Monovision with Contact Lenses
Reversibility: High (returns to baseline when CLs are removed)
Dominant eye: ±0 D (full distance correction)
Non-dominant eye: +1.5 to +2.0 D (near addition)
Features: Ideal for trial. Easy to adjust.

Monovision is a correction method in which one eye is corrected for distance and the other for near, covering distance and near vision through monocular vision.
Originally, “monovision” is mostly thought to develop when an anisometropic eye with one eye emmetropic (or near-emmetropic dominant eye) and the other moderately myopic (non-dominant eye) is left uncorrected during growth, resulting in impaired normal binocular vision. Its application to presbyopia correction is an intentional imitation of this physiological state.
As an option for patients troubled by presbyopia, it can be implemented via contact lenses, refractive surgery, or intraocular lenses (IOLs). Also, after refractive surgery or at presbyopic age, it is important to consider weaker correction or monovision taking into account not only distance vision but also intermediate to near vision.
Historical background and positioning of monovision:
Monovision was developed in the 1970s–1980s as a presbyopia correction method using contact lenses. Inspired by the observation that anisometropic individuals experienced functional distance and near vision even with contact lenses, it was later adopted in refractive surgeries such as LASIK and PRK. In cataract surgery, it is established as an alternative for patients who do not desire or are not suitable for multifocal IOLs. Since overcorrection leading to hyperopia can cause eye strain during near work, special attention is needed when designing correction for presbyopic ages.
It is a method where one eye is set for distance (emmetropia or distance correction) and the other eye for near (residual myopia or near addition), covering distance and near vision through monocular vision of each eye. The goal is to achieve distance and near vision without glasses. However, binocular stereopsis is reduced, which is disadvantageous for tasks requiring depth perception.
Patients with the following characteristics are good candidates for monovision.
Monovision is not suitable or requires careful evaluation in the following cases.
Monovision works because the visual cortex adapts to the difference in focus between the two eyes and preferentially uses the appropriate eye depending on viewing distance. If binocular rivalry does not occur, natural monovision is achieved.
The key to success is “binocular coordination and the brain’s adaptive capacity.” Prior experience with anisometropia, clear ocular dominance, and preserved binocular vision influence the prognosis.
In normal binocular vision, small differences between the two eyes (binocular disparity) are used to perceive depth (stereopsis). In monovision, one eye is intentionally defocused, so binocular disparity information becomes incomplete, reducing stereopsis.
Mini-monovision (addition of +0.75 to +1.00 D) is a compromise that minimizes the impact on stereopsis while providing some near vision. It is an option for patients who need to maintain stereopsis (e.g., sports enthusiasts).
Full monovision (addition of +1.50 to +2.00 D) provides better near vision but causes more significant reduction in stereopsis.
The dominant eye plays a central role in visual information processing. Setting the dominant eye for distance vision stabilizes information processing during distance viewing and increases the everyday acceptability of monovision.
For myopic eyes, undercorrecting one eye can solve the problem of aniseikonia (monovision glasses). In cases of anisometropia, it is desirable that the difference in spherical power between the two eyes does not exceed 1.5 D. If it exceeds this, contact lens correction or intentional monovision setting may be useful in reducing aniseikonia.
The standard procedure for evaluating the indication for the monovision method is described below.
① Determination of the dominant eye
Success is more likely when the dominant eye is set for distance and the non-dominant eye for near.
Quantitatively evaluate binocular stereopsis using TNO (random dot method) or Titmus (polaroid method). Preoperative stereopsis is related to the degree of stereopsis decline after monovision.
③ Refraction test and addition power setting
Set the addition power based on Sloan’s principle (reserve half of the accommodative amplitude as a reserve).
④ Trial fitting (CL trial)
Before surgery, simulate monovision with contact lenses for 1–2 weeks. Assess subjective acceptance in actual daily life (driving, reading, VDT work) before deciding on surgery. A trial using daily disposable CLs is easy to perform.
| Test item | Purpose | Criteria |
|---|---|---|
| Dominant eye determination | Determine distance eye | Hole-in-card / pointing test |
| Stereopsis test | Binocular vision assessment | TNO / Titmus |
| CL trial | Real-life adaptation check | 1–2 weeks of daily use |
| Refraction test | Add power setting | Sloan’s principle |
It is recommended to perform a trial wearing of contact lenses (1–2 weeks) before surgery. Experience the monovision vision in actual daily life (driving, reading, computer work), and if it is deemed acceptable, surgery is indicated. Also, confirmation of the dominant eye and stereopsis testing are always performed preoperatively.
There are three main methods for achieving monovision.
This is the most reversible method and is also used for initial trials.
Standard settings:
Prescription principles:
A method of intentionally leaving one eye myopic through LASIK, PRK, etc. Mainly targeted at middle-aged and older patients with presbyopia.
Standard target refraction settings:
Key points of preoperative evaluation:
Postoperative management:
A method of planning cataract surgery with one eye receiving a distance IOL and the other a near IOL (or set for residual myopia).
Setting considerations:
This is considered as an alternative for patients who do not desire multifocal IOLs or for whom multifocal IOLs are contraindicated (e.g., large higher-order aberrations, severe dry eye). Light-adjustable IOLs may also be an option for correcting postoperative refractive errors.
Monovision with Contact Lenses
Reversibility: High (returns to baseline when CLs are removed)
Dominant eye: ±0 D (full distance correction)
Non-dominant eye: +1.5 to +2.0 D (near addition)
Features: Ideal for trial. Easy to adjust.
Monovision with Surgery (LASIK/PRK)
Reversibility: Low (requires reoperation)
Dominant eye: 0 D (emmetropia)
Non-dominant eye: -1.25 to -1.50 D (intentional residual myopia)
Features: No CL needed. Successful CL trial is a prerequisite.
Monovision with IOL (Cataract Surgery)
Reversibility: Low (requires IOL exchange)
Dominant eye: 0 D (distance)
Non-dominant eye: -1.50 to -2.00 D (near setting)
Features: Alternative option for patients unsuitable for multifocal IOLs
While monovision is the basic approach, adding reading glasses for precise near work is also an option. For myopic patients, “monovision glasses” that use the undercorrected side for near vision under distance correction are a practical choice.
After cataract surgery with monovision setting, pay attention to the following:
Postoperative confirmation items:
Management of postoperative refractive error:
Relationship with smartphone/VDT use: In postoperative monovision patients, although accommodative load during smartphone use does not occur, convergence fatigue from prolonged near work can occur. Guidance on the working environment when using digital devices is provided as part of postoperative management.
Standard flow when conducting a monovision trial with CL:
Success of the CL trial is the best predictor of postoperative satisfaction 1). If the trial is unsatisfactory, do not proceed to surgery and consider other presbyopia correction options (bifocal/multifocal CL, progressive addition lenses, etc.).
Recommended follow-up schedule after monovision surgery:
If stereopsis decreases or dissatisfaction is strong after surgery, it is safer to first try adjusting correction with contact lenses (changing addition power or switching to multifocal CLs) before considering reoperation. Appropriate patient selection and thorough preoperative counseling are essential to maximize postoperative satisfaction.
Special attention is needed when applying to occupations that require depth perception and stereopsis:
| Occupation | Points to note | Countermeasures |
|---|---|---|
| Car/train driver | May affect passing the depth perception test | Check employment regulations; consider mini-monovision |
| Pilot (aviation) | Depth perception required; monovision may be prohibited | Must check aviation medical examination standards in advance |
| Construction worker / high-altitude work | Reduced depth perception affects safety | Check work details in detail; consider alternative methods |
| Surgeons / Dentists | Requires stereopsis for precision work | Option to add reading glasses during surgery |
| Athletes | Reduced depth perception in ball sports and combat sports | Consider mini-monovision; individual assessment |
Depth perception tests (driver’s license, some certifications) evaluate binocular stereopsis, so monovision may affect test results. If there are occupational risks, provide sufficient explanation and obtain consent before the procedure.
The addition required for presbyopia correction changes with age. As the addition increases, stereopsis decreases more noticeably, so regular reassessment based on age is necessary.
| Age | Accommodative Amplitude (Approx.) | Monovision Addition (Approx.) | Characteristics |
|---|---|---|---|
| 40–45 years | 3–5 D | +1.00 to +1.50 D | Manageable with low addition |
| 45–50 years | 2–3 D | +1.50 to +1.75 D | Consider intermediate distance as well |
| 50–55 years | 1–2 D | +1.75 to +2.00 D | Full monovision required |
| 55 years and older | 0–1 D | +2.00 to +2.50 D | Additional reading glasses may be needed |
Re-evaluation and adjustment of monovision are recommended every 2–3 years. As the addition increases, the degree of stereopsis reduction also increases, so it is important to consider switching to alternative methods (such as progressive addition lenses) early in patients with occupations requiring depth perception.
Understanding the factors that affect patient satisfaction can improve appropriate patient selection and the quality of preoperative counseling.
Factors associated with improved satisfaction:
Factors associated with dissatisfaction:
In preoperative counseling, it is essential to emphasize that the goal is not “perfect vision” but “practical daily vision without correction,” and to form realistic expectations to maintain postoperative satisfaction.
The position of monovision within the overall picture of presbyopia correction is as follows.
| Correction method | Main advantages | Main disadvantages | Indications |
|---|---|---|---|
| Progressive addition lenses | Full distance coverage, stereopsis maintained | Peripheral aberrations, adaptation required | Broadest indication |
| Multifocal contact lenses | No glasses needed | Slightly inferior visual quality | Contact lens wearers |
| Monovision (CL/surgery) | No glasses needed, maintains sharpness | Reduced stereopsis, individual variation in adaptation | Successful CL trial cases |
| Multifocal IOL | Full range, spectacle independence | Optical phenomena, high cost | During cataract surgery |
| Mini-monovision | Minimal impact on stereopsis | Limited improvement in near vision | Patients who value stereopsis |
Monovision plays an important role as a “practical intermediate option” for patients who experience strong optical discomfort with progressive addition lenses, those who do not want to wear glasses, and those who are not candidates for multifocal IOLs. It must be remembered that careful patient selection using a contact lens trial is the key to success.
Detailed pathophysiology is described in section “3. Pathophysiological Background.” Additional information is provided below.
Monovision inevitably creates a refractive difference (anisometropia) between the two eyes. When the difference in spherical power exceeds 1.5 D, aniseikonia tends to become problematic. Aniseikonia is perceived as an abnormality in spatial perception (sensation of tilt or distortion).
Correction with contact lenses has less impact on aniseikonia compared to glasses, so a monovision CL trial is also useful for predicting surgical success.
Multifocal CLs are also an option for presbyopia correction, but they differ from the monovision method in the following points:
| Item | Monovision method | Multifocal CL |
|---|---|---|
| Mechanism of action | Monocular vision (one eye for distance, one eye for near) | Simultaneous vision (center for near, periphery for distance, etc.) |
| Image clarity | Clear at each distance | Inferior to single-vision CLs |
| Stereopsis | Decreased | Relatively maintained |
| Indications | After confirmation in CL trial | Trial comparison |
| Dark environment | Contrast reduction is more pronounced with multifocal CLs | Decreased contrast sensitivity |
If multifocal CLs are not well tolerated, monovision with monofocal CLs (dominant eye for distance, non-dominant eye for near) combined with reading glasses is an option.
A smaller addition (+1.00 to +1.25 D) has minimal impact on stereopsis but limited improvement in near visual acuity, while a larger addition (+1.75 to +2.00 D) improves near visual acuity but significantly reduces stereopsis, presenting a trade-off 2).
When a monovision trial with CLs is conducted preoperatively, high postoperative patient satisfaction rates have been reported. Predictive factors for trial success include preoperative anisometropia experience, clear ocular dominance, and preserved binocular vision 1).
Determining the appropriate near addition is key to patient satisfaction. There is a trade-off: a low addition (+1.00 to +1.25 D) has minimal impact on stereopsis but limited improvement in near visual acuity, while a high addition (+1.75 to +2.00 D) improves near visual acuity but significantly reduces stereopsis 2).
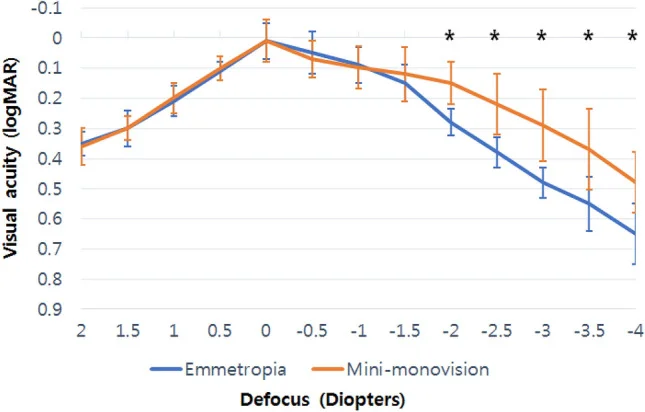
Mini-monovision (addition +0.75 to +1.25 D) is gaining attention as a compromise that compensates for presbyopia while relatively preserving stereopsis. Evidence is accumulating, especially in IOL settings during cataract surgery 3). Reports on mini-monovision using the new monofocal IOL (Eyhance ICB00) show that significantly better visual acuity is maintained in the intermediate to near vision range (−2.0 to −4.0 D) compared to the emmetropic group 5).
With increased use of smartphones, tablets, and other devices, visual acuity at intermediate distances (50–80 cm) has become more important. In contrast to traditional monovision (distance + near), a micro-monovision approach that prioritizes distance + intermediate vision is also being studied 4). In managing digital eye strain (DES), consideration for monovision patients is necessary, and the Tear Film & Ocular Surface Society (TFOS) has comprehensively summarized the impact of the digital environment on the ocular surface 7).
Studies comparing multifocal IOLs and monofocal IOL monovision show that multifocal IOLs provide superior vision at all distances, but have a higher incidence of optical phenomena such as halos and glare. Selection according to the patient’s lifestyle priorities is important 3). A meta-analysis of 22 trials and 2,200 eyes comparing trifocal IOLs and EDOF IOLs showed that trifocal IOLs are superior in near visual acuity and spectacle independence 6), providing a reference when considering multifocal IOLs as an alternative to monovision.
Selection Guide: Multifocal IOL vs. Monovision (Monofocal IOL):
| Aspect | Multifocal IOL | Monovision (Monofocal IOL) |
|---|---|---|
| Vision at all distances | Superior (far to near) | Specialized for distance or near |
| Stereopsis | Relatively preserved | Decreased |
| Optical phenomena (halo/glare) | Frequent | Less frequent |
| Night vision | Risk of decreased | Relatively good |
| Spectacle independence | High | Moderate |
| Cost (selected medical care/out-of-pocket) | Expensive | Relatively inexpensive |
| Indications | Active lifestyle / multiple distance needs | Frequent night driving / cannot tolerate halos |
For patients with severe dry eye, large higher-order aberrations, or concerns about reduced contrast sensitivity, monovision with a monofocal IOL is often more suitable than a multifocal IOL.
In the digital device era, screen time is increasing globally 8)9), and even patients who have undergone monovision require attention to intermediate distance visual function. Particularly in patients with long screen time, accommodative fatigue is more likely to occur 10)11), and optimization of the work environment in addition to monovision settings is important 12). The impact of increased screen time has also been reported in children and young adults 14), and evaluation of digital device usage is essential across all age groups undergoing presbyopia correction 13)15)16)17).
Greenbaum S. Monovision pseudophakia. Journal of cataract and refractive surgery. 2002;28(8):1439-43. doi:10.1016/s0886-3350(02)01218-x. PMID:12160816.
Jain S, Arora I, Azar DT. Success of monovision in presbyopes: review of the literature and potential applications to refractive surgery. Survey of ophthalmology. 1996;40(6):491-9. doi:10.1016/s0039-6257(96)82015-7. PMID:8724641.
Zhang F, Sugar A, Jacobsen G, Collins M. Visual function and patient satisfaction: Comparison between bilateral diffractive multifocal intraocular lenses and monovision pseudophakia. Journal of cataract and refractive surgery. 2011;37(3):446-53. doi:10.1016/j.jcrs.2010.10.045. PMID:21333868.
Evans BJ.. Monovision: a review. Ophthalmic Physiol Opt. 2007;27(5):417-439. doi:10.1111/j.1475-1313.2007.00488.x. PMID:17718882.
Shimizu K, Ito M, Igarashi S, et al. Visual outcomes and spectacle independence of pseudophakic mini-monovision using a new monofocal intraocular lens. Sci Rep. 2022;12(1):22384.
Karam M, Alkhowaiter N, Alkhabbaz A, Aldubaikhi A, Alsaif A, Shareef E, et al. Extended Depth of Focus Versus Trifocal for Intraocular Lens Implantation: An Updated Systematic Review and Meta-Analysis. American journal of ophthalmology. 2023;251:52-70. doi:10.1016/j.ajo.2023.01.024. PMID:36736751.
Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: Impact of the digital environment on the ocular surface. Ocul Surf. 2023 Apr;28:213-252. doi:10.1016/j.jtos.2023.04.004. PMID:37062428.
Kirandeep Kaur, Bharat Gurnani, Swatishree Nayak, Nilutparna Deori, Savleen Kaur, Jitendra Jethani, et al. Digital Eye Strain- A Comprehensive Review. Ophthalmol Ther. 2022;11(5):1655-1680. doi:10.1007/s40123-022-00540-9.
León-Figueroa DA, et al. Prevalence of computer vision syndrome during the COVID-19 pandemic. BMC Public Health. 2024;24:640. doi:10.1186/s12889-024-17636-5. PMID:38424562; PMCID:PMC10902934.
Song F, Liu Y, Zhao Z, Shang X, Wang Y, Lai M, et al. Clinical manifestations, prevalence, and risk factors of asthenopia: a systematic review and meta-analysis. Journal of global health. 2026;16:04053. doi:10.7189/jogh.16.04053. PMID:41648943; PMCID:PMC12879263.
Thakur M, Panicker T, Satgunam P. Refractive error changes and associated asthenopia observed after COVID-19 infection: Case reports from two continents. Indian J Ophthalmol. 2023;71(6):2592-2594. PMID: 37322686. PMCID: PMC10418019. doi:10.4103/IJO.IJO_2581_22.
Pavel IA, Bogdanici CM, Donica VC, Anton N, Savu B, Chiriac CP, et al. Computer Vision Syndrome: An Ophthalmic Pathology of the Modern Era. Medicina (Kaunas, Lithuania). 2023;59(2). doi:10.3390/medicina59020412. PMID:36837613; PMCID:PMC9961559.
Barata MJ, et al. A Review of Digital Eye Strain: Binocular Vision Anomalies, Ocular Surface Changes. J Eye Mov Res. 2025. doi:10.3390/jemr18050039. PMID:40989226; PMCID:PMC12452390.
Bhattacharya S, et al. Let There Be Light-Digital Eye Strain (DES) in Children as a Shadow Pandemic. Front Public Health. 2022;10:945082. doi:10.3389/fpubh.2022.945082. PMID:36033797; PMCID:PMC9403324.
Lem DW, et al. Can Nutrition Play a Role in Ameliorating Digital Eye Strain? Nutrients. 2022;14(19):4005. doi:10.3390/nu14194005. PMID:36235656; PMCID:PMC9570730.
Anbesu EW, Lema. Prevalence of computer vision syndrome. Sci Rep. 2023;13:1801. doi:10.1038/s41598-023-28750-6. PMID:36720986; PMCID:PMC9888747.
Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: Impact of the digital environment on the ocular surface. Ocul Surf. 2023 Apr;28:213-252. doi:10.1016/j.jtos.2023.04.004. PMID:37062428.