
Pupillary Capture of Intraocular Lens (IOL Capture)
Key Points at a Glance
Section titled “Key Points at a Glance”1. What is pupillary capture of the intraocular lens?
Section titled “1. What is pupillary capture of the intraocular lens?”Pupillary capture refers to a condition in which part of the optic of an intraocular lens (IOL) that is not completely fixed within the capsular bag prolapses in front of the iris. It is more likely to occur after extracapsular fixation or suturing, but even with in-the-bag fixation, the portion not covered by the anterior capsule may protrude in front of the iris. It is known to occur more frequently when gas is injected during combined vitrectomy surgery. In addition, it tends to recur after IOL suturing, and is thought to be sometimes caused by reverse pupillary block.
In modern practice, since in-the-bag fixation has become standard, the overall frequency has been decreasing, but it remains a problem in cases with posterior capsule rupture or in aphakic eyes after sutured or scleral-fixated IOLs. The incidence of pupillary capture with scleral-sutured IOLs has been reported as 18 out of 495 eyes (3.6%), 6) and it has also been documented as a late complication in long-term follow-up studies of sutured IOLs inserted during vitrectomy. 1)
Note that intentional insertion of the IOL optic through a posterior continuous curvilinear capsulorhexis (posterior CCC) into the posterior capsule opening, known as “posterior optic capture,” is a deliberate technique to prevent posterior capsule opacification and is distinct from the accidental pupillary capture discussed in this article.
Association with UGH syndrome
Section titled “Association with UGH syndrome”When the IOL haptic directly contacts the iris or surrounding tissues due to extracapsular or asymmetric fixation, the haptic mechanically chafes the iris, releasing iris pigment. This pigment deposits in the trabecular meshwork, causing pigmentary glaucoma, and if iris damage is significant, it may be accompanied by iridocyclitis and hyphema. This series of conditions is called uveitis-glaucoma-hyphema (UGH) syndrome. Fixation of a one-piece acrylic IOL in the ciliary sulcus can cause transillumination defects, pigment dispersion, elevated intraocular pressure, recurrent hyphema, and inflammation; therefore, insertion into the ciliary sulcus is contraindicated. 7)
When combined with vitrectomy or after gas injection, it tends to occur early postoperatively (within days to weeks). After sutured or scleral-fixated IOLs, it may develop months to years after surgery and has a tendency to recur. In a study by Vote et al., it was reported as a late complication in long-term follow-up after vitrectomy with sutured IOL. 1)
2. Main symptoms and clinical findings
Section titled “2. Main symptoms and clinical findings”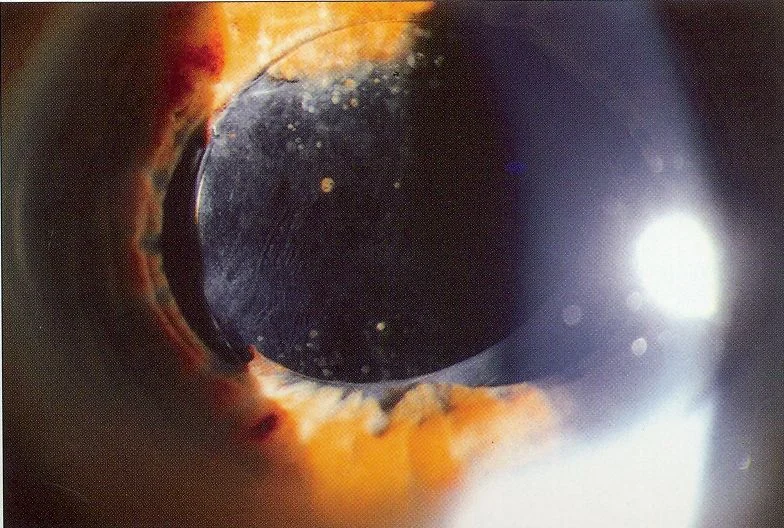
{kind=link}
Subjective Symptoms
Section titled “Subjective Symptoms”- Glare and photophobia from IOL edge: Characteristically occurs when the optic edge is exposed in the pupillary area. Direct impact on corrected visual acuity is usually minimal.
- Refractive error: Astigmatism or changes in spherical power due to IOL decentration are common.
- Elevated intraocular pressure: Pupillary block caused by the dislocated optic can increase intraocular pressure, presenting symptoms similar to acute angle-closure attack.
- Decreased visual acuity: Usually mild, but may occur with UGH syndrome or cystoid macular edema (CME). 6)
- Pupil deviation or irregular pupil: Pupil shape may change due to interaction between the IOL and iris.
Clinical Findings
Section titled “Clinical Findings”- Anterior dislocation of IOL optic: Easily observed under dilated pupil with slit-lamp microscopy. Part or all of the optic is seen anterior to the iris.
- Changes in anterior chamber depth: In cases of reverse pupillary block, the anterior chamber deepens and the iris bows posteriorly, a characteristic finding.
- Iris transillumination defects: Findings of iris chafing by IOL haptics. Confirmed as a sign of UGH syndrome.
- Pigment dispersion and anterior chamber pigmentation: Pigment deposition on the trabecular meshwork suggests UGH syndrome.
- Hyphema: May occur recurrently.
- Corneal edema: Occurs when IOL haptics contact the corneal endothelium.
Even if visual acuity is not significantly affected, treatment should be considered when photophobia due to the IOL edge is severe or when intraocular pressure elevation due to pupillary block is present. If the IOL haptic is in contact with the corneal endothelium, prompt repositioning is necessary; if left untreated, corneal endothelial damage may progress and eventually lead to bullous keratopathy.
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”The fundamental cause of pupillary capture is that the IOL is not completely fixed within the capsular bag. The following risk factors have been reported.
| Risk Factor | Mechanism |
|---|---|
| Extracapsular fixation / asymmetric fixation | IOL is not completely covered by the capsule |
| IOL ciliary sulcus suture | No capsular support, prone to recurrence |
| Intrascleral fixation (including Yamane technique) 8) | No capsular support, residual IOL movement |
| Simultaneous vitrectomy with gas tamponade | Expansile gas pushes the IOL forward |
| Post-vitrectomy 6) | Loss of vitreous support for IOL + flaccid iris |
| Young patients | High iris extensibility |
| Ciliary sulcus implantation of one-piece acrylic IOL 7) | Iris chafing due to sharp anterior edge (contraindicated) |
| Scleral suture placement less than 2 mm from the limbus 6) | IOL too close to the iris |
In a study by Kokame et al., recurrence was significantly lower in the group where the scleral suture position was standardized to 2 mm posterior to the limbus (p=0.025). 6)
Contrary to normal pupillary block, this is a condition where anterior chamber pressure exceeds posterior chamber pressure, and the pupillary margin adheres to the anterior surface of the IOL, acting as a valve. It presents characteristic findings of a deep anterior chamber and posterior bowing of the iris. When the IOL moves anterior to the iris, the flow of aqueous humor from the anterior chamber to the posterior chamber is blocked, further increasing posterior chamber pressure, creating a vicious cycle. Laser iridotomy (LI) is effective in resolving the pressure gradient between the anterior and posterior chambers. 2)
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”| Examination method | Evaluation content | Key points |
|---|---|---|
| Slit-lamp microscopy | Positional relationship between IOL optic and iris | Evaluate optic coverage under mydriasis. Also check for haptic prolapse into the anterior chamber. |
| Tonometry | Intraocular pressure elevation due to pupillary block | Emergency management for acute elevation |
| Anterior segment OCT | Objective assessment of anterior chamber depth, IOL position, and iris curvature | Useful for evaluating reverse pupillary block |
| Ultrasound biomicroscopy (UBM) | Positional relationship between IOL and ciliary body/sulcus | Confirmation of IOL position in sutured or intrascleral fixation |
| Corneal endothelial specular microscopy | Corneal endothelial cell density | Assessment of endothelial damage due to IOL haptic contact |
| Gonioscopy | Evaluation of pigment deposition and peripheral anterior synechiae | Used for evaluation of UGH syndrome |
Differential Diagnosis
Section titled “Differential Diagnosis”- IOL dislocation/subluxation: When the IOL is completely displaced and falls into the vitreous cavity, it is managed as a separate condition.
- UGH syndrome: This is a related complication of pupillary capture, but can occur without pupillary capture due to IOL contact alone.
- IOL decentration/tilt: The IOL is displaced within the capsular bag but does not prolapse in front of the iris.
- Acute angle-closure attack: Presents with elevated intraocular pressure, shallow anterior chamber, and fixed dilated pupil; after IOL surgery, differentiation from pupillary capture is important.
It is not essential if the diagnosis is clear on slit-lamp examination, but it is useful for evaluating reverse pupillary block (increased anterior chamber depth, posterior bowing of the iris) and for objective documentation of IOL position. Especially in recurrent cases, quantitative assessment of IOL position using anterior segment OCT or UBM helps determine treatment strategy.
5. Standard Treatment
Section titled “5. Standard Treatment”Treatment is selected stepwise according to the onset situation, presence of adhesions, and recurrence frequency.
Step 1: Conservative Repositioning (Acute onset, no adhesions)
Section titled “Step 1: Conservative Repositioning (Acute onset, no adhesions)”- After administration of mydriatics (1% tropicamide + 2.5% phenylephrine), place the patient in supine position → attempt spontaneous repositioning.
- Effective when the iris and IOL are not adherent.
- If pupillary block occurs due to anterior chamber IOL dislocation, use mydriatics (miotics are contraindicated).
Step 2: Surgical Repositioning (If spontaneous repositioning fails)
Section titled “Step 2: Surgical Repositioning (If spontaneous repositioning fails)”- Reposition the IOL optic behind the iris using a hook or spatula through a side port.
- The procedure is easy if the iris and capsule are not significantly adherent.
- Outpatient 30G needle paracentesis technique: under topical anesthesia, anterior chamber paracentesis is performed and viscoelastic material is injected to push the IOL posteriorly. Kokame et al. managed all 54 outpatient procedures for pupillary capture in 18 of 495 eyes (3.6%) without transfer to the operating room. 6)
Step 3: Prevention of recurrence (recurrent cases after sutured IOL)
Section titled “Step 3: Prevention of recurrence (recurrent cases after sutured IOL)”After IOL suturing or intrascleral fixation, the optic is not covered by the capsule, so pupillary capture tends to recur.
- Laser iridotomy (LI / iridectomy): Resolves the pressure difference between the anterior and posterior chambers when reverse pupillary block is involved. Although difficult to decide, it can be effective in some cases. 2)
- Suture technique (retention suture): If recurrence occurs even after LI, consider passing a suture to prevent the IOL from prolapsing anterior to the iris. Lin et al. reported a rectangular loop suture, and Kim et al. reported a tram-track suture technique. 3,4)
- Iris constriction or additional suturing: For repeated recurrences, reduce the pupil size or the passageway in front of the IOL to prevent optic prolapse. Suppression of recurrence using flanged polypropylene sutures has also been reported. 5)
Step 4: IOL exchange (irreducible or severe cases)
Section titled “Step 4: IOL exchange (irreducible or severe cases)”- Performed only when visual function is significantly impaired (highly invasive).
- If the iris and capsule are strongly adherent or if the IOL repeatedly dislocates into the anterior chamber, reduction alone is difficult and IOL exchange is necessary.
- If the haptic is in the anterior chamber and contacting the corneal endothelium, reposition as soon as possible.
- Fixation method during exchange: Ciliary sulcus fixation of a three-piece IOL and optic capture preserving the anterior capsulorhexis provide excellent stability. 7)
| Treatment | Indication | Notes |
|---|---|---|
| Mydriasis + supine position | Acute onset, no adhesions | First choice. Miotics are contraindicated |
| Hook/spatula repositioning | Cases where spontaneous repositioning is not possible | Performed via side port |
| 30G needle paracentesis6) | Outpatient repositioning | Under topical anesthesia, no operating room required |
| Laser iridotomy2) | Suspected reverse pupillary block | Resolve anterior-posterior chamber pressure difference |
| Suture fixation method3, 4) | Cases that recur after LI | Scleral fixation suture |
| Iris suturing and additional suturing5) | Recurrent repositioning failure | Adjust pupil size and passage |
| IOL exchange7) | Irreducible or severe cases | Only when visual function is significantly impaired |
Prevention
Section titled “Prevention”- Fixation position of scleral-sutured IOL: Fixation 2 mm posterior to the limbus significantly reduces recurrence (p=0.025).6)
- Optic capture during ciliary sulcus fixation: If the anterior capsulorhexis is preserved, engaging the optic into the CCC opening improves IOL stability.7)
- Do not insert single-piece acrylic IOL into the ciliary sulcus (risk of iris chafing and UGH syndrome).7)
Recurrence is common after sutured IOL or intrascleral fixation IOL. First, try laser iridotomy to relieve reverse pupillary block2). If recurrence persists, manage with suture tensioning method3,4) or additional suturing5) to prevent the IOL from moving anterior to the iris. In some cases, repositioning can be performed in the outpatient setting using a 30G needle paracentesis technique without transferring to the operating room.6)
6. Pathophysiology and detailed mechanism
Section titled “6. Pathophysiology and detailed mechanism”1. Physical instability due to poor IOL fixation
Section titled “1. Physical instability due to poor IOL fixation”When the IOL is not completely fixated within the capsular bag, eye movements, blinking, and postural changes cause the IOL to oscillate anteriorly and posteriorly. In extracapsular fixation, the haptics are in the ciliary sulcus and the optic is just behind the iris, resulting in insufficient coverage by the anterior capsule. A slight anterior displacement can cause the optic to prolapse beyond the iris.
2. Forward displacement by vitreous gas
Section titled “2. Forward displacement by vitreous gas”When gas is injected during concurrent vitrectomy, the expanding gas pushes the IOL forward, causing the optic to dislocate anterior to the iris beyond the pupillary plane. Although the IOL may reposition after gas absorption, recurrence is common in cases with insufficient capsular support.
3. Iris flaccidity after vitrectomy
Section titled “3. Iris flaccidity after vitrectomy”Removal of the vitreous eliminates vitreous support for the IOL, making it unstable. In the absence of the lens capsule, iris flaccidity (iridodonesis/flaccid iris) occurs, increasing the anteroposterior mobility of the iris. As a result, the optic is more likely to dislocate anterior to the iris during pupil dilation. 6)
4. Reverse pupillary block
Section titled “4. Reverse pupillary block”When anterior chamber pressure exceeds posterior chamber pressure, the pupillary margin adheres to the anterior surface of the IOL, acting as a valve (reverse pupillary block). The anterior dislocation of the IOL obstructs the flow of aqueous humor from the anterior chamber to the posterior chamber, creating a vicious cycle that further increases posterior chamber pressure. Characteristic findings include a deep anterior chamber and posterior bowing of the iris. 2)
5. Mechanism of UGH syndrome
Section titled “5. Mechanism of UGH syndrome”Mechanical chafing of the iris by the IOL support releases iris pigment. Pigment deposition in the trabecular meshwork leads to pigmentary glaucoma, and persistent chafing progresses to UGH syndrome, which combines iridocyclitis and hyphema.
6. Influence of IOL material and design
Section titled “6. Influence of IOL material and design”Ciliary sulcus fixation of one-piece acrylic IOLs tends to cause iris transillumination defects and pigment dispersion due to the sharp anterior optic/haptic edge. 7) Three-piece IOLs have a posterior haptic angle and lower risk of iris chafing during ciliary sulcus fixation. Adequate optic diameter (≥6.0 mm) and haptic length contribute to stability in ciliary sulcus fixation.
7. Recent research and future perspectives
Section titled “7. Recent research and future perspectives”Advances in outpatient repositioning techniques
Section titled “Advances in outpatient repositioning techniques”Kokame et al. (2022) reported a 30G needle paracentesis technique that managed pupillary capture in 18 of 495 eyes (3.6%) over 54 outpatient procedures. All procedures were performed painlessly under topical anesthesia and may serve as an effective alternative when operating room access is limited. Setting the scleral suture position 2 mm posterior to the limbus significantly reduced recurrence (p=0.025), indicating that optimizing intraoperative fixation position is important as a preventive strategy. 6)
Advances in intrascleral fixation
Section titled “Advances in intrascleral fixation”The Yamane method (flanged intrascleral fixation, 2017) uses a double-needle technique to fixate the IOL haptic within the sclera. Its advantage over conventional suturing is the avoidance of suture erosion or breakage, but since it lacks capsular support like suturing, the risk of pupillary capture remains. 8) The concept of sutureless intrascleral fixation was first reported by Gabor & Pavlidis (2007) 9), and Agarwal (2008) 10) described a sutureless fixation method using fibrin glue. The incidence of pupillary capture and comparison with suturing methods are topics for future investigation.
Optimization of scleral suture position
Section titled “Optimization of scleral suture position”Fixation at 2 mm posterior to the limbus has been shown to significantly reduce recurrence of pupillary capture (p=0.025), and accumulation of data toward standardization of optimal fixation position is desired. 6)
Intrascleral fixation avoids suture-related complications (erosion, breakage) compared to suturing methods, but since it also lacks capsular support, the risk of pupillary capture remains. Direct comparative data on the incidence of both are limited and require future investigation. 8)
8. References
Section titled “8. References”- Vote BJ, Tranos P, Bunce C, et al. Long-term outcome of combined pars plana vitrectomy and scleral fixated sutured posterior chamber intraocular lens implantation. Am J Ophthalmol. 2006;141(2):308-312. PMID: 16458685
- 東出朋巳. 眼内レンズ毛様溝縫着後の逆瞳孔ブロックによる虹彩捕獲とその治療. IOL & RS. 2009;23(3):410-412. URL: https://cir.nii.ac.jp/crid/1573950399792764160
- Lin K, Hu Z, Lin Z, Chen T, Tang Y, Wu R. Rectangular loop suture to correct iris capture of the posterior chamber intraocular lens. BMC Ophthalmol. 2020;20:383. doi:10.1186/s12886-020-01650-3.
- Kim SI, Kim K. Tram-Track Suture Technique for Pupillary Capture of a Scleral Fixated Intraocular Lens. Case Rep Ophthalmol. 2016;7(2):290-295. PMID: 27462257. PMCID: PMC4943309. doi:10.1159/000446208.
- Kim DH, Moon DRC, Kang YK, et al. Case report: Management of recurrent pupillary optic capture with sutureless surgical technique using 7-0 polypropylene flange. Front Med (Lausanne). 2024;11:1367905. doi:10.3389/fmed.2024.1367905.
- Kokame GT, Card K, Pisig AU, Shantha JG. In office management of optic capture of scleral fixated posterior chamber intraocular lenses. Am J Ophthalmol Case Rep. 2022;25:101356. doi:10.1016/j.ajoc.2022.101356.
- Miller KM, Oetting TA, Tweeten JP, Carter K, Lee BS, Lin S, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID:34780842.
- Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136-1142. PMID: 28457613
- Gabor SGB, Pavlidis MM. Sutureless intrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg. 2007;33(11):1851-1854. PMID: 17964387
- Agarwal A, Kumar DA, Jacob S, et al. Fibrin glue-assisted sutureless posterior chamber intraocular lens implantation in eyes with deficient posterior capsules. J Cataract Refract Surg. 2008;34(9):1433-1438. PMID: 18721701