Intraocular lens (IOL) dislocation is a general term for conditions in which the IOL inserted during cataract surgery shifts from its normal fixation position within the eye. The cumulative incidence of late in-the-bag IOL dislocation is reported to be 0.5–3%, most commonly occurring 6–12 years after cataract surgery 11).
IOL displacement is classified into the following three types:
Decentration/tilt: The optic is displaced from the visual axis due to fixation failure such as asymmetric insertion, without progression to dislocation.
Dislocation (subluxation): The IOL is displaced while still attached to part of the zonules or lens capsule, with IOL movement and risk of dislocation.
Drop: The IOL is completely detached from the zonules or capsule and falls onto the retina.
Dislocation is further classified into intracapsular dislocation (the IOL dislocates while still enclosed in the capsular bag) and extracapsular dislocation (the IOL dislocates after exiting the capsular bag). Intracapsular dislocation occurs as zonular rupture progresses and the IOL sinks posteriorly, with zonular degeneration due to exfoliation syndrome accounting for about 40% of cases.
Based on the time of onset, dislocation occurring within 3 months of IOL insertion is termed early dislocation, and that occurring after 3 months is termed late dislocation. Early dislocation is caused by intraoperative poor IOL fixation or rupture of the capsular bag or zonules. Late dislocation is mainly due to progressive zonular insufficiency and anterior capsule contraction.
According to statistics from Showa University Fujigaoka Hospital, the incidence of lens dislocation was 16 out of 1,639 eyes (approximately 1.0%), and associated factors were: after laser iridotomy 50.0%, history of ocular contusion 25.0%, exfoliation syndrome (XFS) 18.8%, and Marfan syndrome 12.5%.
QHow long after cataract surgery does IOL dislocation occur?
A
Early dislocation within 3 months after surgery often results from surgical manipulation factors. On the other hand, late dislocation may develop several years to more than a decade after surgery due to progressive zonular insufficiency. Long-term follow-up is necessary when underlying factors such as exfoliation syndrome or retinitis pigmentosa are present.
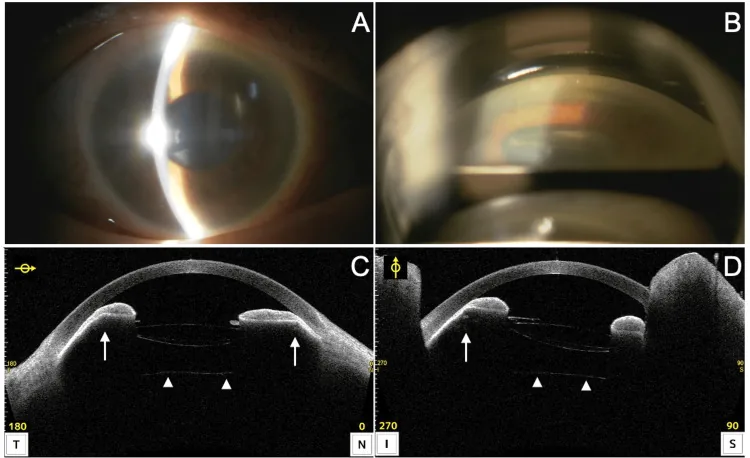
Murakami K, et al. A Case of Acute Angle Closure Secondary to Pupillary Block Caused by a Dislocated Intraocular Lens-Capsular Tension Ring Complex. Cureus. 2024. Figure 3. PMCID: PMC11617787. License: CC BY.
Slit-lamp examination shows corneal edema and shallow anterior chamber; gonioscopy reveals obscured angle structures. Anterior segment OCT demonstrates anterior displacement of the IOL complex and iris indentation, indicating clinical findings of IOL dislocation.
In mild cases, IOL displacement is observed within the pupillary area. In severe cases, the IOL is observed outside the pupillary area. Its position often changes with postural changes.
IOL oscillation can be observed with eye movements or blinking under non-mydriatic conditions, which is useful for diagnosing mild dislocation. Even if the inferior zonules are broken, if the superior zonules are attached, the IOL may appear in a normal position on slit-lamp examination in the sitting position. When the patient is supine, the IOL tilts and sinks posteriorly, so the supine position should be confirmed under an operating microscope before surgery.
In cases with significant vitreous liquefaction or in aphakic eyes, the IOL may fall into the vitreous cavity, presenting findings similar to aphakia (high hyperopia).
When the IOL is dislocated into the anterior chamber, the following serious complications may occur:
Pupillary blockglaucoma: The IOL occludes the pupil, causing a rapid increase in intraocular pressure6)
Uveitis and hyphema: Inflammation due to irritation of the iris
Sim et al. (2022) reported a case of sequential anterior IOL dislocation in both eyes of a 64-year-old woman with retinitis pigmentosa6). The right eye developed bullous keratopathy due to corneal endothelial damage, and the left eye developed pupillary blockglaucoma (IOP 50 mmHg); both required IOL explantation.
History of vitrectomy: Zonular damage during peripheral vitrectomy or loss of vitreous support.
High myopia: May be associated with zonular weakness. Vitreous liquefaction also contributes.
Chronic intraocular inflammation: In conditions such as uveitis, be aware of zonular weakening and late in-the-bag dislocation. 8)
Systemic and external factors
Trauma: Blunt trauma causes eyeball deformation and rupture of the zonules. This is the most common cause of lens dislocation when the cause is clear.
Marfan syndrome: A connective tissue disease caused by mutations in the FBN1 gene. About 60% of cases develop lens subluxation, often upward.
Atopic dermatitis: Repeated eye rubbing damages the zonules.
Homocystinuria: A congenital amino acid metabolism disorder. It causes bilateral lens subluxation (often downward).
Zonular weakness is problematic in conditions such as exfoliation syndrome, history of vitrectomy, and high myopia, increasing the risk of complications during cataract surgery and late IOL dislocation. 7, 8, 9)
The main mechanism of late dislocation is anterior capsule contraction (capsular phimosis). After continuous curvilinear capsulorhexis (CCC), lens epithelial cells at the capsulotomy edge proliferate and transform into myofibroblasts. When this contractile force overcomes the centrifugal force of the zonules, contraction of the capsulotomy opening progresses. The frequency and severity of anterior capsule contraction syndrome vary depending on the IOL type and ocular background. 10) Risk factors for anterior capsule contraction include small-diameter CCC, zonular weakness, exfoliation syndrome, retinitis pigmentosa, chronic intraocular inflammation, and high myopia. The shock of Nd:YAG laser posterior capsulotomy for posterior capsule opacification can also trigger subluxation.
QWhat is exfoliation syndrome? How is it related to IOL dislocation?
A
Exfoliation syndrome (pseudoexfoliation syndrome; PXF) is an age-related disease in which white exfoliative material deposits on the iris, lens surface, and angle. The zonules progressively weaken, making it the greatest risk factor for IOL in-the-bag dislocation after cataract surgery, accounting for about 40% of in-the-bag dislocations. It is often accompanied by poor pupil dilation and glaucoma.
For differentiation between dislocation and drop and for surgical planning, evaluation in the supine position under an operating microscope is essential. An IOL that appears within the pupillary area in the sitting position often tilts and sinks posteriorly in the supine position.
Even if the IOL can be confirmed with a slit-lamp microscope, in cases with significant vitreous liquefaction, the IOL may not be directly visible under the surgical microscope. Fundus examination is essential, and if the IOL falls into the vitreous cavity, it will show strong hyperopic shift.
For multifocal IOLs and toric IOLs, even very slight displacement can significantly degrade optical performance, so early surgical intervention should be considered.
Preoperative diagnosis requires determining whether the dislocation is intracapsular or extracapsular, how to lift the IOL onto the iris, the extent of vitrectomy, and the instruments needed for removal and fixation.
Visual loss due to posterior capsule opacification: The IOL position is usually normal. It improves with Nd:YAG laser posterior capsulotomy.
Visual impairment due to vitreous opacity: No abnormality in the anterior segment or IOL position; vitreous opacity is confirmed by fundus examination and B-mode ultrasound.
Mano et al. (2021) reported a case of IOL dislocation and elevated intraocular pressure in end-stage exfoliation syndrome, measuring the IOL tilt angle over time using swept-source OCT, which was 6.6°, 7.9°, and 8.7° at 1, 4, and 6 months postoperatively, respectively 4).
If the IOL subluxation is mild, has little effect on vision, and causes no damage to surrounding tissues, observation is an option. Cases with pseudophacodonesis but no inferior dislocation often remain asymptomatic. Visual correction with refractive methods and close monitoring are performed.
Depending on the degree of displacement, repositioning alone may be sufficient. Pupillary capture, capsular capture, anterior chamber dislocation of a loop, and early postoperative asymmetric fixation can be repositioned using a hook or spatula through a side port.
A 2018 network meta-analysis confirmed that iris fixation, transscleral fixation, and intrascleral fixation all show equivalent efficacy (AAO PPP). 7) It is recommended to reduce the IOL power for ciliary sulcus fixation by 0.5–1.0 D from the calculated in-the-bag value. 7) Note that ciliary sulcus fixation of a single-piece acrylic IOL is contraindicated due to risks of iris chafing, pigment dispersion, and IOL decentration. 7)
Intrascleral Fixation (Yamane Technique)
Principle: Create a scleral tunnel with a 30-gauge needle, pass the haptic of a 3-piece IOL through it, and form a flange by cauterization. No sutures or adhesives required. 12)
Advantages: Minimal conjunctival dissection, less invasive. Favorable for combined glaucoma surgery. 4)
Recommended IOL: IOLs with PVDF haptics (e.g., CT Lucia 602) offer superior durability.
Challenge: With 10-0 polypropylene, there is a risk of suture breakage at an average of 4 to 6.5 years.
Main complications: IOL redislocation, tilt, intraocular hemorrhage, retinal detachment, exposure/erosion/breakage of suture knots7)
Anterior chamber lens / Iris fixation
ACIOL: Flexible open-loop type. Assessment of anterior chamber depth and angle is essential. Some reports recommend avoiding it in patients under 50 years of age.
Iris suture fixation: Iris clip lens or McCannel suture technique. Be aware of the risk of corneal endothelial damage.
If a multi-piece IOL made of a less breakable material such as polyvinylidene fluoride (PVDF) is used, it is possible to refixate the dislocated IOL directly within the vitreous cavity to the sclera. In cases of repeated IOL redislocation or poor iris/scleral condition, exchange to an ACIOL may ultimately be chosen2).
Mano et al. (2021) performed simultaneous Yamane technique (flanged intrascleral fixation) and trabeculectomy in an 88-year-old woman with end-stage exfoliation syndrome (IOP 47 mmHg)4). IOL removal was performed through an inferior temporal L-shaped incision (at 8 o’clock), preserving the superior conjunctiva for trabeculectomy. At 6 months postoperatively, corrected visual acuity improved from 0.2 to 0.4, and IOP was 8 mmHg, indicating a favorable course.
QDoes every dislocated IOL require surgery?
A
Mild subluxation without significant visual impact or damage to surrounding tissues can be observed. Correct vision with refractive correction and monitor regularly. However, because progression is possible, patients should promptly see an ophthalmologist if symptoms change.
QCan a dislocated multifocal IOL be reused?
A
If the IOL is undamaged and the power is appropriate, reuse (repositioning) via scleral fixation is possible. Eom et al. (2022) used the cable tie method to fix a C-loop haptic multifocal IOL with four-point flange fixation and restored good distance and near visual acuity5). It is also more cost-effective than IOL exchange.
The mechanism of IOL dislocation is based on weakening or rupture of the zonules of Zinn. The zonules are fibers that suspend the lens capsule from the ciliary body, and the clinical presentation varies depending on the extent of rupture.
Partial rupture: Depending on the extent of rupture, lens (IOL) instability, iris tremulousness, and shallow anterior chamber occur.
Complete circumferential rupture: The IOL falls into the vitreous cavity or dislocates into the anterior chamber.
Zonular Insufficiency in Pseudoexfoliation Syndrome
In pseudoexfoliation syndrome, exfoliative material deposits on the iris, lens surface, angle, and ciliary body surface. This material accumulates directly on the zonules, leading to progressive fiber weakening with age. It is often accompanied by poor pupillary dilation, increasing the difficulty of cataract surgery.
Late Dislocation Due to Anterior Capsule Contraction
After continuous curvilinear capsulorhexis (CCC), lens epithelial cells at the capsulotomy edge proliferate and transdifferentiate into myofibroblasts. When the centripetal contractile force generated by these cells exceeds the centrifugal force of the zonules, capsular phimosis (contraction of the capsulotomy opening) occurs. Epithelial cell proliferation due to posterior capsule opacification increases the weight of the IOL and lens capsule, further increasing stress on the zonules. 8)9)
In patients with retinitis pigmentosa, the prevalence of IOL dislocation is reported to be 9–10% 6). Direct damage to the zonules by toxic substances from the degenerated retina is presumed. Another proposed mechanism is that disruption of the blood-ocular barrier increases cytokines in the aqueous humor, promoting proliferation of lens epithelial cells and accelerating anterior capsule contraction 6).
Marfan syndrome is an autosomal dominant connective tissue disorder caused by mutations in the FBN1 gene. In addition to skeletal (tall stature, arachnodactyly, scoliosis) and cardiovascular (aortic aneurysm, dissection) manifestations, approximately 60% of cases have ectopia lentis. Dislocation is often upward or upward-temporal. There is also a high risk of spherophakia, high myopia, retinal detachment, and glaucoma.
7. Latest Research and Future Prospects (Investigational Reports)
Scleral-fixated IOLs have reduced refractive predictability, with only about 50% of patients achieving within ±0.5 D compared to 72% for in-the-bag fixation. The Light Adjustable Lens (LAL) is an IOL whose power can be adjusted postoperatively by ultraviolet light exposure.
Ma et al. (2023) performed trocar-based intrascleral haptic fixation (ISHF) of an LAL in a 53-year-old woman with bilateral lens subluxation1). Postoperative power adjustment was performed targeting micro-monovision, achieving uncorrected visual acuity of 20/20 in both eyes. The application of LAL to scleral fixation is an approach that may overcome the refractive prediction error, the greatest weakness of ISHF.
Simplification of Technique via Trocar-Based Modification
Bever et al. (2021) reported a modification in which the IOL is intentionally dropped onto the retina and the haptic tip is directly grasped with a 27-gauge forceps and pulled out through the sclera3). This technique eliminates the need for manipulation at the iris plane and is safe and efficient for surgeons experienced in vitreoretinal surgery. In four eyes, all achieved lens stability and good centration.
Refixation of Multifocal IOLs Using the Cable Tie Technique
Eom et al. (2022) reported four-point flange intrascleral fixation of subluxated multifocal IOLs with C-loop and double C-loop haptics using the cable tie technique with 6-0 polypropylene 5). By forming a loop of the suture like a cable tie, secure fixation at the optic-haptic junction is achieved. Both cases achieved good IOL centration and distance and near visual acuity.
Chu Jian Ma, Craig C. Schallhorn, Jay M. Stewart, Julie M. Schallhorn. Modified intrascleral haptic fixation of the light adjustable lens in a case of spontaneous adult-onset bilateral lens subluxation. American Journal of Ophthalmology Case Reports. 2023;31:101864. doi:10.1016/j.ajoc.2023.101864.
Hoang J, Gutowski M, Altaweel M, Liu Y. Combined minimally invasive conjunctival surgery with lens repositioning for traumatic bleb leak with dislocated intraocular lens. Trauma case reports. 2023;48:100936. doi:10.1016/j.tcr.2023.100936. PMID:37810536; PMCID:PMC10551890.
Bever GJ, Liu Y, Stewart JM. Modified technique for trocar-based sutureless scleral fixation of intraocular lenses: A new approach to haptic externalization. American journal of ophthalmology case reports. 2021;23:101145. doi:10.1016/j.ajoc.2021.101145. PMID:34195478; PMCID:PMC8233194.
Mano Y, Mizobuchi K, Watanabe T, Watanabe A, Nakano T. Minimally invasive surgery for intraocular lens removal and intrascleral intraocular lens fixation with trabeculectomy in a patient with dislocated intraocular lens and elevated intraocular pressure. Case Rep Ophthalmol. 2021;12:538-542. doi:10.1159/000511593.
Eom Y, Lee YJ, Park SY, Choi Y, Kim JW, Kim SJ, et al. Cable tie technique for securing scleral fixation suture to intraocular lens. American journal of ophthalmology case reports. 2022;27:101646. doi:10.1016/j.ajoc.2022.101646. PMID:35813586; PMCID:PMC9263869.
Yee Chau Sim A, Meng Hsien Y, Seng Fai T, Mustapha M, Wan Abdul Halim WH.. Bilateral Sequential Spontaneous Anterior Dislocated Intraocular Lens in a Patient With Retinitis Pigmentosa. Cureus. 2022;14(7):e26986. doi:10.7759/cureus.26986. PMID:35989805; PMCID:PMC9385266.
Miller KM, Oetting TA, Tweeten JP, Carter K, Lee BS, Lin S, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID:34780842.
Hayashi K, Hirata A, Hayashi H. Possible predisposing factors for in-the-bag and out-of-the-bag intraocular lens dislocation and outcomes of intraocular lens exchange surgery. Ophthalmology. 2007;114(5):969-975. doi:10.1016/j.ophtha.2006.09.017.
Hartman M, Rauser M, Brucks M, Chalam KV. Evaluation of anterior capsular contraction syndrome after cataract surgery with commonly used intraocular lenses. Clinical ophthalmology (Auckland, N.Z.). 2018;12:1399-1403. doi:10.2147/OPTH.S172251. PMID:30122893; PMCID:PMC6087024.
Kristianslund O, Dalby M, Drolsum L. Late in-the-bag intraocular lens dislocation. J Cataract Refract Surg. 2021;47(7):942-954. PMID: 33750091. doi:10.1097/j.jcrs.0000000000000605.