Sleep disorders have various systemic effects, and their impact on the eyes has recently gained attention. In particular, obstructive sleep apnea syndrome (OSAS) has been shown by systematic reviews and meta-analyses to increase the risk of several eye diseases through intermittent hypoxia, intraocular pressure fluctuations, and impaired ocular blood flow.
The global prevalence of OSAS is estimated at approximately 15% in adult men and 5% in adult women 1). The problem is that about 80% of cases remain undiagnosed 1), and many patients are unaware of their risk for eye diseases. Reports indicate that the frequency of various eye diseases is significantly higher in OSAS patients compared to non-OSAS individuals 2).
The relationship between sleep and eye diseases can be understood in terms of quantitative and qualitative sleep issues.
Quantitative sleep deficiency (sleep deprivation, sleep debt): Reduces tear secretion and destabilizes the tear film, worsening dry eye3). Combined with VDT (video display terminal) work, ocular surface damage is further exacerbated.
Qualitative sleep disorder (OSAS): Affects the optic nerve, retina, eyelids, and ocular surface through intermittent hypoxia, intraocular pressure fluctuations, and impaired ocular blood flow.
QIf I have sleep apnea, should I also see an ophthalmologist?
A
OSAS patients have a higher risk of eye diseases such as glaucoma, floppy eyelid syndrome, and non-arteritic anterior ischemic optic neuropathy (NAION), so regular ophthalmologic examinations are recommended 2). Main tests include intraocular pressure measurement, visual field testing, OCT (retinal nerve fiber layer thickness measurement), eyelid laxity evaluation, and tear film tests. It is important to see an ophthalmologist alongside OSAS treatment to detect eye diseases early.
2. Major Eye Diseases Associated with Sleep Disorders
The following are eye diseases reported to be associated with OSAS and sleep disorders.
Glaucoma (Normal-Tension Glaucoma)
Definition: A subtype of glaucoma in which optic nerve damage progresses even when intraocular pressure is within the normal range.
Association with OSAS: Meta-analyses report an odds ratio of 1.2 to 2.0 for the comorbidity of OSAS and glaucoma5). In particular, the association with normal-tension glaucoma has attracted attention6), and nocturnal intermittent hypoxia and elevated intraocular pressure are thought to cause optic nerve damage.
Floppy Eyelid Syndrome (FES)
Definition: A condition in which excessive laxity of the eyelids causes the upper eyelid to easily evert during sleep, exposing the ocular surface.
Association with OSAS: A strong association with OSAS has been established4), and approximately 16% of OSAS patients have comorbid FES4). Symptoms include eye discharge, redness, and corneal erosion upon waking.
Definition: A disease in which acute optic nerve damage occurs due to impaired blood flow to the optic disc.
Association with OSAS: OSAS patients have an increased risk of NAION10). Impaired blood flow to the optic disc due to nocturnal intermittent hypoxia is considered the main mechanism.
Dry Eye
Definition: Ocular surface damage due to abnormalities in the quality or quantity of tears.
Association with Sleep: Sleep deprivation reduces parasympathetic nerve function and decreases tear secretion3). Air leaks from CPAP masks used for OSAS treatment also cause ocular surface dryness8).
Central Serous Chorioretinopathy (CSC)
Definition: A disease in which serous fluid accumulates under the retina due to increased choroidal vascular permeability.
Association with sleep: Psychological stress, corticosteroids, and the mineralocorticoid pathway are associated with the pathogenesis of CSC9).
Retinal Vein Occlusion
Definition: A disease in which the retinal vein becomes occluded, causing hemorrhage and edema in the retina.
Association with OSAS: Arteriosclerosis due to OSAS, hypertension, and dyslipidemia increases the risk of retinal vascular disorders. Vascular endothelial damage and hyperviscosity of blood predispose to occlusion.
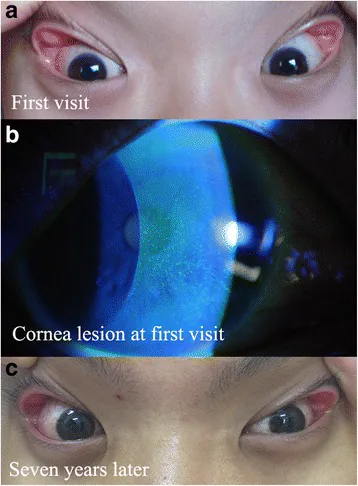
Gao YY, Wang HJ. Superficial punctate keratopathy in a pediatric patient was related to adenoid hypertrophy and obstructive sleep apnea syndrome: a case report. BMC Ophthalmol. 2018;18:55. Figure 1. PMCID: PMC5824558. License: CC BY.
Case photographs showing grade 2 lax eyelids and mild conjunctival injection in both eyes at the first visit (a), scattered punctate corneal epithelial defects in the right eye confirmed by fluorescein staining (b), and the degree of lax eyelids unchanged after 7 years (c). These correspond to the clinical findings of floppy eyelid syndrome (FES) discussed in the section “2. Major eye diseases associated with sleep disorders”.
QWhat eye diseases does sleep apnea syndrome increase the risk of?
A
OSAS mainly increases the risk of the following eye diseases: ① Glaucoma (especially normal-tension glaucoma): meta-analysis shows OR 1.2–2.0 5), ② Floppy eyelid syndrome: occurs in about 16% of OSAS patients 4), ③ Non-arteritic anterior ischemic optic neuropathy (NAION): optic nerve blood flow impairment due to nocturnal hypoxia 10), ④ Dry eye: air leak associated with CPAP therapy 8), ⑤ Central serous chorioretinopathy: association with psychological stress and corticosteroid pathway 9). From the perspective of these disease risks, regular ophthalmologic examinations are recommended for OSAS patients.
The main mechanisms by which OSAS causes eye diseases are as follows.
Intermittent Hypoxia (IH): The repeated hypoxia-reoxygenation cycles characteristic of OSAS lead to increased production of reactive oxygen species (ROS), causing oxidative stress2). Endothelial cell dysfunction impairs the microcirculation of the optic nerve and retina.
Intraocular pressure fluctuation: Sleeping in the supine position and increased negative intrathoracic pressure during apnea raise the episcleral venous pressure, increasing outflow resistance and elevating intraocular pressure7). Nocturnal IOP elevation is easily missed during daytime measurements and is noted as one cause of normal-tension glaucoma.
Ocular blood flow impairment: Chronic sympathetic activation associated with OSAS leads to vasospasm and increased peripheral vascular resistance, disrupting the autoregulation of blood flow to the optic disc and retina10). This contributes to NAION and glaucomatous optic nerve damage.
Elevation of inflammatory cytokines: IH increases inflammatory cytokines such as TNF-α and IL-6, promoting vascular damage 11). It may also be involved in promoting apoptosis of retinal ganglion cells14).
Stress-related pathways: Psychological stress, glucocorticoid, and mineralocorticoid receptor pathways are included in the pathological hypothesis of CSC9).
Decreased parasympathetic function: Sleep deprivation shifts autonomic balance toward sympathetic dominance, leading to reduced tear secretion mediated by the parasympathetic system 3).
The gold standard for diagnosing OSAS is overnight polysomnography (PSG) 1). PSG simultaneously records electroencephalogram, eye movements, electromyogram, SpO2, airflow, and effort to evaluate the nature and severity of apnea.
Severity classification is based on the Apnea-Hypopnea Index (AHI) 1).
Severity
AHI (events/hour)
Characteristics
Normal
<5
No problem
Mild
5 to <15
Often with minimal symptoms
Moderate
15 to less than 30
Daytime sleepiness and reduced concentration appear
Severe
30 or more
Severe daytime sleepiness and increased risk of cardiovascular complications
The Epworth Sleepiness Scale (ESS) is used for screening excessive daytime sleepiness 12). The ESS is an 8-item self-administered questionnaire, and a total score of 10 or more is considered indicative of hypersomnia.
OCT (Optical Coherence Tomography): Measurement of retinal nerve fiber layer (RNFL) thickness. Detects early glaucomatous changes.
Fundus examination: Evaluate optic disc cupping, retinal hemorrhage, and presence of NAION.
Lid laxity test: Diagnosis of FES. Check whether the upper eyelid can be easily everted 4).
Tear film testing: Dry eye evaluation using Schirmer test and tear break-up time (BUT) measurement.
QWhat does ophthalmologic screening for sleep apnea syndrome involve?
A
The recommended ophthalmologic examinations for OSAS patients include: (1) intraocular pressure measurement (including diurnal variation), (2) visual field testing (Humphrey static perimetry), (3) OCT measurement of RNFL thickness, (4) fundus examination (evaluation of optic disc and retina), (5) assessment of eyelid laxity (lid laxity test for FES diagnosis4)), and (6) tear film tests (Schirmer test, BUT). These can help detect glaucoma, NAION, FES, and dry eye at an early stage.
CPAP (continuous positive airway pressure) therapy is the first-line treatment for OSAS1). It delivers positive pressure air through the nose or mouth during sleep to keep the upper airway open, suppressing apnea and hypopnea. CPAP therapy is expected to improve AHI, relieve daytime sleepiness, and reduce the risk of cardiovascular complications.
However, if the CPAP mask does not fit properly, air leaks can dry the ocular surface and worsen dry eye8). If eye symptoms appear after starting CPAP, the mask size and shape should be readjusted.
Oral appliances (OA) are used as an alternative treatment for mild to moderate OSAS1). They hold the lower jaw in a forward position to reduce upper airway obstruction. They are an option for patients who cannot tolerate CPAP.
Weight loss and lifestyle modification: Reducing BMI is known to improve the severity of OSAS1). For obese OSAS patients, weight loss can be a fundamental treatment.
Intraocular pressure management with topical hypotensive agents (prostaglandin analogs, beta-blockers, etc.). For severe cases, selective laser trabeculoplasty (SLT) or surgery. Concurrent management of OSAS is recommended5)
Eyelid fixation with light-blocking tape during sleep. For severe cases (recurrent corneal erosion, corneal opacity), surgical treatment such as eyelid shortening4)
Dry eye (CPAP-related)
Use artificial tears and moisturizing eye drops. Adjust CPAP mask size and position. Use hyaluronic acid 0.1–0.3% eye drops 4–6 times daily 8)
NAION
Acute-phase steroid administration (limited efficacy). The fundamental treatment is management of OSAS 10). If optic disc swelling is confirmed in the acute phase, promptly refer to a specialist facility
Intravitreal injection of anti-VEGF drugs for macular edema. Control hypertension and dyslipidemia
QIs CPAP treatment effective for eye diseases?
A
CPAP therapy improves intermittent hypoxia in OSAS, which is expected to reduce the risk of optic nerve damage. Some studies suggest it may suppress glaucoma progression and prevent recurrence of NAION13), but definitive RCT evidence is currently limited. On the other hand, dry eye worsening due to air leakage from the CPAP mask has been reported as a side effect 8). If ocular symptoms appear after starting CPAP, mask fitting should be reviewed and an ophthalmology consultation is necessary.
OSAS is a disease in which the airway repeatedly closes due to relaxation of the soft tissues of the upper airway during sleep 1). Obstruction causes ventilation to stop (apnea) or decrease (hypopnea), leading to a drop in blood oxygen saturation (SpO2). When hypoxia reaches a certain level, an arousal response occurs, opening the airway. This cycle of apnea → hypoxia → arousal → airway opening is repeated dozens to hundreds of times per night.
Intermittent Hypoxia-Reoxygenation (IH) and Oxidative Stress
Repeated hypoxia and reoxygenation in IH induce massive production of reactive oxygen species (ROS) through a mechanism similar to ischemia-reperfusion injury 11). ROS suppress nitric oxide (NO) production in vascular endothelial cells, reducing vasodilation capacity. In the microvessels of the retina and optic nerve, endothelial damage progresses through a similar mechanism, leading to chronic blood flow reduction.
Furthermore, IH activates the transcription factor NF-κB, leading to increased production of inflammatory cytokines such as TNF-α, IL-6, and IL-8 11). These inflammatory mediators promote vascular damage through increased vascular permeability, leukocyte adhesion, and platelet aggregation.
Sleeping in the supine position is known to increase intraocular pressure by 2–6 mmHg compared to the sitting position 7). Increased negative intrathoracic pressure during apnea in OSAS raises superior vena cava and head/neck venous pressure, which in turn increases episcleral venous pressure and resistance to aqueous humor outflow. As a result, intraocular pressure rises 7).
It has also been reported that CPAP therapy may paradoxically increase intraocular pressure7), and intraocular pressure monitoring during CPAP use may be recommended in some cases.
In healthy individuals, optic nerve head blood flow has autoregulation that maintains constant flow despite fluctuations in ocular perfusion pressure. Sympathetic hyperactivity and vascular endothelial damage associated with OSAS impair this autoregulation, leading to a hypoperfusion state 10). Repeated nocturnal hypoxia causes reduced blood flow to the optic nerve head under conditions of impaired autoregulation, which is thought to contribute to the development of NAION and normal-tension glaucoma.
Promotion of apoptosis (programmed cell death) of retinal ganglion cells under hypoxic conditions has also been confirmed in animal experiments 14), suggesting a link to glaucomatous optic neuropathy.
RCTs are being conducted to verify whether CPAP therapy suppresses glaucoma progression 13). A study by Chen et al. (2014) showed that the association with glaucoma weakened in patients who underwent OSAS surgery 13), suggesting that OSAS treatment may contribute to reducing glaucoma risk. However, RCTs directly demonstrating the suppression of glaucoma progression by CPAP therapy itself are currently limited, and further evidence accumulation is awaited.
Causal Inference Using Mendelian Randomization Studies
The association between OSAS and glaucoma has been epidemiologically demonstrated, but it is difficult to completely exclude confounding factors (hypertension, diabetes, obesity, etc.). In recent years, studies using Mendelian Randomization methods with genetic variants as instrumental variables have been conducted to examine causality 15). This approach is expected to more rigorously test whether OSAS is an independent cause of glaucoma.
Continuous monitoring of nighttime SpO2 using wearable devices such as smartwatches is advancing as a screening tool for OSAS. Longitudinal studies combining nighttime hypoxia records with ophthalmic indicators (RNFL thickness, visual field) are expected to improve the accuracy of eye disease risk prediction.
Research on Inflammatory Biomarkers and Eye Diseases
Studies investigating the association between inflammatory biomarkers such as TNF-α and IL-6 and the severity of OSAS and progression of eye diseases are ongoing 11). If risk stratification for eye diseases using biomarkers becomes feasible, early ophthalmologic intervention for high-risk patients is expected.
Cross-disciplinary Care between Sleep Medicine and Ophthalmology
Diagnosis and treatment of OSAS are primarily handled by respiratory medicine and otorhinolaryngology, but establishing a multidisciplinary collaboration system with ophthalmologic complications in mind is an important issue. Standardization of clinical protocols linking sleep specialty clinics and ophthalmology clinics is a future perspective.
Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687-698.
Huon LK, Liu SY, Camacho M, et al. The association between ophthalmologic diseases and obstructive sleep apnea: a systematic review and meta-analysis. Sleep Breath. 2016;20(4):1145-1154.
Lee YB, Koh JW, Hyon JY, et al. Sleep deprivation reduces tear secretion and impairs the tear film. Invest Ophthalmol Vis Sci. 2014;55(6):3525-3531.
Shi Y, Liu P, Guan J, et al. Association between glaucoma and obstructive sleep apnea syndrome: a meta-analysis and systematic review. PLoS One. 2015;10(2):e0115625.
Bilgin G. Normal-tension glaucoma and obstructive sleep apnea syndrome: a prospective study. BMC Ophthalmol. 2014;14:27.
Kiekens S, De Groot V, Coeckelbergh T, et al. Continuous positive airway pressure therapy is associated with an increase in intraocular pressure in obstructive sleep apnea. Invest Ophthalmol Vis Sci. 2008;49(3):934-940.
Hayirci E, Yagci A, Palamar M, et al. The effect of continuous positive airway pressure treatment for obstructive sleep apnea syndrome on the ocular surface. Cornea. 2012;31(6):604-608.
Daruich A, Matet A, Dirani A, et al. Central serous chorioretinopathy: recent findings and new physiopathology hypothesis. Prog Retin Eye Res. 2015;48:82-118. doi:10.1016/j.preteyeres.2015.05.003. PMID:26026923.
Stein JD, Kim DS, Mundy KM, et al. The association between glaucomatous and other causes of optic neuropathy and sleep apnea. Am J Ophthalmol. 2011;152(6):989-998.
Lavie L. Obstructive sleep apnoea syndrome — an oxidative stress disorder. Sleep Med Rev. 2003;7(1):35-51.
Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-545.
Chen HY, Chang YC, Lin CC, et al. Obstructive sleep apnea patients having surgery are less associated with glaucoma. J Ophthalmol. 2014;2014:838912.