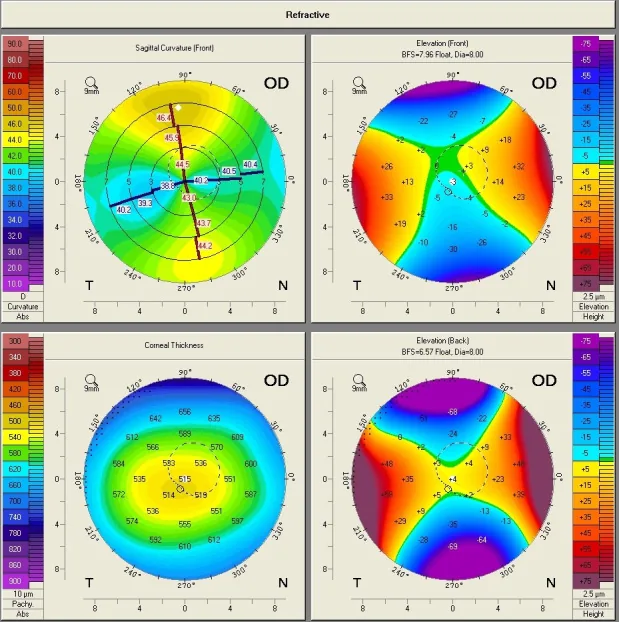
Lazăr AS, et al. Toric intraocular lens implantation - atypical cases. Rom J Ophthalmol. 2020. Figure 1. PMCID: PMC7739021. License: CC BY.
Sagittal curvature map from Scheimpflug corneal topography of the right eye, showing oblique astigmatism with an asymmetric bow-tie pattern. This corresponds to the corneal shape abnormality discussed in the section “2. Main symptoms and clinical findings”.
Biometry itself is a measurement method, not a disease. When measurement accuracy is insufficient, postoperative refractive surprise occurs, and patients complain of the following symptoms.
Hyperopic or myopic shift: The refractive outcome differs from the target, requiring spectacle correction.
Poor visual acuity: The greater the deviation from the target refraction, the lower the uncorrected visual acuity.
Reduced visual quality with multifocal intraocular lenses: Refractive error significantly affects patient satisfaction, especially with multifocal or extended depth of focus (EDF) intraocular lenses.
There are three main sources of postoperative refractive error.
Axial length error
Largest source of error: Axial length is the most important parameter, changing intraocular lens power by approximately 2.5 to 3 times.
Compression error: Contact A-scan can underestimate axial length due to corneal compression.
Overestimation in long eyes: Optical biometry applies a uniform refractive index to the entire eye, leading to overestimation in eyes with axial length >25 mm.
Corneal power error
Second source of error: A 1 D error in K value is reflected almost 1:1 in intraocular lens power error.
Measurement range issue: The keratometer measures a 3.2 mm diameter area, which may differ from the actual refractive power of the central cornea.
Post-refractive surgery eyes: Changes in the anterior-posterior curvature ratio lead to overestimation of corneal refractive power.
ELP Prediction Error
Effective lens position prediction error: It is difficult to accurately predict preoperatively where the intraocular lens will settle within the capsular bag.
Formula dependence: The accuracy of ELP prediction is the main cause of differences among generations of calculation formulas.
The ESCRS guidelines emphasize the accuracy of preoperative measurements, selection of appropriate formulas, and prediction of intraocular lens position as key points for reducing refractive error. Although measurement accuracy of axial length and corneal curvature has improved with advances in biometry, the accuracy of intraocular lens position prediction largely depends on the formula used1).
Risk factors that increase postoperative refractive error are listed below.
Short eye (AL <22 mm) or long eye (AL ≥26 mm): Calculation errors tend to be larger at the extremes of axial length. Normal eyes have AL of 22–25 mm, and the average anterior chamber depth of emmetropic eyes is 3–4 mm1).
Post-refractive surgery eyes: After LASIK, PRK, or RK, corneal shape changes, leading to systematic errors with conventional calculation methods.
Pediatric eyes: Because axial length is short and growth changes are large, applying adult formulas directly tends to cause errors2).
Mature cataract: The more severe the opacity, the lower the signal-to-noise ratio of optical measurements, and measurement may become impossible.
Macular pathology: Double peaks appear in about 35% of eyes with epiretinal membrane and about 20% with macular edema, requiring manual confirmation of measurements.
Silicone oil-filled eyes: Because the speed of sound in silicone oil differs from that in vitreous, special correction is needed for ultrasound methods.
QWhat to do when measurement with an optical biometer is not possible?
A
In cases of dense cataract or poor fixation, optical measurement may be difficult. In such cases, consider ultrasound biometry such as immersion A-scan 1). With contact methods, be cautious of shortening errors due to corneal compression.
Optical biometry is a non-contact measurement method using partial coherence interferometry (PCI) and has been the standard technique since the early device (IOL Master). Compared to contact A-mode ultrasound, it avoids axial length shortening due to corneal compression and has less operator dependence 3). Newer swept-source OCT can measure more cataractous eyes than conventional PCI 3).
The AAO Cataract PPP states that optical biometry measures the “refractive axial length” even when the macula is located on the sloping wall of a posterior staphyloma, and is therefore more accurate than standard A-mode ultrasound. It is also considered easier to use in eyes with intraocular silicone oil3).
A limitation of optical biometry is the application of a uniform refractive index to all eyes. In highly myopic eyes, due to the volume ratio of vitreous gel, the true axial length may be overestimated, leading to underestimation of IOL power with standard formulas. For eyes with axial length >25 mm, the Wang-Koch adjustment can be applied (but not needed for new-generation formulas such as Barrett Universal II or Hill-RBF) 3).
A-mode ultrasound uses mechanical waves and measures the time for a pulse to travel from the cornea to the retina. Sound velocity varies by medium (approximately 1641 m/s in lens and cornea, 1532 m/s in aqueous and vitreous), with an average of 1555 m/s in normal phakic eyes. The contact (applanation) method tends to artificially shorten axial length due to corneal compression, and measurement accuracy heavily depends on operator skill 3). The immersion method avoids compression error because the probe does not touch the cornea directly, but alignment control is difficult.
Corneal refractive power can be measured using manual keratometers, automated keratometers, computer videokeratography, Scheimpflug cameras (e.g., Pentacam), and anterior segment OCT3).
Standard keratometers assume the central cornea is a perfect sphere and estimate the posterior curvature from the anterior curvature (fixed anterior-posterior curvature ratio). This assumption does not hold in eyes after refractive surgery. In normal eyes, the average anterior corneal curvature radius is 7.5 mm (approximately 44.44 D), and the posterior radius is on average 1.2 mm smaller than the anterior.
Intraocular lens power calculation formulas are broadly classified into theoretical formulas, regression formulas, and mixed formulas, and are categorized by “generation.”
Currently, the most important variable is the prediction of the effective lens position (ELP), and the core of the generational evolution of each formula lies in improving the accuracy of ELP prediction.
The variables of each major formula are shown below. In addition to axial length and corneal power, there are differences in the additional variables used by each formula3).
Fusion of theoretical optics and regression analysis
The SRK formula (Sanders, Retzlaff, Kraff) is no longer recommended, but it is useful for understanding the relationship between variables (P = A − 0.9K − 2.5AL).
In Japan, the third-generation SRK/T formula is widely used, but it is advisable to compare multiple calculation results depending on axial length and anterior segment morphology. About 15% of patients seeking cataract surgery have eyes with disproportionate axial length and corneal power.
New-generation formulas (Barrett Universal II, Kane, Hill-RBF, etc.) combine theoretical optics, regression, and AI-based methods, and are being developed to improve accuracy even in short and long eyes, where conventional formulas had larger errors 4).
Relying solely on a single older-generation formula tends to increase refractive errors at the extremes of axial length. Comparing multiple formulas and selecting based on patient characteristics is important 4, 6).
The differences in mean absolute error (MAE) among new-generation formulas are often small 6). However, accuracy varies depending on the axial length range, so consider the following selection.
Short eyes (≤22 mm)
Hoffer Q and Holladay 2 are representative formulas that have been compared for short eyes.
ACD < 2.5 mm: ELP prediction errors tend to be larger, so compare multiple formulas 6).
Long eyes (≥24.5 mm)
24.5–26.0 mm: Compare results from third-generation and new-generation formulas.
≥26.0 mm: Pay attention to systematic errors among formulas for long eyes. Consider Wang-Koch axial length adjustment if necessary 6).
New-generation formulas (Olsen, EVO, Kane, Hill-RBF, Barrett II) have been evaluated across a wide range of axial lengths6).
The lens constants (A-constants) provided by intraocular lens manufacturers are only recommended values, and their consistency with the biometry method actually used is not guaranteed. It is beneficial to optimize constants based on the surgeon’s actual postoperative refractive outcomes or to utilize an online database (e.g., ULIB: User Group for Laser Interference Biometry) that aggregates data from multiple surgeons3).
When using an optical biometer, use intraocular lens constants dedicated to optical biometry. When using the IOLMaster, adopt measurements with a signal-to-noise ratio (SNR) ≥5.
Consider toric intraocular lenses when corneal astigmatism measured by keratometer is ≥2D for with-the-rule astigmatism or ≥1.5D for against-the-rule astigmatism. A 2016 systematic review and meta-analysis showed that toric intraocular lenses, including when combined with corneal relaxing incisions, result in less residual astigmatism than non-toric intraocular lenses3).
For calculation, it is recommended to use the manufacturer’s online calculator or the Haigis-T formula or Barrett Toric formula built into the optical biometer. These can directly import measurement values, reducing the risk of input errors. Preoperative corneal astigmatism ≥1D is present in about one-third of cataract surgery patients, indicating a large potential indication for toric intraocular lenses.
Major toric formulas include the Barrett Toric formula (empirically considers posterior corneal astigmatism), the Kane Toric formula (combined algorithm of AI, regression, and theoretical optics), and the EVO 2.0 Toric formula (integrates theoretical posterior corneal astigmatism and thick lens model). The Kane Toric formula has been reported to have a significantly lower mean absolute prediction error compared to other formulas.
Care must be taken regarding axis misalignment of toric intraocular lenses. Each degree of misalignment reduces the astigmatic correction effect by approximately 3%, and a 30-degree misalignment eliminates the correction effect.
QWhy is intraocular lens calculation difficult in cataract surgery for eyes that have undergone refractive surgery?
A
Refractive surgery (LASIK, PRK, RK) changes the curvature ratio of the anterior and posterior corneal surfaces. Since keratometers estimate the posterior curvature only from the anterior curvature, they overestimate corneal power in post-surgical eyes. Additionally, many IOL power formulas predict ELP from axial length and corneal power, but this relationship changes after refractive surgery, leading to errors in the formulas (see Management of Post-Refractive Surgery Eyes).
The only variable in this formula that cannot be measured preoperatively is ELP, and subsequent formulas (Holladay, Hoffer Q, SRK/T, Haigis, etc.) aim to improve the accuracy of ELP estimation.
Aphakic eye: The ultrasound velocity becomes 1532 m/s, and the two lens spikes disappear and are replaced by a single spike. For sulcus fixation, subtract 0.25 mm from the calculated ACD value.
Pseudophakic eye: The ultrasound velocity within the IOL depends on the lens material (PMMA: correction factor +0.45, silicone: −0.56 or −0.41, acrylic: +0.30). Optical biometry is recommended for remeasuring axial length in pseudophakic eyes.
After posterior vitrectomy or silicone oil-filled eyes: The two most common silicone oils have different sound velocities (1050 m/s and 980 m/s). Optical measurement is more accurate than ultrasound, and since intraocular silicone acts as a minus lens when implanting a biconvex IOL, the IOL power needs to be adjusted by 3 to 5 D.
Three main types of errors occur in eyes after refractive surgery.
Instrument error: The keratometer measurement zone (diameter 3.2 mm) does not accurately reflect the effective central corneal power zone. The error increases as the cornea becomes flatter.
Refractive index error: In PRK, LASIK, LASEK, and RK, the anterior-posterior curvature ratio changes, potentially overestimating corneal power by approximately 1 D for every 7 D of refractive correction.
Formula error: Most formulas predict ELP from axial length and corneal power, but they do not account for the fact that refractive surgery changes only corneal shape without proportionally altering anterior chamber dimensions.
Methods to obtain true corneal power after refractive surgery
The applicability of each method after LVC and RK is shown below.
Method
After LVC
After RK
Clinical history method
○
×
Contact lens overrefraction method
○
○
Central ring topography method
×
○
Clinical history method: This method subtracts the refractive change before and after surgery from the preoperative K value. Preoperative data is required, and it is unsuitable for RK (because the cornea flattens over time).
Contact lens overrefraction method: The corneal power is back-calculated from the base curve and power of the contact lens and the overrefraction. It can be used after both LVC and RK, but accuracy decreases in cases of low vision due to advanced cataract.
Central ring topography method (Awwad method): This method averages the K values in the central 3.0 mm zone and is useful for post-RK eyes.
Topography-based regression formulas (Koch-Wang formula, Shammas formula): These estimate the true corneal power from the central K value after LASIK. They are unsuitable for RK.
Direct measurement devices for the anterior and posterior corneal surfaces include Pentacam (rotating Scheimpflug camera, calculates TrueNetPower map and Holladay Report equivalent K values, alternative when clinical history data is unavailable), anterior segment OCT (direct measurement of anterior and posterior corneal power, can be used with ray-tracing software OKULIX), and Orbscan (slit scanning + Placido disc, caution for posterior surface measurement artifacts due to corneal opacity)7).
Dedicated intraocular lens calculation formulas after refractive surgery
Double-K method: This method uses the postoperative K value for vergence calculation and the preoperative K value (or its estimate) for ELP prediction. Double-K versions of SRK/T, Hoffer Q, and Holladay II are available and applicable to both LVC and RK7).
Barrett True-K formula: Can be used regardless of the availability of historical data. It is considered more accurate than many other formulas (e.g., Haigis-L, Masket). It was updated in 2015 to also cover post-hyperopic LASIK and RK6).
Haigis-L formula: Standardly installed in IOLMaster. No preoperative data required, but it is for post-LVC only and unsuitable for RK6).
Masket formula: Corrects the IOL power obtained from standard formulas by the induced refractive change from refractive surgery7).
Koch-Wang nomogram adjustment: Adjusts the IOL power calculated by SRK/T, Hoffer Q, and Holladay 1 based on separate nomograms for myopic and hyperopic corrections7).
ASCRS Post-LVC Calculator: Calculates results from multiple dedicated formulas simultaneously and presents the mean, median, maximum, and minimum values. Input items can be selected based on the availability of preoperative data, so it is widely recommended in clinical practice6)7).
Ray tracing method: Improves accuracy by using corneal anterior and posterior K values from anterior segment OCT7).
Even with methods that do not rely on historical data, 30–68% of cases achieve a target spherical equivalent within ±0.5 D, and methods requiring historical data are no longer the gold standard 6). Combining multiple methods yields the highest accuracy, with reported MedAE of 0.31–0.35 D and 66–68% within ±0.5 D 7).
The predictive accuracy by prior surgery type is as follows 7):
For eyes after radial keratotomy (RK), the ASCRS post-RK IOL calculator is useful. The clinical history method is often inaccurate in RK because of progressive central corneal flattening (hyperopic drift) 3). In post-RK eyes, the following points require special attention 7):
Using IOLMaster K values + Haigis formula with a target refraction of −1.00 D showed 73% within ±0.50 D and 88% within ±1.00 D.
A slightly myopic target refraction (−0.5 to −1.5 D) is recommended.
Care must be taken during cataract surgery to avoid interfering with RK incisions. The incision should be placed so that it does not cross RK scars, and in eyes with many incisions (more than 8), a scleral tunnel incision is preferred. Crossing RK incisions can lead to wound dehiscence and worsening of irregular astigmatism.
Transient flattening due to postoperative corneal edema may persist for several months. Early intraocular lens exchange should be avoided; additional correction should be considered after refractive stability is achieved.
In post-RK eyes, diurnal variation (hyperopia in the morning, myopia in the evening) may persist, so it is desirable to perform multiple refraction measurements at different times of the day.
Zeng et al. (2022) reported two patients who underwent PRK or LASIK after RK 5). In a case with increased anterior-to-posterior corneal curvature radius ratio (B/F ratio) (Case 1, RK+PRK), Barrett True-K (no history, post-RK) was most accurate (difference from actual IOL within 1D). In a case with decreased B/F ratio (Case 2, RK+LASIK), Shammas, Haigis-L, and Barrett True-K (no history, post-LASIK/PRK) showed good accuracy.
Based on these findings, Zeng et al. suggested that the B/F ratio (approximately 84% in normal eyes) may be an important indicator for selecting IOL calculation formulas in eyes after repeated refractive surgery 5).
Special Considerations for Intraocular Lens Power Calculation in Pediatric Eyes
In pediatric eyes, especially in infants, the short axial length amplifies errors. Additionally, an undercorrection strategy considering myopic shift due to eye growth is necessary 2).
Pediatric eyes differ fundamentally from adult eyes in the following aspects.
Myopic shift with eye growth: Myopia progresses over several years to decades after surgery. The most rapid growth occurs in the first 1–3 years of life, with reported myopic shifts of up to 8–17 D 2).
Difficulty in biometry: In young children, measurements often require general anesthesia, and errors are prone due to poor fixation and effects of anesthetic agents.
Balancing amblyopia risk: In pediatric IOL calculation, target refraction must consider both amblyopia prevention and future refractive status.
A systematic review by Rathod et al. (2025) revealed the following regarding pediatric IOL calculation 2).
Integrating multiple studies on IOL calculation accuracy, newer formulas (Barrett Universal II, Kane) showed higher accuracy compared to older formulas (SRK/T, etc.), especially in children aged ≥2 years with AL >21 mm. However, many reports suggest that Holladay 2, SRK/T, and Hoffer Q are useful in eyes with AL <22 mm, and no consensus has been reached 2).
AL and K measurements are the most influential parameters in children. Contact A-scan measures axial length shorter by an average of 0.24–0.32 mm due to corneal compression, so immersion A-scan is recommended when possible 2). IOL implantation in eyes with WTW diameter less than 9 mm is recommended to be avoided due to risks of posterior synechiae and secondary glaucoma2).
Representative proposed values for undercorrection strategy in children are shown below (Khokhar et al. protocol).
Under 6 months of age: 20% undercorrection of calculated power
At 1 year: 10% undercorrection
At 2 years: 5% undercorrection
At 5 years: 2% undercorrection
This setting anticipates myopic shift due to ocular growth, aiming to achieve near emmetropia in adulthood 2).
In a randomized study by Trivedi et al. on pediatric axial length measurement, contact measurements were on average 0.24–0.32 mm shorter than immersion measurements. Pediatric eyes have lower corneal and scleral rigidity, making them prone to compression error; immersion method is recommended 2).
QWhat is the best IOL calculation formula for pediatric cataract surgery?
A
Currently, there is no consensus. For children aged 2 years or older with AL >21 mm, Barrett Universal II and Kane formula are reported to have high accuracy, while for short eyes with AL <22 mm, many reports indicate that Holladay 2, SRK/T, and Hoffer Q are useful 2). Since individual differences in myopic shift are large, it is important to combine undercorrection strategy with long-term follow-up.
7. Latest Research and Future Perspectives (Research-stage Reports)
The Hill-RBF method (artificial intelligence-based pattern recognition) is an algorithm that estimates intraocular lens power from measured data and functions independently of anatomical parameters. In a study by Rastogi et al. (99 eyes, children aged 4–18 years), the Hill-RBF method showed predictive accuracy comparable to Barrett Universal II, SRK/T, Holladay 1, and Hoffer Q formulas, and is attracting attention as a promising option in pediatric ophthalmology 2).
Future AI-based formulas are expected to achieve higher accuracy than current formulas even in special eyes including pediatric cases by utilizing normal biometric data from each population 2).
Suzuki et al. (2025) retrospectively evaluated the accuracy of AI-driven intraocular lens calculation formulas in 80 eyes with extreme axial myopia (axial length ≥30.0 mm) 8). The Kane and Hill-RBF formulas showed significantly lower mean absolute error (MAE) compared to the conventional SRK/T formula. The percentage within ±0.5 D was 26.3% for SRK/T, 45.0% for Barrett Universal II, 55.0% for Hill-RBF, and 65.0% for Kane, demonstrating the superiority of AI-driven formulas. In the subgroup with axial length ≥32 mm, Hill-RBF had an MAE of 0.49 D and Kane had an MAE of 0.44 D, the best results 8).
An AI formula published in 2021 that uses machine learning to predict posterior corneal curvature radius and theoretical lens position. It is characterized by not requiring retraining for new intraocular lens models and is said to be applicable to toric IOLs and post-refractive surgery eyes. Accumulation of evidence is awaited.
This formula has a fully disclosed algorithm and integrates a device-independent toric calculation function 6). It holds a unique position in terms of algorithm transparency.
Ray tracing based on OCT data (Anterion-OKULIX) has been reported to have significantly lower arithmetic prediction error compared to the Barrett True K no-history formula in post-myopic LVC eyes (−0.13 D vs −0.32 D) 7). Since ray tracing directly uses the full corneal shape data, it is expected to have theoretical advantages in application to post-refractive surgery eyes.
In contrast to the conventional method that uses a uniform refractive index for the entire eye, “segmented axial length measurement” is being studied, which applies individual refractive indices to each segment (aqueous humor, lens, vitreous body). It is reported that for short eyes, the measurement is up to 0.29 mm larger, and for long eyes, 0.50 mm smaller, and significant improvements in MAE (mean absolute error) have been reported for many formulas except Haigis in the subgroups of long and short eyes. Currently, ARGOS (Suntec) implements the segmented method.
A “piggyback intraocular lens” approach has been proposed, where one intraocular lens is permanently placed in the capsular bag and the other is temporarily placed in the ciliary sulcus. The temporary intraocular lens can be removed after the patient reaches adulthood, allowing adjustment of postoperative refraction2). Further long-term data are needed for practical application.
Intraoperative wavefront aberrometry using devices such as the Optiwave refractive analyzer has been reported to achieve postoperative outcomes comparable to conventional biometry in adult routine cataract surgery. Its applicability to children is currently unclear, and further research is needed 2).
Rathod A, Khokhar S, Rani D. Pediatric IOL power calculation: Factors and considerations. Indian J Ophthalmol. 2025;73(3):312-319. doi:10.4103/ijo.ijo_1205_24.
American Academy of Ophthalmology. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. PMID: 34780842.
Chung J, Bu JJ, Afshari NA. Advancements in intraocular lens power calculation formulas. Curr Opin Ophthalmol. 2022;33(1):35-40. doi:10.1097/ICU.0000000000000822. PMID: 34854826.
Zeng Z, Ye X, Chen Q, Jia C, Zhang G. Intraocular lens power calculation after two different successive corneal refractive surgeries. American journal of ophthalmology case reports. 2022;26:101547. doi:10.1016/j.ajoc.2022.101547. PMID:35514797; PMCID:PMC9062137.
Wang L, Koch DD. Intraocular lens power calculations in eyes with previous corneal refractive surgery: review. In: ESCRS Guidelines on Prevention, Investigation, and Management of Post-operative Endophthalmitis and Cataract Surgery. 2024. (ESCRS Cataract Guideline, Section 6.3)
Suzuki Y, Kamoi K, Uramoto K, Ohno-Matsui K. Artificial intelligence driven intraocular lens power calculation in extreme axial myopia. Scientific reports. 2025;15(1):36921. doi:10.1038/s41598-025-20899-6. PMID:41125680; PMCID:PMC12546796.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.