Recurrent corneal erosion (RCE) is a disease in which the corneal epithelium repeatedly detaches spontaneously due to abnormalities in the adhesive structures formed between the corneal epithelium and the basement membrane1,2). Although the resulting epithelial erosion heals within a few days, it recurs after a certain period (ranging from 1 to 2 weeks to several months). It is a representative corneal disease that presents with recurrent eye pain and corneal epithelial damage, significantly impairing the patient’s quality of life5).
Attacks most often occur upon waking in the early morning. A characteristic feature is that subjective symptoms such as pain and foreign body sensation are disproportionately severe compared to the size of the erosion. When episodes recur frequently, the anxiety about recurrence can become a significant psychological stressor for the patient. Because onset often occurs after sleep, it may also lead to insomnia. Since it presents as unilateral recurrent keratitis, it is easily misdiagnosed as herpes simplex keratitis; therefore, a careful combination of history taking and clinical findings is key to diagnosis.
The most common cause is mechanical trauma, with tangential injuries from the edge of paper, fingernails, tree branches, the tip of mascara brushes, and similar objects serving as typical triggers. On the other hand, corneal dystrophies such as epithelial basement membrane dystrophy (EBMD) are also important causes, and metaherpetic keratitis, diabetic keratoepitheliopathy, and neurotrophic keratopathy can also be predisposing factors1,5).
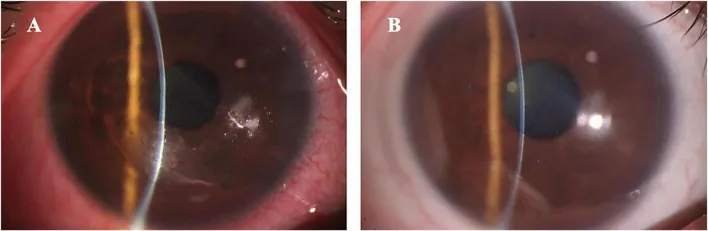
Yu X, et al. Photorefractive keratectomy with extended ablation zone for recurrent corneal erosion syndrome accompanied with refractive errors: a study of effectiveness, safety, and refractive outcomes. Front Med (Lausanne). 2025. Figure 2. PMCID: PMC12313699. License: CC BY.
A pair of slit-lamp anterior segment photographs; the left image shows irregularity of the corneal surface and conjunctival injection. These visually demonstrate the corneal epithelial abnormalities seen in recurrent corneal erosion, making them useful for explaining clinical findings.
Patients may also report a foreign-body sensation upon waking even between attacks, which has high diagnostic value. Because episodes frequently occur after sleep, they can cause insomnia and affect the patient’s daily life2,5).
QWhy do erosion attacks occur upon waking?
A
During sleep, the eyelids remain closed, which reduces tear production and brings the corneal epithelium into direct contact with the eyelid. The poorly adherent epithelium is easily dislodged by the opening and closing of the eyelids, with the initial opening of the eyes upon waking being a particular trigger. It is thought that the combination of overnight drying of the corneal surface and physical contact with the eyelid leads to erosion attacks upon waking.
Findings on slit-lamp microscopy range from normal to extensive epithelial defects2).
During attacks: Erosions are seen, most often in the central to inferior cornea. The epithelium surrounding the erosion appears edematous and opaque, indicating poor adhesion. Fluorescein staining clearly delineates the epithelial defect.
Between attacks: Microcysts (intraepithelial cysts) and subepithelial gray-white opacities may be observed. Findings such as an area that repels fluorescein stain may be noted, but sometimes no abnormality is found at all.
Location: The lower half of the cornea is most frequently affected. When there is a history of prior trauma, the erosion site tends to correspond to the previous injury site3).
When caused by corneal dystrophy: The findings tend to appear bilaterally and symmetrically1).
The location and size of the erosion are compared over time using corneal diagram documentation and photography.
Observations using in vivo confocal microscopy (IVCM) in traumatic RCE have reported deposits within basal epithelial cells, subepithelial microfolds and striae, damaged subepithelial nerves, abnormal basement membrane, and morphological changes in the anterior stroma4). These findings suggest microstructural changes underlying the clinical adhesion defect.
This is the most common cause1). Tangential trauma to the cornea from sharp objects such as the edge of paper, fingernails, tree branches, or the tip of mascara brushes often triggers the condition. Patients may not recall the traumatic event, and some cases present as vague complaints with an indolent course5).
The following corneal dystrophies can cause RCE1,2).
Epithelial basement membrane dystrophy (EBMD): Also known as Cogan dystrophy or map-dot-fingerprint dystrophy. It is the corneal dystrophy most strongly associated with RCE.
Reis-Bücklers corneal dystrophy: A TGFBI-related corneal dystrophy involving abnormalities of the Bowman layer.
QIf I have a corneal dystrophy, will I definitely develop RCE?
A
Not all patients with corneal dystrophy develop RCE. Epithelial basement membrane dystrophy (EBMD) is most strongly associated, but still accounts for only about 19–29% of RCE cases. The type and severity of corneal dystrophy, along with environmental factors, are involved in a complex manner.
Medical history: History of trauma, onset pattern upon waking, and family history of corneal dystrophy are important. Recurrent eye pain upon waking strongly suggests this disease.
Slit-lamp microscopy: Fluorescein staining is used to confirm epithelial defects. During non-attack periods, it is important not to overlook subtle findings such as microcysts and subepithelial opacities.
Erosion evaluation: Objectively record the location and size of the erosion using corneal diagrams or anterior segment photographs.
Sensory testing: Check corneal sensitivity for differential diagnosis.
IVCM: In refractory or atypical cases, it may be useful for evaluating the adhesion complex4).
Treatment of RCE is performed in a stepwise manner. In the acute phase, the goal is to promote healing of the erosion, and thereafter the main goal is prevention of recurrence2,5,11).
Artificial tears and ophthalmic ointment: The standard prescription combines 0.1% sodium hyaluronate eye drops 4 times daily with bedtime application of ofloxacin ophthalmic ointment (0.3%).
Eye patch and cycloplegic agents: In the acute phase, topical cycloplegics combined with temporary eye patching promote ocular surface healing2).
Antibiotics: Topical antibiotics are prescribed to prevent infection of the epithelial defect.
Bedtime ophthalmic ointment: Continue for at least 3 months, preferably 6 months, even after erosion episodes resolve. Patients are advised to instill artificial tears immediately upon waking and keep the eye drop bottle by the bedside.
Hypertonic saline: 5% sodium chloride eye drops or ointment are used. Bedtime application has been reported effective for both the acute and chronic phases2).
Therapeutic contact lenses: Continuous wear promotes epithelial stabilization. In a report of 12 cases with 3 months of continuous wear, 9 cases (75%) showed no recurrence at approximately 1-year follow-up7).
Punctal occlusion: Considered when dry eye is present. Options include temporary occlusion with collagen plugs or permanent occlusion with silicone plugs2).
Added when conservative treatment is insufficient.
Doxycycline: Has matrix metalloproteinase-9 (MMP-9) inhibitory activity. Administered orally at 50 mg twice daily for approximately 2 months, in combination with topical corticosteroid eye drops (1% methylprednisolone, 1% prednisolone acetate, or 0.1% fluorometholone) 3 times daily for 2–3 weeks. In the report by Dursun et al., pain and epithelial defects improved within 2–10 days after starting treatment, and no recurrence was observed during an average follow-up of 21.9 months8)
Topical cyclosporine 0.05%: A small case series has reported a reduction in recurrent episodes2)
Autologous serum eye drops: Positioned as one of the second-line therapies for cases where lubricants or eye patching are insufficient2)
Indicated for refractory cases that do not respond to conservative treatment.
Surgical Treatment Options
Epithelial debridement: Removes poorly adherent epithelium with a cotton swab or cellulose sponge to expose the smooth surface of Bowman’s layer. Thereafter, a therapeutic soft contact lens and topical antibiotics are used in combination6)
Anterior stromal puncture (ASP): Using a 25-gauge fine needle, micro-punctures are made into the superficial stroma after debridement under a slit-lamp microscope. The needle tip is slightly bent to prevent perforation. Since puncture sites leave punctate opacities, the pupillary area should be avoided. In a retrospective study by Zauberman et al. (30 cases, 35 eyes), 62.9% of eyes became symptom-free after a single treatment, and erosion episodes became milder in 37.1%9)
Diamond bar polishing: After epithelial removal, the Bowman layer is polished with a diamond bar to improve epithelial adhesion. A therapeutic contact lens is worn for 4–5 days after the procedure2)
PTK (phototherapeutic keratectomy): The cornea is ablated uniformly to a depth of 5–7 μm using an excimer laser. In the report by O’Brart et al., no recurrence was observed in 13 of 17 eyes at the final follow-up10). There is a risk of hyperopic shift, and available facilities are limited.
A non-contact puncture method using an Nd:YAG laser (0.4–0.5 mJ pulses) has also been reported for anterior stromal puncture2). Since puncture sites may cause scar formation, application to the pupillary area should be avoided with any technique.
QWhat is anterior stromal puncture?
A
This is a procedure in which micro-punctures are made in the superficial layer of the corneal stroma at the site of epithelial defects using a 25-gauge fine needle. It can be performed under topical anesthesia using a slit-lamp microscope. The punctures induce a fibrocystic reaction and wound healing, strengthening the adhesion between the epithelium and the corneal stroma. It is effective in approximately 63% of cases after a single treatment, but punctate opacities remain at the puncture sites, so application over the pupillary area should be avoided.
QHow long should prophylactic treatment be continued?
A
Continue bedtime eye ointment and artificial tears immediately after waking for at least 3 months, preferably 6 months, after erosion episodes have resolved. In some cases, erosion episodes may recur even after more than a year, so continuation for a sufficient period is important.
A 2018 Cochrane review on the management of RCE exists, but the 10 included RCTs (total 505 cases) have limitations in size and quality and have not established a definitive treatment algorithm11). In clinical practice, a stepwise approach starting with conservative treatment and considering surgical treatment for refractory cases is common.
Normal corneal epithelium adheres to the basement membrane via hemidesmosomes of basal cells1,2). The basement membrane is mainly composed of type IV collagen and laminin, and is connected to the underlying Bowman’s layer and stroma by anchoring fibrils (type VII collagen). Cell-cell and cell-matrix interactions via the fibronectin-integrin system play an important role in maintaining the adhesion structure.
In RCE, adhesion of the epithelium to the underlying stroma after initial injury becomes incomplete and unstable1). Pathologically, disruption or loss of the basement membrane and a decrease in hemidesmosomes, the adhesion mechanism of basal cells, are observed.
In post-traumatic RCE, reconstruction of the normal adhesion structure is impaired for some reason. Tangential trauma from paper or fingernails damages not only the epithelium but also the adhesion mechanism near Bowman’s layer, and it is believed that sufficient anchoring fibrils do not regenerate during the healing process5). In contrast, in RCE associated with corneal dystrophy, the adhesion structure itself is fragile due to genetic abnormalities in the constituent protein components.
IVCM observation of traumatic RCE has revealed detailed findings including adhesion complex defects, deposits within basal epithelial cells, subepithelial microfolds, subepithelial nerve damage, abnormal basement membrane, and anterior stromal morphological changes4). These findings reflect complex microstructural abnormalities involving not just epithelial detachment but the basement membrane, Bowman’s layer, and anterior stroma.
In patients with meibomian gland dysfunction (MGD), ocular rosacea, and recurrent erosion, elevated levels of toxic free fatty acids, interleukin-1 (IL-1), and matrix metalloproteinase-9 (MMP-9) have been reported2). These molecules degrade adhesion complexes and inhibit basement membrane formation.
Both doxycycline and topical steroids reduce MMP-9 levels and activity in cultured human corneal epithelium. Inhibition of MMP-9 is thought to suppress the degradation of collagen and hemidesmosomes, thereby contributing to the stabilization of epithelial adhesion mechanisms8).
During nighttime sleep, eyelid closure reduces tear production, causing the epithelium and palpebral conjunctiva to adhere tightly. In areas where adhesion is weak, the mechanical stress of opening the eyelids upon waking readily causes epithelial detachment. This mechanism explains why RCE attacks predominantly occur in the early morning upon awakening2,5).
RCE is fundamentally a disease with a strong tendency toward spontaneous healing2). However, to consider it healed, an attack-free period of at least 3 months, and preferably 6 months, is required. Erosion attacks may recur even after more than a year has passed, so it is important to repeatedly explain the risk of recurrence to the patient.
Some cases relapse as soon as treatment is discontinued. Particularly when trauma is the cause, complete reconstruction of adhesive structures takes several months to half a year or more, so patients need motivation to continue prophylactic eye drops even after symptoms resolve. To prevent patients from deciding on their own that they are cured and stopping treatment, explaining the prospect of long-term therapy from the initial visit directly helps reduce recurrence.
Complications include corneal opacity and scar formation, infectious keratitis associated with therapeutic contact lens use or long-term steroid use, and reduced visual acuity2). Since the prognosis is extremely favorable with appropriate treatment and prompt diagnosis, it is advisable to educate patients with risk factors to seek medical attention promptly when symptoms appear.
Farid M, Rhee MK, Akpek EK, Amescua G, Garcia-Ferrer FJ, Lin A, et al. Corneal Edema and Opacification Preferred Practice Pattern®. Ophthalmology. 2019;126(1):P216-P285. doi:10.1016/j.ophtha.2018.10.022. PMID:30366795.
Fraunfelder FW, Cabezas M. Treatment of recurrent corneal erosion by extended-wear bandage contact lens. Cornea. 2011;30(2):164-166. PMID: 20847650.
Dursun D, Kim MC, Solomon A, Pflugfelder SC. Treatment of recalcitrant recurrent corneal erosions with inhibitors of matrix metalloproteinase-9, doxycycline and corticosteroids. Am J Ophthalmol. 2001;132(1):8-13. PMID: 11438047.
Zauberman NA, Artornsombudh P, Elbaz U, Goldich Y, Rootman DS, Chan CC. Anterior stromal puncture for the treatment of recurrent corneal erosion syndrome: patient clinical features and outcomes. Am J Ophthalmol. 2014;157(2):273-279.e1. PMID: 24439438.
O’Brart DP, Muir MG, Marshall J. Phototherapeutic keratectomy for recurrent corneal erosions. Eye (Lond). 1994;8(Pt 4):378-383. PMID: 7821455.
Watson SL, Leung V. Interventions for recurrent corneal erosions. Cochrane Database Syst Rev. 2018;7(7):CD001861. PMID: 29985545.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.