Prolonged use of smartphones, computer displays, video games, etc., under poor conditions can lead to various physical and mental symptoms centered on the visual system (eyes), known as VDT (visual display terminals) syndrome. It is also called technostress eye syndrome or IT eye strain. In recent years, it has also been referred to as digital eye strain (DES), and its prevalence is increasing due to the widespread use of smartphones across all generations 1).
It is reported that 50–90% of VDT workers experience ocular symptoms 1), and it is internationally recognized as an occupational eye disease. The Ministry of Health, Labour and Welfare of Japan issued the “Guidelines for Occupational Health Management in Information Device Work” (revised in 2019), requiring employers to manage workers’ health 2). Since 2020, the spread of remote work and increased screen time due to the COVID-19 pandemic has further increased the number of affected individuals 3).
The main situations where VDT syndrome becomes a problem are shown below.
Occupational exposure: Increased risk due to VDT work for 4 hours or more per day2)
Long screen time: In children and adolescents, association with myopia is being studied7)
Use of 3D displays: Effects on the autonomic nervous system due to dissociation between accommodation and convergence
Inappropriate work environment: Combination of environmental factors such as lighting, screen position, and indoor dryness
QAre VDT syndrome and IT eye disease the same?
A
VDT syndrome, IT eye disease, technostress eye disease, and digital eye strain (DES) are all different names for the same condition. VDT (visual display terminals) syndrome is the traditional medical term, while IT eye disease is a more everyday expression. In recent years, the term “Digital Eye Strain” has been increasingly used internationally, and the definition and pathophysiology are the same.
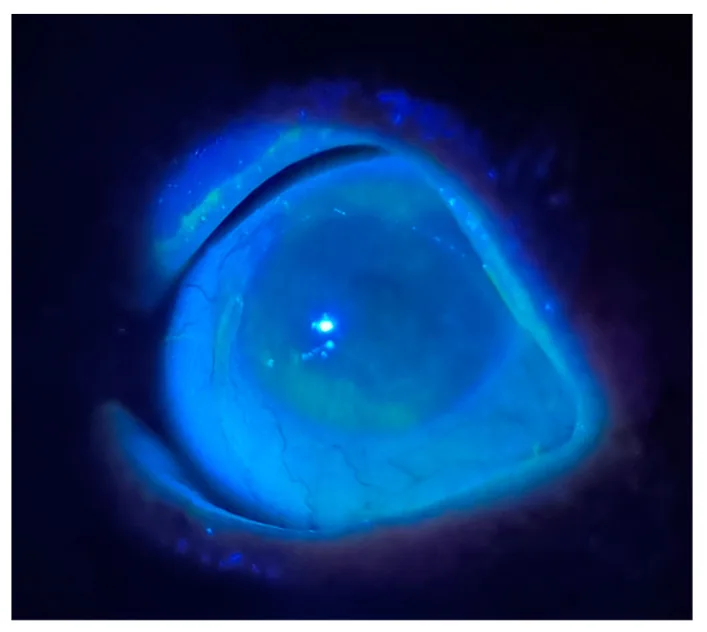
Kwon J, Moghtader A, Kang C, et al. Overview of Dry Eye Disease for Primary Care Physicians. Medicina (Kaunas). 2025;61(3):460. Figure 2. PMID: 40142272; PMCID: PMC11943967; DOI: 10.3390/medicina61030460. License: CC BY.
Slit-lamp examination photograph of a 68-year-old female dry eye patient, showing corneal damage visualized by applying fluorescein and irradiating with blue light from an ophthalmoscope in a dark room. Extensive epithelial staining (green fluorescence) is observed on the corneal surface, indicating a pattern of epithelial damage due to dry eye. This corresponds to the objective findings of dry eye discussed in the section “2. Main symptoms and clinical findings”.
Symptoms of VDT syndrome are broadly divided into three groups: ocular symptoms, systemic symptoms, and mental symptoms.
Ocular symptoms
Eye fatigue and pain: Mainly accommodative fatigue due to excessive tension of the ciliary muscle
Dry eyes and blurred vision: Decreased blinking causes tear evaporation, leading to functional dry eye
Accommodation and convergence disorders: The coordination of accommodation, miosis, and convergence breaks down, making it difficult to switch between near and far vision
Systemic symptoms
Neck, shoulder, arm stiffness and low back pain: Accumulation of musculoskeletal load due to prolonged poor posture
Fatigue and numbness in limbs: Peripheral symptoms due to impaired blood flow and sustained muscle tension
Menstrual irregularities: Endocrine effects mediated by autonomic nervous system disruption
Mental symptoms
Insomnia: Circadian rhythm disruption by blue light 9) and excessive cognitive activity
Depression and decreased concentration: Mental symptoms due to chronic stress and autonomic nervous system effects
Technostress: Psychological burden from excessive contact with screens and information
During VDT work, the blink rate is said to decrease from about 20 times per minute to about 7 times per minute 4). Combined with a dry office environment, this leads to functional dry eye. Shortened tear film breakup time (BUT) is also observed 5). After work, a compensatory increase in blink rate may occur.
After VDT work, the synergy of the three components of the near response (accommodation, miosis, convergence) is disrupted, causing inconsistency in simultaneous induction. Accommodation analysis devices show normal responses to distant targets, but patterns of accommodative spasm or excessive accommodation are detected for near targets.
The presence of refractive errors (especially myopia and presbyopia) or ocular misalignment (e.g., convergence insufficiency exophoria) significantly exacerbates symptoms. In people over 40, convergence insufficiency exophoria often appears against a background of presbyopia, requiring careful examination.
QWhy do non-ocular symptoms occur in VDT syndrome?
A
Prolonged poor posture during VDT work places continuous strain on the musculoskeletal system of the neck, shoulders, arms, and lower back, causing stiffness and pain. Additionally, stress from excessive information processing and sustained concentration disrupts the balance of the autonomic nervous system, leading to mental symptoms such as insomnia and depression. Furthermore, circadian rhythm disruption by blue light promotes sleep disorders. The combination of these musculoskeletal, mental, and autonomic nervous system effects produces a variety of systemic symptoms, which is characteristic of VDT syndrome.
Presbyopia in individuals aged 40 and older: Difficulty focusing on intermediate distances (computer screen)
Ocular misalignment (convergence insufficiency-type exophoria or esophoria): Requires excessive effort for binocular vision
History of dry eye: Worsening of symptoms due to decreased blinking
Environmental factors:
Inappropriate lighting: Glare and flicker increase accommodative load
Screen position and distance: Symptoms worsen when the distance between the eyes and monitor is less than 40 cm or more than 70 cm
Indoor dryness: Low humidity from air conditioning promotes tear evaporation 5)
Direct airflow from heating or cooling: Drying irritation to the cornea
3D displays and smartphones:
When viewing 3D displays: the accommodation point is on the screen, but the convergence point deviates from the screen, which may affect the autonomic nervous system.
Prolonged screen time: In children and adolescents, an association with myopia has been considered 7).
The diagnosis of IT eye syndrome is primarily one of exclusion. While ruling out underlying diseases and other ophthalmic or systemic conditions, the relationship between the work environment and symptoms is evaluated.
Medical history:
Details of the work environment (type, position, distance, and lighting of the monitor)
Daily VDT work hours and continuous duration
Presence of symptoms other than ocular (insomnia, mental symptoms)
Confirmation of medications (psychiatric drugs, antiallergic drugs, etc.): These drugs may worsen accommodation disorders and dry eye.
Ophthalmic examination items:
Refraction and visual acuity tests: Evaluate accurate refraction values for distance, near, and intermediate distance (60 cm). If symptoms are severe, refraction under cycloplegia using cyclopentolate eye drops is recommended.
Ocular alignment test: Evaluation of distance and near ocular alignment using the prism cover test. In people aged 40 and older, convergence insufficiency-type exophoria tends to appear.
Age 40 or older, decreased near visual acuity. Symptoms disappear with appropriate reading glasses.
Sjögren’s syndrome
Accompanied by dry mouth and systemic symptoms. Positive for anti-SS-A/SS-B antibodies.
Glaucoma
Elevated intraocular pressure, optic disc changes, visual field defects. Asthenopia may be the initial symptom.
Cervical spondylosis
Primarily presents with neck-shoulder-arm pain. Accompanied by neurological findings (e.g., tendon reflexes, muscle weakness).
QHow is VDT syndrome diagnosed?
A
There are no specific diagnostic criteria for VDT syndrome; diagnosis is primarily based on exclusion. First, a detailed history of the work environment, work hours, and symptoms is obtained. Then, refractive error, ocular alignment, accommodative function, and tear film are assessed using appropriate tests. After excluding or identifying organic diseases such as dry eye, accommodative disorders, convergence insufficiency, presbyopia, and glaucoma, a diagnosis is made if a temporal and quantitative relationship with VDT work is established. It is important to carefully check for underlying diseases.
Treatment for VDT syndrome involves a combination of improving the work environment, appropriate refractive correction, medication, and management of musculoskeletal and psychological symptoms.
Proper correction of refractive errors: Correct nearsightedness, farsightedness, and astigmatism accurately.
Presbyopia management for those over 40: Distance glasses alone may not focus at intermediate distances (computer screen). Progressive lenses or intermediate-distance glasses are effective.
Vitamin B12 supplementation and improvement of eye strain
Moisturizing eye drops are often used in combination with Hyalein and Mucosta or Diquas. Mydrin M ophthalmic solution (0.4% tropicamide/phenylephrine) applied at bedtime relieves ciliary muscle hypertonicity (accommodative spasm) after VDT work.
Management of musculoskeletal and psychiatric symptoms
Environmental adjustments: Review desk, chair, and screen placement to improve poor posture
Exercise therapy: Incorporate light exercise, walking, and stretching into daily routine
Collaboration with specialists: Consult an orthopedic surgeon if neck, shoulder, arm, or back symptoms are severe
Management of psychiatric symptoms: Provide counseling and, if necessary, prescribe anxiolytics, antidepressants, or sleep aids in collaboration with a psychiatrist or psychosomatic medicine specialist
QWhat eye drops are effective for VDT syndrome?
A
Multiple eye drops are combined according to symptoms. For dryness, artificial tears (Soft Santear, 2-3 drops per dose, 5-6 times daily) and hyaluronic acid eye drops (Hyalein 0.1%, 5-6 times daily) are basic. Adding mucin secretion-promoting Mucosta eye drops UD (2%) or Diquas eye drops (3%) is effective. If accommodative spasm (excessive tension of the eye’s focusing muscle) is suspected, Mydrin M eye drops (0.4%) are instilled before bedtime. For general eye strain, Sancoba eye drops (0.02%) are also used.
During VDT work, concentration on visual stimuli causes suppression of blinking from the frontal lobe, reducing the normal blink rate of about 20 times per minute to about 7 times per minute 4). Blinking is essential for maintaining the tear film, and decreased blinking accelerates tear evaporation, destabilizing the tear film. Low humidity from office air conditioning further exacerbates this. Tear film breakup time (BUT) is shortened 5), creating a vicious cycle of dry eye due to exposure and drying of the corneal epithelium. The prevalence of dry eye among VDT workers is reported to be over 60% in office workers 11).
The near response is a physiological reaction in which three elements—accommodation (focusing), miosis (pupil constriction), and convergence (inward turning of both eyes)—are neurologically linked and simultaneously induced. After prolonged VDT work, this synkinesis is disrupted, causing inconsistency in the simultaneous induction of the three elements. Even when trying to look at a distance, accommodation does not relax sufficiently, and accommodative spasm or excessive convergence persists.
As an indicator of ciliary muscle fatigue, an increase in the high-frequency component (HFC) of accommodative microfluctuation is known 8). By detecting the increase in HFC using an accommodative function analyzer, ciliary muscle fatigue can be objectively evaluated.
Blue light (380-500 nm) strongly stimulates intrinsically photosensitive retinal ganglion cells (ipRGCs) containing melanopsin 9). Signals from ipRGCs regulate circadian rhythm via the suprachiasmatic nucleus, and strong blue light exposure at night can suppress melatonin secretion, potentially causing sleep disorders 9). This is the mechanism by which using smartphones or tablets before bedtime leads to insomnia and poor sleep quality.
Effects of Electromagnetic Waves and Chemical Substances
There are reports of corneal damage caused by extremely low-frequency electromagnetic waves emitted from computer monitors and smartphones. Additionally, it has been pointed out that chemical substances volatilized from recent computer products may contribute to the complexity of symptoms.
When viewing a 3D display, the focal point of accommodation is on the screen (fixed distance), while the convergence point shifts away from the screen to perceive pop-out and depth. This dissociation between accommodation and convergence disrupts the coordination of the physiological near response, leading to effects on the autonomic nervous system and discomfort.
Whether blue light blocking spectacle lenses are beneficial for eye strain, sleep, and macular health has long been a subject of debate. A Cochrane review by Downie et al. (2023) meta-analyzed 28 RCTs and concluded that there is insufficient evidence that blue light blocking lenses reduce daytime eye strain, and there is no basis for recommendation 6). Regarding effects on sleep and prevention of macular disease, current evidence is also insufficient to support a recommendation 6).
The association between screen time and myopia progression has been examined in systematic reviews 7), with prolonged smartphone use in children and adolescents particularly noted as a risk factor for myopia progression. Confounding with reduced outdoor activity time has been pointed out 7), and a combination of screen time limitation and promotion of outdoor activities is recommended from the perspective of myopia prevention.
Increase in VDT Syndrome After the COVID-19 Pandemic
The shift to remote work and the surge in prolonged screen use after the COVID-19 pandemic have significantly increased the prevalence of VDT syndrome3). A study by Mohan et al. (2021) reported in detail the prevalence and associated risk factors of digital eye strain during the pandemic 3), and this trend is expected to continue even after the establishment of hybrid work.
Research is progressing on AI-assisted systems that analyze posture, blink frequency, and the distance between the eyes and the screen in real time from camera images during work. In the future, comprehensive VDT health management tools integrated with automatic work environment adjustment and break reminder functions are expected to be put into practical use.
Development of new therapeutic drugs for dry eye related to VDT work is underway. In addition to existing drugs such as diquafosol and rebamipide, clinical trials of agents with new mechanisms that promote tear secretion (e.g., beta-3 receptor agonists) are being conducted 10), and expansion of future options is anticipated.
Mohan A, Sen P, Shah C, et al. Prevalence and risk factor assessment of digital eye strain during COVID-19 pandemic. Indian J Ophthalmol. 2021;69(6):1420-1426.
Tsubota K, Nakamori K. Dry eyes and video display terminals. N Engl J Med. 1993;328(8):584.
Uchino M, Schaumberg DA, Dogru M, et al. Prevalence of dry eye disease among Japanese visual display terminal users. Ophthalmology. 2008;115(11):1982-1988.
Downie LE, Keller PR, Busija L, et al. Blue-light filtering spectacle lenses for visual performance, sleep, and macular health in adults. Cochrane Database Syst Rev. 2023;8(8):CD013244.
Lanca C, Saw SM. The association between digital screen time and myopia: a systematic review. Ophthalmic Physiol Opt. 2020;40(2):216-229.
Iwasaki T, Kurimoto S. Objective evaluation of eye strain using measurements of accommodative oscillation. Ergonomics. 1987;30(3):581-587.
Tosini G, Ferguson I, Tsubota K. Effects of blue light on the circadian system and eye physiology. Mol Vis. 2016;22:61-72. PMID: 26900325.
Rosenfield M. Computer vision syndrome: a review of ocular causes and potential treatments. Ophthalmic Physiol Opt. 2011;31(5):502-515.
Courtin R, Pereira B, Naughton G, et al. Prevalence of dry eye disease in visual display terminal workers: a systematic review and meta-analysis. BMJ Open. 2016;6(1):e009675.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.